Beliefs, Experiences, and Attitudes toward the Mediterranean Diet in Coronary Artery Bypass Graft Surgery Patients
Abstract
The Mediterranean Diet (MD) can be used for treatment, primary, and secondary prevention of coronary heart disease. This cross-sectional, observational study completed on cardiac patients recovering from Coronary Artery Bypass Graft (CABG) surgery provides a comprehensive picture of this population. We assessed the demographic and lifestyle characteristics of this population. Additionally, we assessed beliefs, experiences, and attitudes toward the MD. The majority (74%) of CABG patients were males, Caucasian, college educated, married, overweight, physically inactive, and formers mokers. Their average age was 67 ± 9 years. They are rather poorly informed regarding the MD, with limited experience using the MD. Their average adherence to the MD was 48%. Few believe the MD is hard to follow, but they are willing to change their diet so that it would more adhere to the principles of MD. They also believe eating more fruits and vegetables, nuts, and red wine in moderation is healthy. The results for females were similar to the one for males. The theoretical model seems to indicate that in our population of post CABG patients, physically active patients, who had experience with Mediterranean lifestyle would be willing to adhere to the MD. Achieved education was a contributing factor for the interest in MD.
Keywords
Mediterranean diet, CABG (Coronary Artery Bypass Graft), Lifestyle, Attitudes, Beliefs
Introduction
Heart disease is the number one cause of death worldwide. About 655,000 Americans die from heart disease each year [1]. Coronary Artery Bypass Graft (CABG) has been used for the treatment of coronary artery disease (CAD) for nearly 50 years and has been performed on millions of people worldwide. Approximately 510,000 CABG surgeries are performed annually in the USA [1].
The traditional Mediterranean diet (MD) is characterized by a high intake of olive oil, fruit, nuts, vegetables, and cereals; a moderate intake of fish and poultry; a low intake of dairy products, red meat, processed meats, and sweets; and wine in moderation, consumed with meals [2]. A systematic review ranked the MD as the most likely dietary model to provide protection against coronary heart disease (CHD) [3]. Traditional MD can be used for primary and secondary prevention of cardiovascular disease [4,5]. However, most of the research was conducted in countries around the Mediterranean Sea. Yang, et al. reported that greater adherence to MD in a North American population reduced metabolic syndrome, weight, LDL cholesterol, and improved HDL cholesterol levels [6].
Little is known about the impact of lifestyle changes, including diet and exercise, on long-term outcomes in patients who have had CABG surgery. Current evidence indicates diet and exercise interventions are effective in the short-term, but intervention effects fade over time [7]. Further research is needed with more rigorous designs to define optimal management regimens and prevention strategies [8,9].
Research regarding attitudes and food choice behavior discovered that taste is the major determinant for food choices. The rapid growth of olive oil consumption in the UK was often attributed to healthy eating and avoidance of saturated fats. However, when studied, this does not seem to be the main determinant for usage. The attributes most strongly correlated with the intention to use olive oil were those regarding improvement to the taste of both salads and cooked meals. For olive oil users, health considerations were only a secondary factor [10].
For Americans who wish to improve their diet, MD is an attractive dietary pattern famous for palatability and health benefits [2]. For post CABG patients, adoption of MD provides an appealing, palatable secondary prevention of CAD strategy. Although there has been an increased interest in MD overtime, it is not clear what the attitudes are toward MD in the post CABG patient’s population. Therefore, the focus of our study was to examine the beliefs, experiences and attitudes toward MD and develop a theoretical model of the relationships between health behaviors (smoking, exercise), attitudes toward MD, BMI, education, gender, experiences with MD, and adherence to MD.
Materials and Methods
Recruitment of subjects
This cross-sectional, observation study was completed at Lovelace Heart Hospital in Albuquerque, New Mexico. The study was approved by the University of New Mexico Office of the Institutional Review Board (IRB protocol # 10816). Post CABG patients admitted to the cardiac Intensive Care Unit (ICU) were recruited by a research dietitian for study participation. On day three post-surgery, patients were surveyed for coherence. If coherent, the research dietitian proceeded with the consent and administration of the health survey. The research dietitian read all questions to the patients and marked or circled the answers. The data collection time averaged 20 minutes per patient.
Assessment of beliefs, experiences, and attitudes toward the Mediterranean diet
The health survey was divided into five sections. The first section ascertained basic demographic information including: gender, race/ethnicity, education, marital status, self-reported weight, self-reported height, age, and smoking status.
