Optimising Screw Trajectory in the Bristow-Latarjet Procedure: A Simple Technique to Improve the Alpha Angle
Structured Abstract
Introduction: Screw entry point and trajectory (the alpha angle) are essential to ensure appropriate graft position in the Bristow Latarjet procedure. A high alpha angle may occur in patients with a large soft tissue envelope, where adequate medial positioning of the drill and guide can be challenging. This study investigated the effect of using a longer drill bit and soft tissue guide during the procedure to improve the starting position and drill trajectory and whether this can result in improved postoperative screw alpha angle.
Material and methods: 66 consecutive Latarjet procedures between January 2013 and August 2017 were separated into two groups. In group one (Standard drill) the screw holes were created using the standard length 3.2 mm AO large fragment drill bit and 3.2/4.5 mm double drill sleeve (Synthes, Paoli, PA, USA). For the patients in group two (Long drill) the 3.2 mm percutaneous drill bit (300 mm) with a longer 4.3 mm drill sleeve (Synthes, Paoli, PA, USA) was utilised. The postoperative Bernageau radiographs were assessed independently by two observers to record each screw alpha angle.
Results: There was a significant difference in average screw angle between both groups studied (5.8 ± 1.7 versus 2.1 ± 0.8, P = 0.037). There was excellent reliability (all correlations > 0.93) for both intra-observer and inter-observer measurements of screw angles.
Discussion: The use of a longer drill bit and guide allowed optimal positioning of the drill during screw hole preparation in the Latarjet procedure. This simple technique modification is cheap and easy to add to any surgeons practice and may offer benefit to patients.
Keywords
Latarjet procedure, Shoulder instability, Shoulder stabilisation
Introduction