The second section of the survey evaluated patient physical activity using a validated self-reported Godin-Shephard leisure physical activity questionnaire [11]. Participants were asked how frequently they engaged in strenuous, moderate, or mild exercise per week. The weekly frequencies of strenuous, moderate, and mild activities were then multiplied by nine, five and three, respectively; these three values corresponded to the Metabolic Equivalent (MET) value categories of the physical activities listed. The total weekly leisure activity score was then calculated. Three classes of physical activity were defined: > 24 METs/week - active, 14-23 METs/week - moderately active, and < 14 METs/week - insufficiently active.
The third section of the survey was a validated food frequency questionnaire (FFQ) that evaluated adherence to the Mediterranean dietary pattern [12]. Food components of the MD were listed, and patients were asked how many times per week they consumed these foods. Alcohol consumption was also measured. The FFQ was then used to compute a diet score in the range between 0-55. Five classes of the distribution of the diet score have been developed: 0-11 poor adherence, 12-22 fair adherence, 23-34 good adherence, 35-44 very good adherence, and 45-55 excellent adherence. Using the highest category (i.e., 45-55) as comparison if someone had the score between 0-11 (i.e., away from the Mediterranean dietary pattern) his OR of having CHD was 2.17 higher, for the score of 12-22 the OR was 1.63 higher, for the score of 23-34 the OR was 1.42 higher and for the score of 35-44 the OR was almost 1, similar to the excellent adherence.
The fourth section of the survey ascertained the experience with the MD using four simple yes or no questions. This section was preceded with a short explanation of what the MD is: “The Mediterranean diet is a healthy eating plan traditionally followed in Greece, France, and Italy that emphasizes fruits and vegetables, nuts, grains, olive oil (as opposed to butter), grilled or steamed chicken and seafood (as opposed to red meat) and drinking red wine in moderation.” Patients were asked if they had ever heard of the MD, tried to follow the MD, knew a family member or friend who follow MD. The last question assessed whether they believe that following MD is hard.
In the last section of the survey, the patients were asked ten agree or disagree questions regarding their attitudes toward the MD. The questions were meant to provoke answers and determine their attitude or willingness to adhere to MD. Examples of questions are e.g., the Mediterranean diet is very restrictive; I could eat fish once a week; Mediterranean diet should be only eaten in Greece, France, and Italy; or it is healthy to eat a handful of nuts every day.
Statistical analysis
The data was analyzed using SPSS (version 24.0; SPSS, Inc., Chicago, IL, USA) for descriptive statistics (mean, standard deviation) and inferential statistics (T-test, Chi-square) and AMOS 21.0 statistical software for Structural Equation Modeling (SEM). SEM is a multivariate statistical method used in social sciences, and in health behavior research. SEM examines underlying relationships among variables in a conceptual model and helps to explain social or behavioral phenomena [13]. We performed descriptive statistics and measures of internal consistency on relevant variables before model testing. Model indicators to determine the best-fit model were based on theoretical as well as statistical [Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), p of Close Fit (PCLOSE) and Holter’s M] judgments. P values less than or equal to 0.05 were considered statistically significant.
Results
Demographics
Overall, there were 90 participants who completed the survey. Descriptive demographic data are shown in Table 1. Majority of the participants (74.4%) were male and Caucasian (62.7% of males and 52.2% of females). Majority of males (46.3%) had college education while most females (52.2%) had high school education. Majority of the participants were married (71.6% of males and 60.9% of females). The mean age was 67.3 years for males and 66.3 years for females.
Lifestyle characteristics
Table 2 shows the lifestyle characteristics of the study population. Most males (44.8%) and females (39.1%) were overweight. However, the second most common BMI category in males was obese (22.4%), but normal weight (30.4%) in females. Majority of participants were physically inactive (68.7% of males and 82.6% of females), never or rarely engaging in a physical activity enough to increase heartbeat or work up sweat (67.2% of males and 73.9% of females). Only 9% of males and females were current smokers. Non-smokers and former smokers were equally distributed in males (44.8% non-smokers and 46.3% former smokers), however in females the non-smoking category (52.2%) was the largest, followed by former smoker category (36.1%). The mean duration of smoking was 28 years for males and 22.9 years for females.
Assessment of adherence to the Mediterranean diet
We used a validated FFQ [16] to assess the adherence of the participants to the MD. Nobody achieved excellent adherence to the MD (Table 3). Three males (4.5%) achieved a very good score meaning that their average adherence to the MD was 69% and their OR of having CHD was 1.00 in comparison to someone in the excellent adherence category. Most males (61.2%) and females (60.9%) reported good adherence to the MD, which would put their OR of having CHD 1.42 higher than someone in the excellent adherence category. The average adherence to the MD in males in the good category was 48%, in females 50%. The second most frequently reported adherence category was fair (32.8% of males and 39.1% of females), which would put their OR of having CHD 1.63 higher than someone in the excellent adherence category. Their average adherence to the MD was 35% for males and 37% for females. There was only one male with poor adherence to the MD, his OR of having CHD was 2.17 higher than some in the excellent adherence category, and his adherence to the MD was 20%.
Assessment of experiences with the Mediterranean diet
Table 4 shows the experiences our population had with the MD, 28.4% of males and 47.8% of females never heard of the MD. Only 10.4% of males and 4.3% of females have ever tried to follow the MD. Only a small portion of participants (16.4% of males and 26.1% of females) know a family member or friend who follows MD. Some participants (20.9% of males and 13.0% of females) believe that the MD is hard to follow.
Assessment of attitudes toward the Mediterranean diet
\Table 5 shows the distribution of attitudes toward MD by gender. Males (41.8%) and females (39.1%) equally felt that MD is a very restrictive diet. But the majority of participants (males 70.1% and females 73.9%) also felt that it would be easy for them or their family to follow the MD. Absolute majority of the participants felt that they could eat fish once a week (males 91.0% and females 82.6%) and that eating a handful of nuts every day is a healthy habit (males 91.0% and females 95.7%). A sizable portion of participants felt that the MD is a popular diet (males 22.4% and females 43.5%). Majority of participants felt that they could eat less beef and pork (males 86.6% and females 91.3%) and that eating more fruits and vegetables is a healthy habit (males 98.5% and females 100.0%). Only 7.5% of males and 4.3% of females felt that the MD should be only eaten in Greece, France, and Italy. Males (74.6%) and females (73.9%) equally felt that drinking red wine in moderation is good for your heart. Lastly, a majority of participants felt that it is easy to cook with olive oil instead of butter (males 85.1% and females 73.9%).
Theoretical model of the relationships between smoking behavior, attitudes toward MD, BMI, education, gender, experiences with MD, physical activity, and adherence to MD
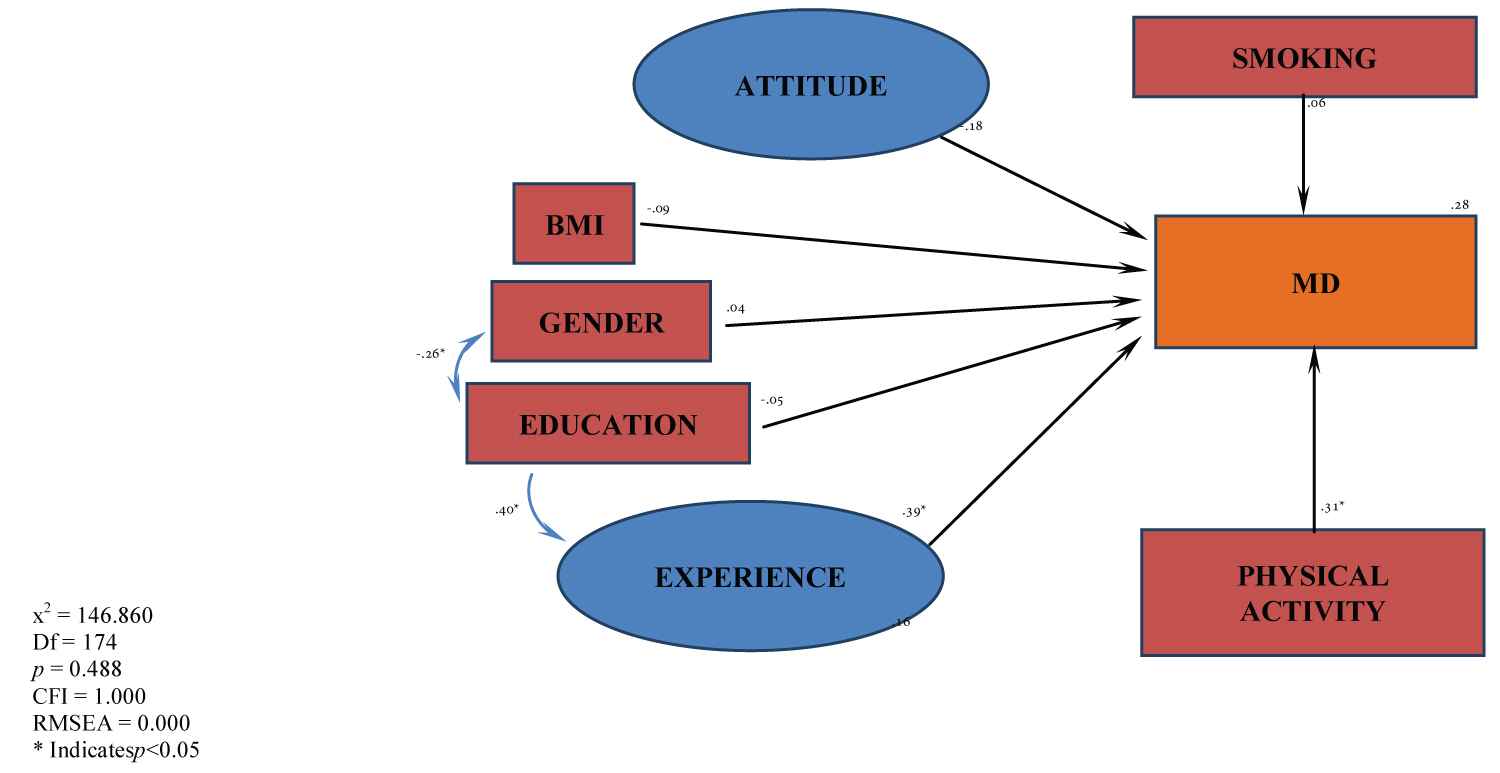