Dr. Michel Latarjet first described his coracoid transfer procedure for shoulder stabilization in 1954 [1,2]. The Latarjet procedure is effective in reducing instability in patients with significant bone loss but does incur greater risk of complication when compared to standard soft tissue stabilisation procedures (Bankart repair) [3-6]. Hardware related problems are common, especially if the screw start point or trajectory are incorrect which results in poor bone graft position. Developing a safe and reproducible technique is important to ensure correct graft placement, encourage graft healing and minimize complications related to the screws [7]. The ideal angle of screw insertion is believed to be parallel to the glenoid articular surface, to help improve graft union, avoid suprascapular nerve injury and most importantly to avoid a lateralized graft and prominent hardware [5,8,9]. Despite the acceptance of screw trajectory as the key to a good graft position, in practice this remains challenging especially in larger, muscled athletes where adequate medial positioning the drill and guide are difficult. The senior author made a simple change from an established technique using standard large fragment instrumentation to a longer drill bit and a longer, more robust drill sleeve. It was felt that this adjustment was technically easier, and this study aimed to ascertain if there was an objective improvement in Latarjet screw alpha angle.
Material and Methods
No institutional ethics approval was necessary as this study involved review of existing deidentified patient data and description of technique only.
Drill bit and guide
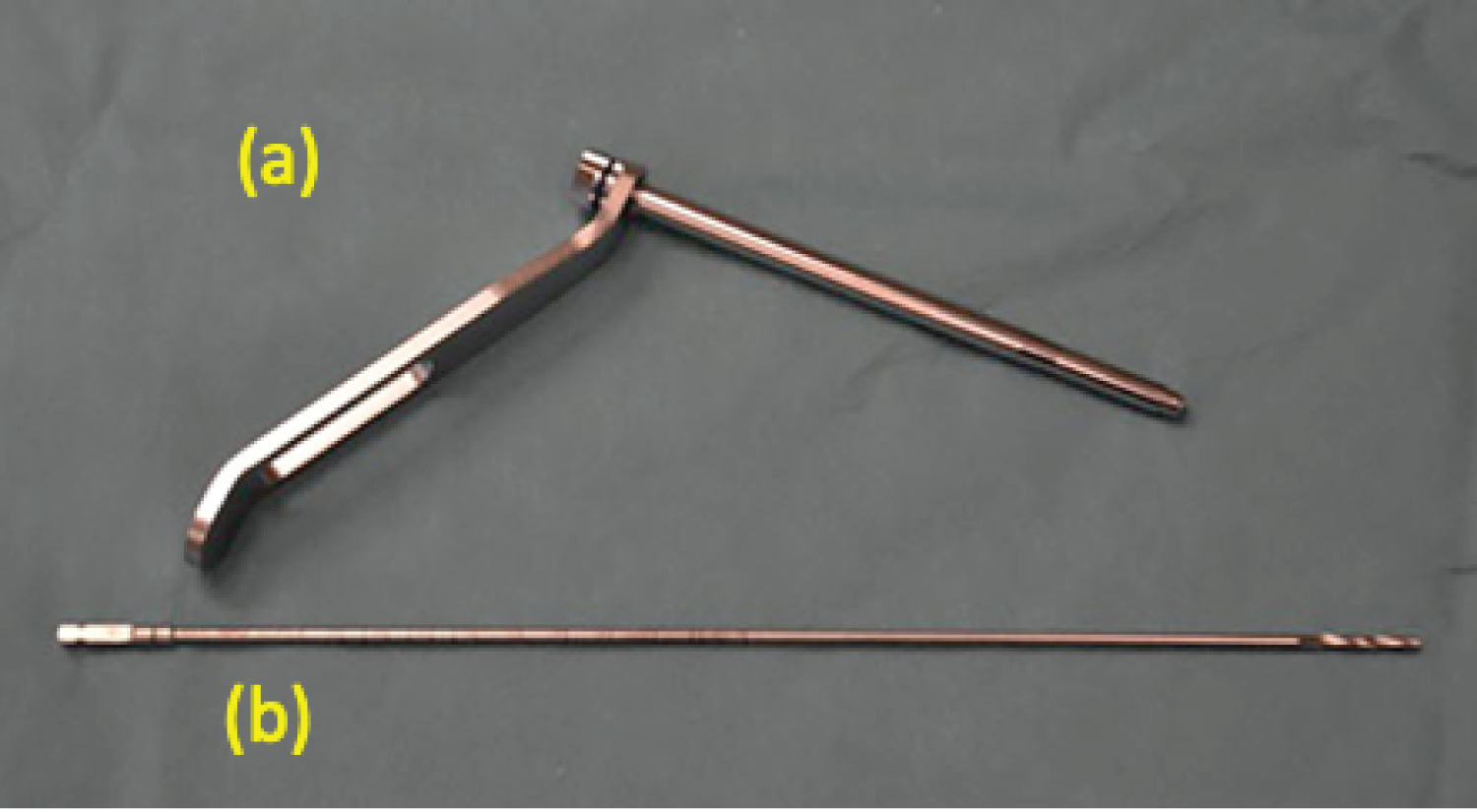
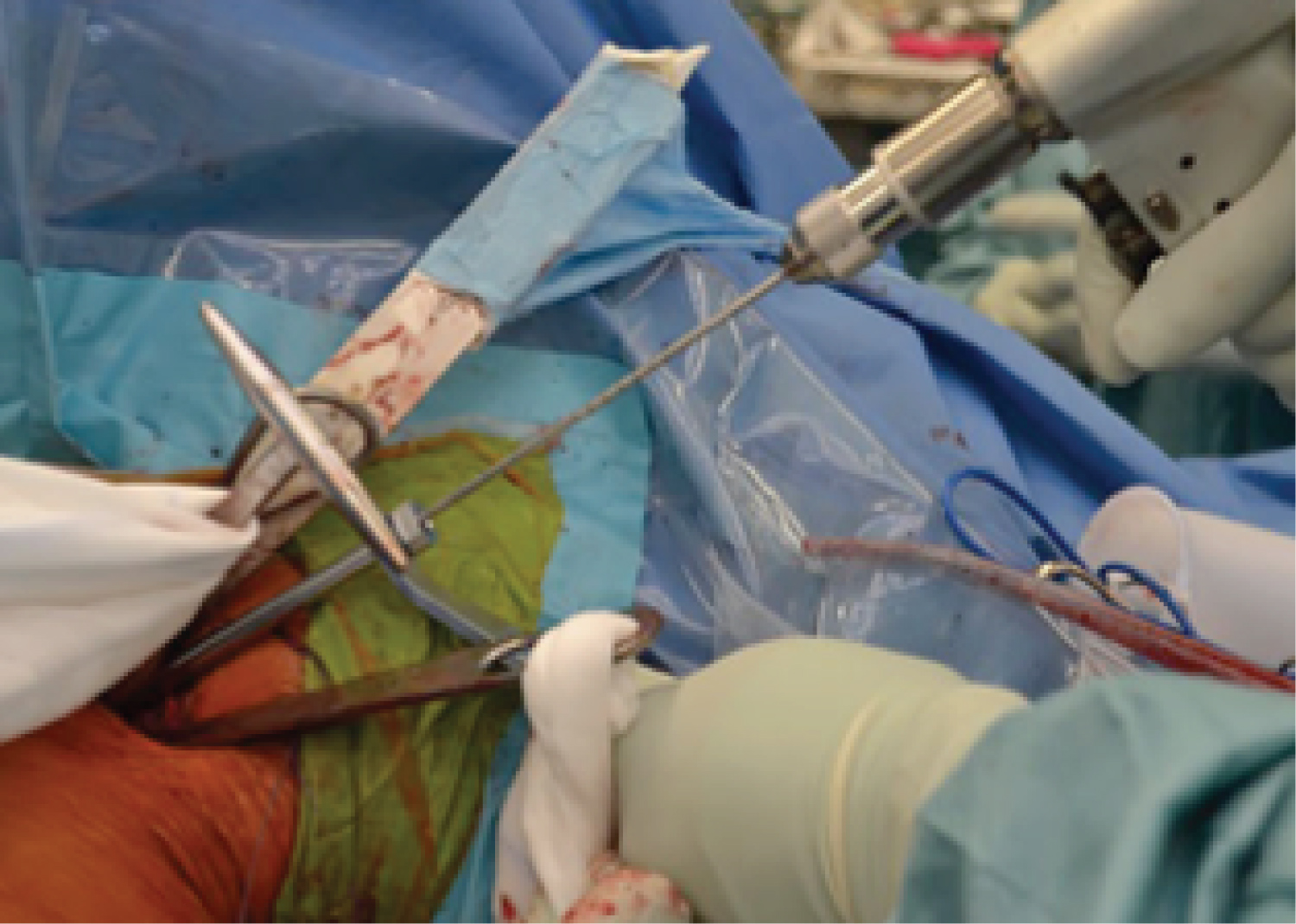