The purpose of this study was to test the predictive role of attitudes, beliefs, and experiences with MD, smoking, BMI, level of physical activity, gender, and educational level as predictors of adherence to the MD. SEM technique was used to test the fit of the theoretical model described in Figure 1 using IBM SPSS Amos version 21.0.
Our model is a mixed combination of two latent variables and five observed exogenous variables as predictors of one observed endogenous variable (adherence to MD). A non-significant Chi Square of 146.860 (Df = 147, p = 0.488) with a Chi Square/Df ratio of 0.999, RMSEA = 0.000, High 90 = 0.05, and PCLOSE = 0.952 suggests that the model is viable. The Holter’s M 0.01 = 74 (for the independence model) suggests that the sample size is acceptable.
Analysis of the estimates shows that Smoking (β = 0.06), Attitude toward MD (β = -0.18), BMI (β = -0.09), Gender (β = 0.04), Education (β = -0.05), Experience with MD (β = 0.39), and level of Physical activity (β = 0.31), are predictors of 28% of the variance of adherence to MD as it is explained by the theoretical model. Additionally significant bivariate correlation was found between Education and Gender (r = -0.26). Education is a significant predictor of 16% of the variance of Experience with MD (β = 0.40).
The model seems to indicate that in our population of post CABG patients, physically active patients, who had experience with Mediterranean life style would be willing to adhere to the MD. Achieved education was a contributing factor for the interest in MD.
Discussion
The results from this cross-sectional, observational study completed on cardiac patients recovering from CABG surgery provide a comprehensive picture of this population. Majority (74%) of CABG patients are males, Caucasian, college educated, married, overweight, physically inactive, and former smokers. Their average age was 67 years. Their present diet is only 48% similar to the MD and because of this they have higher risk of having CHD. They are poorly informed regarding the MD, with limited experience with the MD. However, only minority believes the MD is hard to follow. They are willing to consume more fish and less beef and pork; cook on olive oil instead of butter. They also believe eating more fruits and vegetables, nuts and red wine in moderation is healthy. Minority (26%) of CABG patients are females, Caucasian, high school educated, married, overweight, physically inactive, and non-smoker. They are on average 66-years-old. Their present diet is 50% similar to the MD and because of this they have higher risk of having CHD. They are also poorly informed regarding the MD, with very limited experience with the MD. Though, only very small minority believes MD is hard to follow. They are willing to consume more fish and less beef and pork; cook with olive oil instead of butter. They believe eating more fruits and vegetables, nuts and red wine in moderation is healthy.