The standard 3.2 mm drill bit in an AO (Synthes, Paoli, PA, USA) Large Fragment set is 145 mm long with the corresponding 3.2 mm/4.5 mm double drill guide. This drill size allows subsequent placement of 4.5 mm partially threaded cannulated screws. The new technique utilised instrumentation off the Synthes VA-LCP Condylar Plate system. This included a 300 mm percutaneous 3.2 mm drill bit and a 4.3 mm drill sleeve/handle (Figure 1). There was no commercially available 3.2 mm drill sleeve equivalent to fit the larger handle however we did not have any issue with the 1.1 mm difference between the drill guide and drill bit. The advantage of the longer drill bit imparts a longer lever arm, which helps to achieve parallelism with the glenoid surface (Figure 2). The longer drill guide is an advantage in large or muscular patients to further improve control of the trajectory of the drill. The longer drill guide also helps to protect the skin and the skin adhesive material.
Patients
Patients without the use of the long drill bit and guide were named "Standard drill" group. The "Long drill" group corresponded to the ones that used the new system. They were chosen consecutively after the initiation of the technique to perform the open Latarjet procedure.
Patients had a mean age of 31-years-old for the first group and 23-years-old for the second group. Age, gender and side of operation were recorded for each patient. All the surgeries were performed by the senior author (Young). A total number of 66 patients were included.
Surgical technique
The full detailed surgical technique in its entirety was described in a publication by the senior author [10-12].
Radiographic assessment
All patients underwent standard post-operative radiographic assessment at 6 and 12 weeks. AP, glenoid, axillary and Bernageau views were obtained where possible. The Bernageau views were independently assessed by fellowship trained surgeons. By consensus, 3 patients in the standard drill group and 4 patients in the long drill group were excluded. These were all due to difficult patient position during radiographic exposure and subsequent inadequate exposure of a representative glenoid subchondral plate.
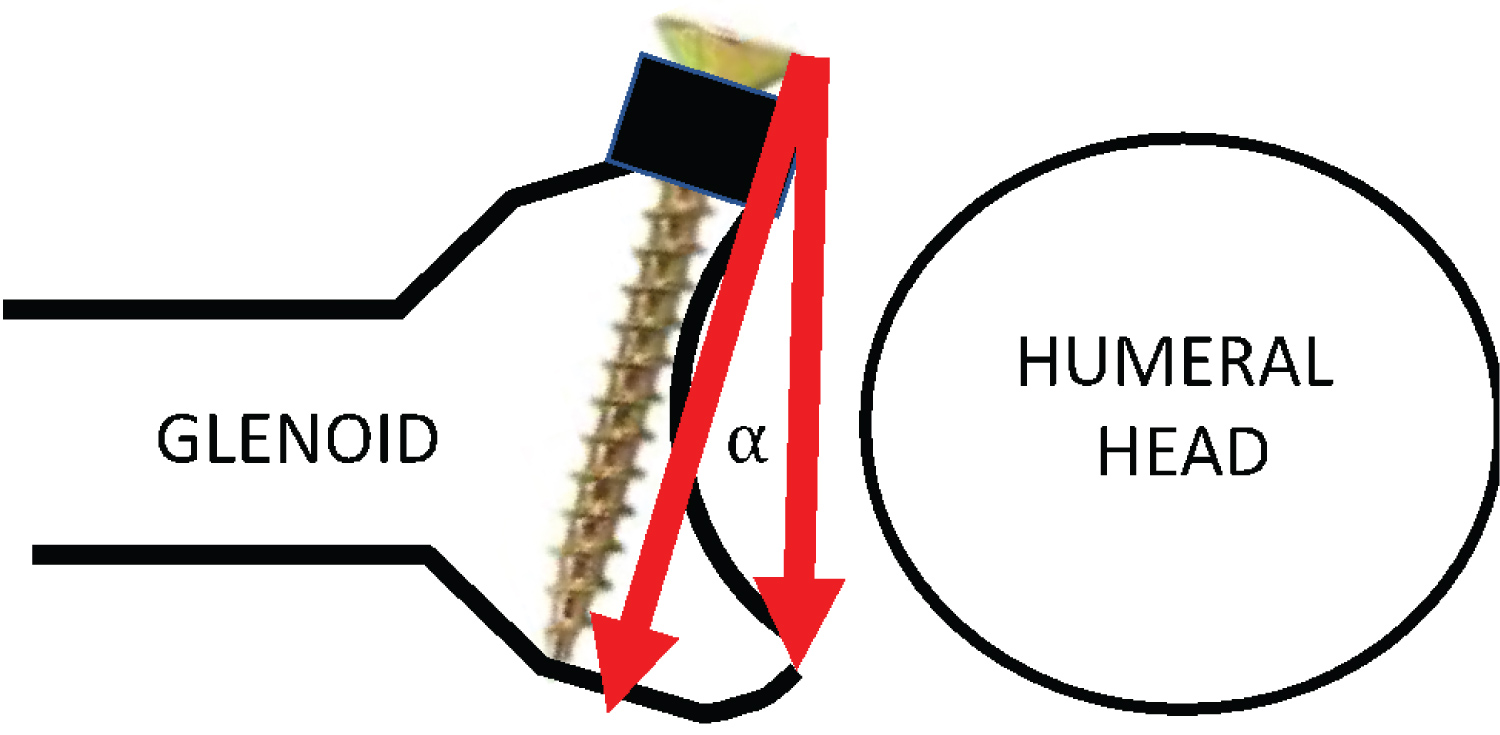
All radiographs were accessed by Intele Viewer (Intelerad Medical Systems Incorporated) and measurements performed by the Cobb Angle measurement tool provided in the software. Each radiograph was zoomed by x2 magnification with a field of view cantered on the glenoid and screws. The angle of the screws in relation to the bony glenoid was assessed in the axial plane, as described by Ladermann, et al. [10] (Figure 3). The line between the anterior and posterior glenoid margins of the subchondral plate represents the plane of the bony glenoid. The axis of the screw was represented by a line joining the centre of the screw head to the tip of the screw. The angulation value of the screws was then calculated from the two planes. A divergent screw from the glenoid surface is represented by a positive value and a convergent screw is represented by a negative value. The average of the two screw measurements was calculated and compared. The measurements were taken by two independent reviewers on two separate occasions, separated by 4 weeks (Observer 1 named O, and Observer 2 named R).
Statistical analysis
Data was analyzed both as an average angle of the two screws and as the maximum angle of the two screws. Descriptive statistics were performed by unpaired Students T test or chi squared test as appropriate. After positive testing for normality, the effect of gender, age and operated side were tested using linear regression. Intra- and Inter-observer reliability testing was performed using the intra-class correlation coefficient (ICC) and Bland-Altman (B-A) analysis. ICC values range from zero to one, with values closer to one indicating higher reproducibility.