To embrace healthy lifestyle-change after CABG surgery represents a significant advantage for the patient as well as the US health care system. The surgeons performed approximately 510,000 CABG surgeries in the US at the average operation cost $86,914. This represents $34 billion per year [1]. Despite the expense of the CABG surgery, 30-50% of bypass grafts reocclude after 5-7 years [14]. When this happens, the bypass surgery is often repeated, incurring additional cost. The idea that CHD is reversible by comprehensive lifestyle change was once a radical concept, however now it has become mainstream [15]. A number of lifestyle programs developed by Dean Ornish [16,17], John McDougall [18,19] and Hans Diehl [20-22] have shown to arrest or reverse the progression of coronary atherosclerosis on short term and long-term basis. However, it is not known how many patients with CHD would be interested to make such comprehensive lifestyle changes to avoid revascularization surgery. Critics of these comprehensive lifestyle programs often mark them as too restrictive.
Presently at Lovelace Heart hospital, education used by dietitians for patients after CABG surgery is the Therapeutic Lifestyle Changes (TLC) Diet from the Academy of Nutrition and Dietetics Nutrition Manual. This diet is very similar in recommendations to the MD, but maybe lacks the “name recognition” associated with MD. A persuasive body of evidence from observational studies has documented that Mediterranean-style diets are associated with a substantially reduced risk of cardiovascular disease [23]. Of particular interest should also be the very high palatability of MD.
To our knowledge, the present study is first one to methodologically examine the post CABG population using such sophisticated tools as SEM. There is agreement within the research community [7] that much more focus on diet and exercise for the CABG surgery population is necessary. Presently most of the focus is on medication adherence and tobacco cessation. However, both diet and exercise modifications can significantly influence prevention of re-occlusion after CABG. Heart disease affects many aspects of women’s lives. Women with heart disease have poorer medical outcomes than men [24]. There is dearth of research regarding CHD in females. Our study included both genders and provides in depth descriptive and multivariate statistics how males and females would be willing to change their lifestyles and consider MD as one possible option.
One of the major findings of our study is that physically active patients, who had experience with Mediterranean lifestyle would be willing to adhere to the MD. Achieved education was a contributing factor for the interest in MD. Although the majority of our CABG patients (74%) were men, their spouses are often present and very involved in the nutrition education. Women are often the ones who cook at home and do the grocery shopping. It seems that targeted nutrition education regarding MD toward women would be beneficial and help the whole family.
Several potential limitations to this study should be considered. This is a population-based cross-sectional study, which included both genders and all age groups. The study was conducted in New Mexico, which may limit the generalizability of the results for the whole US population. Although the sample size of the population was large enough, some groups may be underrepresented. The data was collected the third day following a successful CABG surgery, reflecting the state of mind of the participants at that time point in their life. Although SEM is a sophisticated analytic tool for testing theoretical models in behavioral or social science, the analyses are correlational which makes it difficult to establish causality. Because the isolation of variables in the model are impossible, all models must be looked at only as estimation of reality [25]. The strengths of our study are large sample size, no missing data, and a diverse study population.
Conclusions
Results from this cross-sectional, observational study show great similarities in males and females in demographic characteristics, lifestyle variables, adherence to MD, and experiences and attitudes toward MD. Post CABG surgery patients of both genders seem to be willing to change their lifestyle and consider MD as one option. Our theoretical model seems to indicate that physically active patients, who had experience with Mediterranean lifestyle would be willing to adhere to the MD. Achieved education was a contributing factor for the interest in MD.
Author Contributions
Conceptualization, D.M.C. and P.P.; Data curation, D.M.C; Formal analysis, P.P. and T.G.; Funding acquisition, P.P.; Investigation, D.M.C; Methodology, P.P.; Project administration, P.P.; Supervision, P.P. and D.P-G.; Validation, P.P.; Visualization, D.M.C; Writing – original draft, D.M.C and P.P.; Writing – review & editing, D.M.C, P.P., D.P-G., and T.G.
Funding
The present study was supported in part from the USDA National Institute of Food and Agriculture, HSI Collaboration: Integrating Food Science/Engineering and Education Network (IFSEEN; Award # 2015-38422-24059).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the University of New Mexico Office of the Institutional Review Board (IRB protocol # 10816).
Informed Consent Statement: Informed consent was obtained from all patients involved in the study.
Acknowledgments
We would like to express our gratitude to all participants for their willingness to partake in this research. We would like to thank Cyndi Silva, Heather Brads, and Leah Maus - dietitians at the Lovelace Heart Hospital of New Mexico for their support and technical assistance. We would like to also thank to Dr. Kevin Rosenberg, the lead hospitalist at the Love-lace Heart Hospital of New Mexico for his help and support. The study was conceived and carried out as part of the requirement for the Master Degree in Nutrition at the University of New Mexico. Soli Deo Gloria.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Virani SS, Alvaro A, Benjamin EJ, et al. (2020) Heart disease and stroke statistics-2020 update: A report from the American Heart Association. Circulation 141: e139-e596.