Results
Patient demographics are presented in the Table 1 exhibiting that both groups presented similar characteristics, expect for age, which was significant (31.4 ± 1.9 versus 23.8 ± 0.9, p < 0.001).
The comparative analysis in terms of screw angles is shown in Table 2. There was a significant difference in average screw angle between the Standard drill and Long drill groups (5.8 ± 1.7 versus 2.1 ± 0.8, P = 0.037). This difference was not affected by gender or side of operation but was not present if corrected for age (which was significantly different between groups).There were no significant differences when maximum angles were compared.
There was excellent reliability (all correlations > 0.93) for both intra-observer and inter-observer measurements of screw angles, irrespective of whether the average angle or the maximum angle of the two screws was used (Table 3).
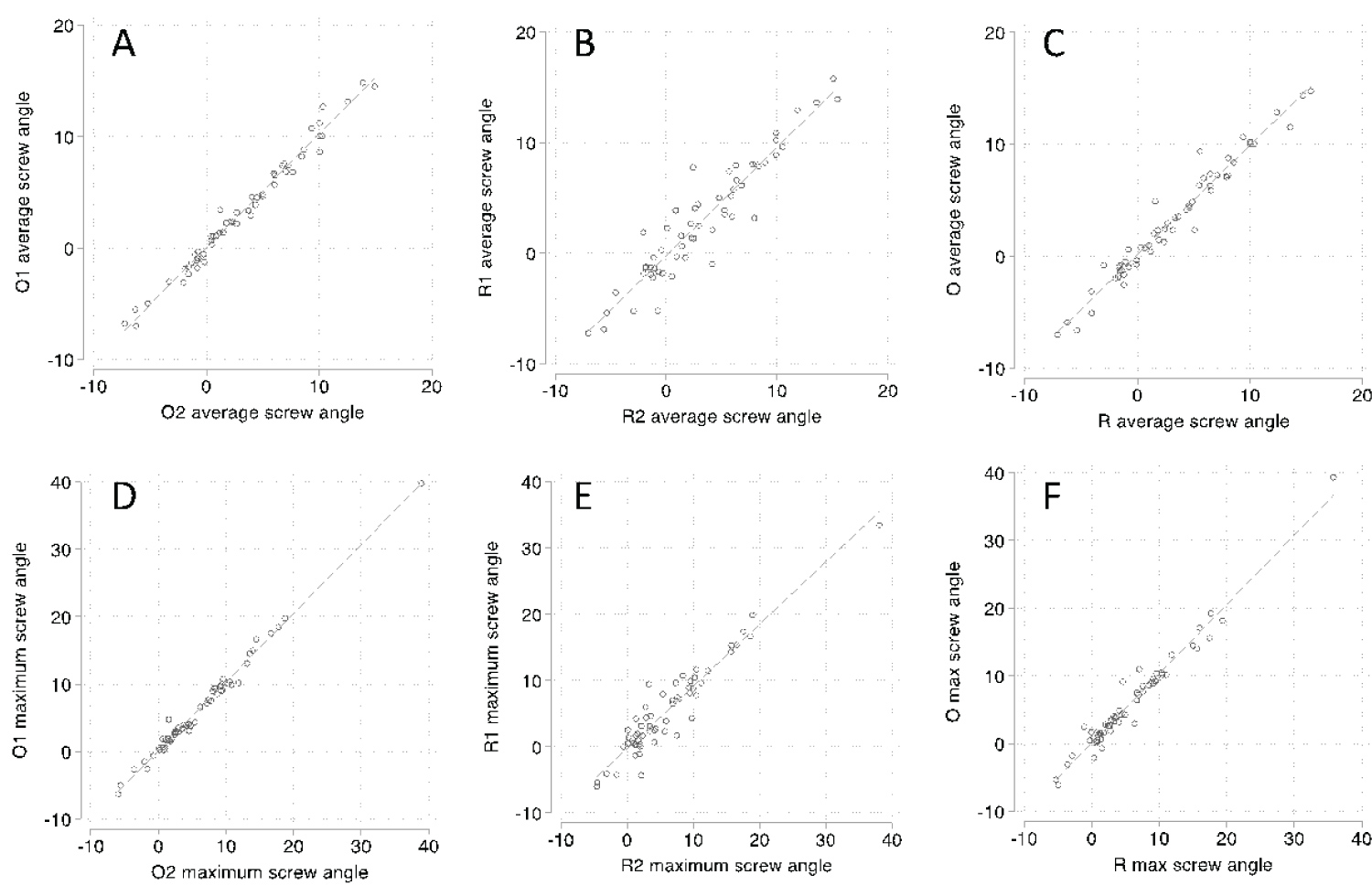
Scatter plots were performed for average (A-C) and maximum (D-F) screw angle showing intra-observer variation for observers O (A, D) and R (B, E) and inter-observer variation between observers O and R (C, F) (Figure 4).
Discussion
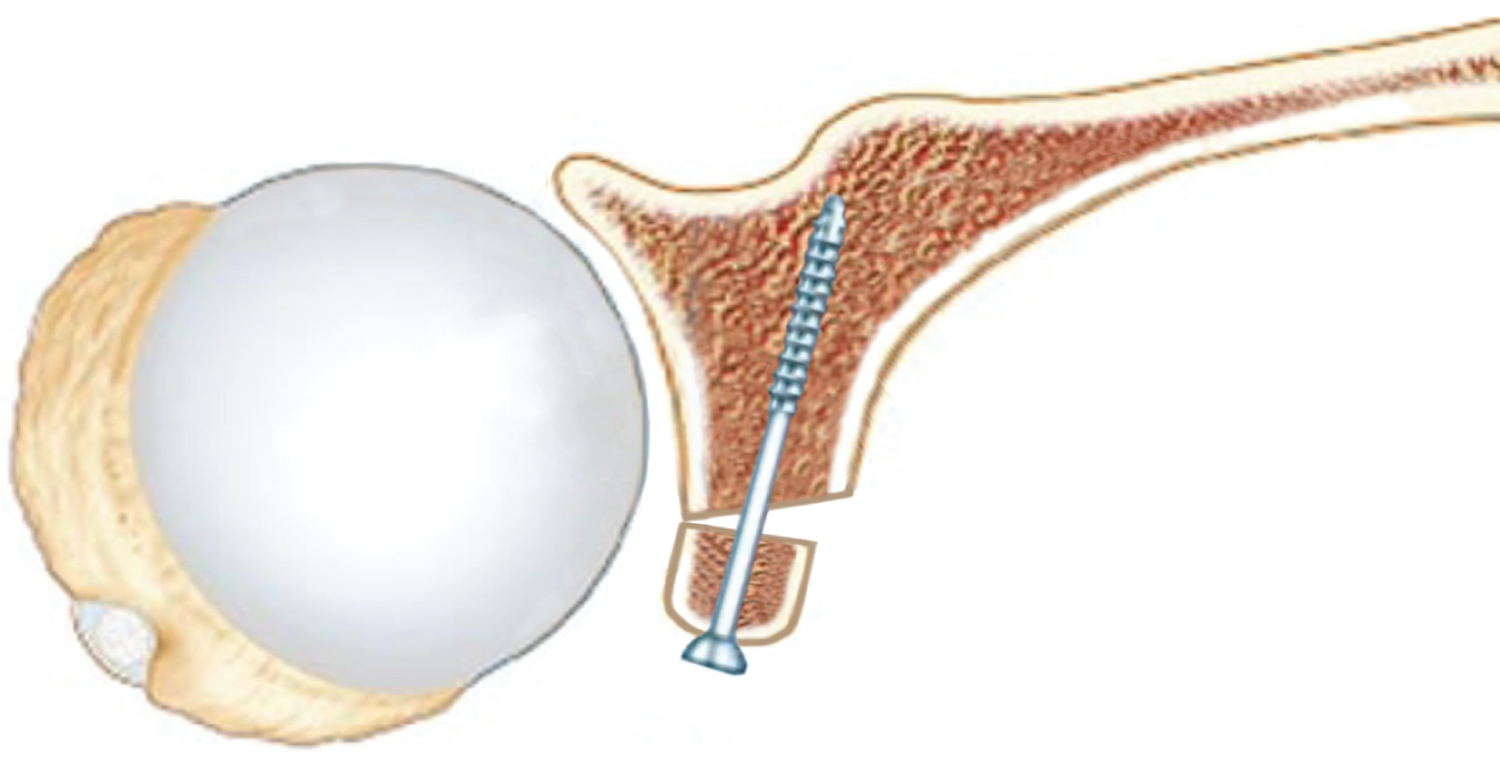
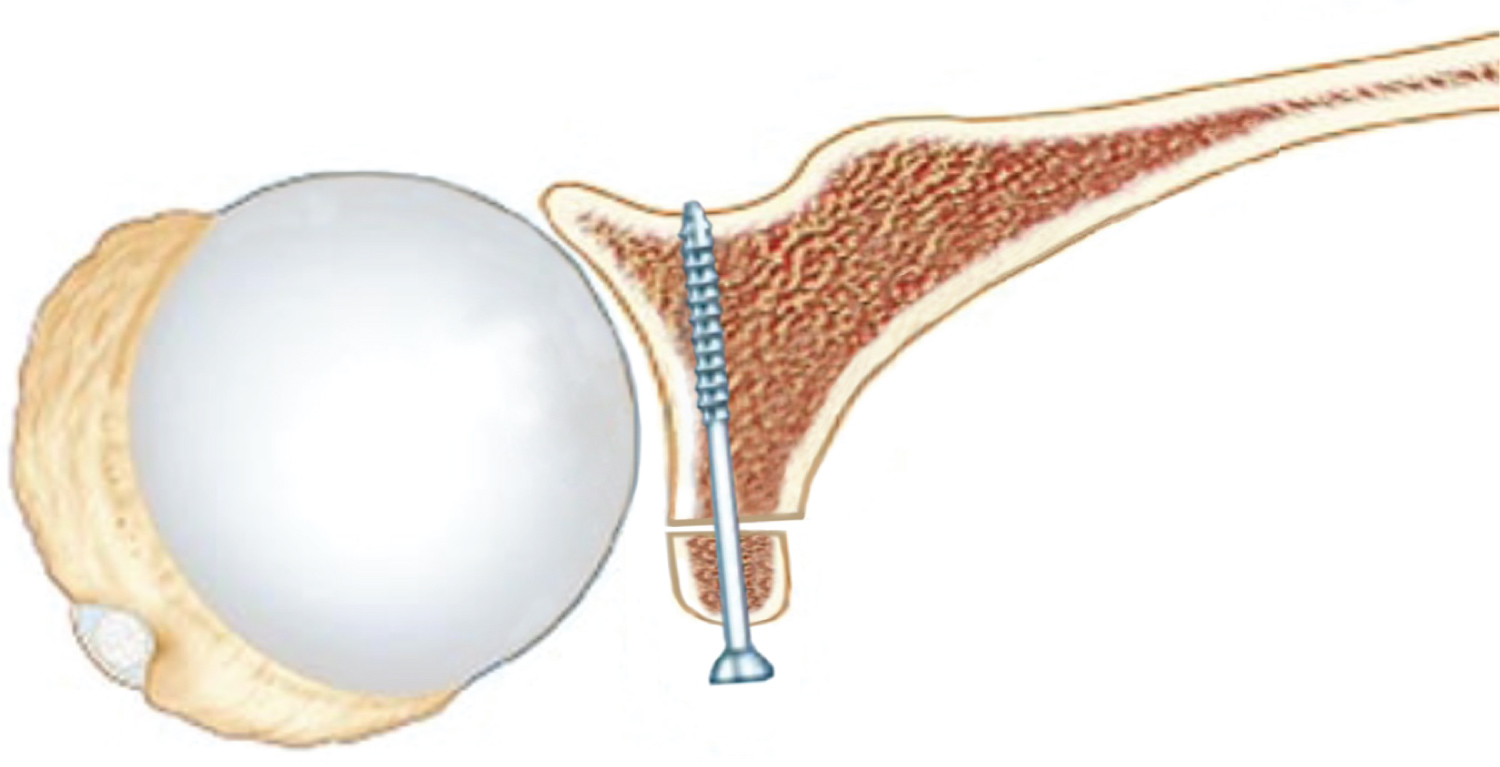
Use of the Latarjet procedure has become increasingly widespread with recognition of its ability to address cases with marked bone loss and reduce the rates of post-operative recurrent instability. It can be a very difficult operation to perform, both with open and arthroscopic techniques. Obtaining satisfactory positioning and angulation of the screws is perhaps the most important and at the same time challenging aspect of the procedure. Placing the screws parallel to the glenoid articular surface improves the chances of bone union of the graft to the glenoid and also reduces the likelihood of lateral positioning of the graft (Figure 5 and Figure 6). One of the known complications of the Latarjet procedure is arthritis of the shoulder due to lateral positioning of the graft [4-6,8,9] and so one of the main tenets of the procedure is to avoid lateral overhang of the graft. We have shown in this study that a simple change to a longer drill bit and soft tissue guide can improve the surgeon´s ability to achieve a screw trajectory more parallel to the glenoid articular surface. The long drill bit and guide are commercially available and used for lower limb trauma. It has been our experience that not only has the screw trajectory improved with our change in technique, but the operative step of drilling holes for the screws is technically much easier, particularly in larger patients. The long drill bit allows better leverage to obtain correct angulation and at the same time as the soft tissue guide helps push away medially the soft tissues of the anterior chest wall. Another advantage is that by achieving a lower screw angle the surgeon diminishes the risk of injuring the suprascapular nerve, which lies on the trajectory from the screw, as it is shown by Ladermann, et al. [10]. A positive screw angle elicits a divergent course from the joint line, so the more it tends to zero the lower the risk of the above consequences.