- Willett WC, Sacks F, Trichopoulou A, et al. (1995) Mediterranean diet pyramid: A cultural model for healthy eating. Am J Clin Nutr 61: 1402S-1406S.
- Mente A, de Koning L, Shannon HS, et al. (2009) A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Inter Med 169: 659-669.
- Estruch R, Ros E, Salas-Salvadó J, et al. (2018) Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med 378: e34.
- Widmer RJ, Flammer AJ, Lerman LO, et al. (2015) The Mediterranean diet, its components, and cardiovascular disease. Am J Med 128: 229-238.
- Yang J, Farioli A, Korre M, et al. (2014) Modified Mediterranean diet score and cardiovascular risk in a North American working population. PLos One 9: e87539.
- Coyan GN, Reeder KM, Vacek JL, et al. (2014) Diet and exercise interventions following coronary artery bypass graft surgery: A review and call to action. Phys Sportsmed 42: 119-129.
- Hartwell D, Henry J (2003) Dietary advice for patients undergoing coronary artery bypass surgery: falling on deaf ears? Int J Food Sci Nutr 54: 37-47.
- Vachenauer R, Drünenfelder J, Plass A, et al. (2008) Changing lifestyle habits as secondary prophylaxis after coronary artery bypass grafting. Heart Surg Forum 11: e243-e247.
- Thompson KE, Haziris N, Alekos PJ (1994) Attitudes and food choice behavior. Br Food J 96: 9-13.
- Godin G, Shephard RJ (1985) A simple method to assess exercise behavior in the community. Can J Appl Sport Sci 10: 141-146.
- Panagiotakos DB, Milias GA, Pitsavos C, et al. (2006) MedDiet Score: A computer program that evaluates the adherence to the Mediterranean dietary pattern and its relation to cardiovascular disease risk. Comput Methods Programs Biomed 83: 73-77.
- Buhi ER, Goodson P, Neilands TB (2007) Structural equation modeling: A primer for health behavior researchers. Am J Health Behav 31: 74-85.
- Bourassa MG (1994) Long-term vein graft patency. Curr Opin Cardiol 9: 685-691.
- Ornish D (1998) Avoiding revascularization with lifestyle changes: The Multicenter Lifestyle Demonstration Project. Am J Card 82: 72-76.
- Ornish D, Brown SE, Scherwitz LW, et al. (1990) Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet 336: 129-133.
- Ornish D, Schwewitz LW, Billings JH, et al. (1998) Intensive lifestyle changes for reversal of coronary heart disease. JAMA 280: 2001-2007.
- Mc Dougall J, Thomas LE, McDougall C, et al. (2014) Effects of 7 days on an ad libitum low-fat vegan diet: The McDougall Program cohort. Nutr J 13: 99.
- Mc Dougall J, Litzau E, Saunders V, et al. (1995) Rapid reduction of serum cholesterol and blood pressure by a twelve-day, very low fat, strictly vegetarian diet. J Am Coll Nutr 14: 491-496.
- Kent L, Morton D, Hurlow T, et al. (2013) Long-term effectiveness of the community-based Complete Health Improvement Program (CHIP) lifestyle intervention: A cohort study. BMJ Open 3: e003751.
- Ken LM, Morton DP, Rankin PM, et al. (2014) Gender differences in effectiveness of the Complete Health Improvement Program (CHIP) lifestyle intervention: An Australasian study. Health Promot J Austr 25: 222-229.
- Wennehorst K, Mildenstein K, Saliger B, et al. (2016) A comprehensive lifestyle intervention to prevent Type 2 Diabetes and cardiovascular diseases: The German CHIP Trial. Prev Sci 17: 386-397.
- Sofi F, Abbate R, Gensini GF, et al. (2010) Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am J Clin Nutr 92: 1189-1196.
- Marcuccio E, Loving N, Bennet SK, et al. (2003) A survey of attitudes and experiences of women with heart disease. Women's Health Issues 13: 23-31.
- Bollen KA (2009) Structural equations with latent variables. John Wiley & Sons, New York, USA, 319-393.
Corresponding Author
Peter Pribis, Department of Individual, Family & Community Education, Nutrition & Dietetics Program, College of Education & Human Sciences, University of New Mexico, Hokona Zuni 157, MSC05 3042, Albuquerque, NM 87131, USA.
Copyright
© 2023 Crowley DM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.