Limitations
Although some of the patients had a previous CT scan to plan the surgery, X-ray was used in all the patients as described above. CT scan measurements and details of the shoulder structures are more accurate, however, the X-ray measurement and standardization of the technique of visualization was performed. We also tested twice with different surgeons and the interrater reliability exhibited acceptable scores.
While we showed a significant statistical difference, we were not able to confirm clinical significance in this study. It is likely that there is an acceptable range in degree of angulation that is acceptable and resulting in satisfactory graft healing without lateral overhang. Of course, the starting position of the drill in distance from the glenoid margin is also important and we have studies that recommended an ideal position of 7 mm from the glenoid margin [11]. Nonetheless, if the goal of the surgeon is to achieve a screw trajectory more parallel to the glenoid articular surface, then this simple technique change could be useful.
We did not randomize, rather selected a series of cases just before and after the change in technique. The senior author is very experienced with the procedure and has always tried to place the trajectory of the screws as close to parallel to the glenoid articular surface as possible. There was no other change in the surgical technique between patient groups or alteration of the goal at surgery with regards to trying to achieve a screw trajectory parallel to the glenoid articular surface. Given that we were already trying very hard to achieve such a screw trajectory, it shows how effective the change to a long drill bit and guide has been. For less experienced surgeons, we believe that use of the long drill bit and guide may potentially improve their results more so.
Sources of Support that Require Acknowledgement
None.
Conflicts of Interest
None.
References
- Van der Linde JA, Wessel RN, Trantalis JN, et al. (2018) Review of Latarjet (1954) on the treatment of recurrent shoulder dislocations. JISAKOS 3: 242-248.
- Giles JW, Degen RM, Johnson JA, et al. (2014) The Bristow and Latarjet procedures: Why these techniques should not be considered synonymous. J Bone Joint Surg Am 96: 1340-1348.
- Zimmermann SM, Scheyerer MJ, Farshad M, et al. (2016) Long-term restoration of anterior shoulder stability: A retrospective analysis of arthroscopic Bankart repair versus open Latarjet procedure. J Bone Joint Surg Am 98: 1954-1961.
- Shah AA, Butler RB, Romanowski J, et al. (2011) Short-term complications of the Latarjet procedure. J Bone Joint Surg Am 94: 495-501.
- Domos P, Lunini E, Walch G (2018) Contraindications and complications of the Latarjet procedure. Shoulder Elbow 10: 15-24.
- Griesser MJ, Harris JD, McCoy BW, et al. (2013) Complications and re-operations after Bristow-Latarjet shoulder stabilization: A systematic review. J Shoulder Elbow Surg 22: 286-292.
- Young AA, Maia R, Berhouet J, et al. (2011) Open Latarjet procedure for management of bone loss in anterior instability of the glenohumeral joint. J Shoulder Elbow Surg 20: S61-S69.
- Barth J, Neyton L, Metais P, et al. (2017) Is the two-dimensional computed tomography scan analysis reliable for coracoid graft positioning in Latarjet procedures?. J Shoulder Elbow Surg 26: e237-e242.
- Kany J, Flamand O, Grimberg J (2016) Arthroscopic Latarjet procedure: Is optimal positioning of the bone block and screws possible? A prospective computed tomography scan analysis. J Shoulder Elbow Surg 25: 69-77.
- Lädermann A, Denard PJ, Burkhart SS (2012) Injury of the suprascapular nerve during Latarjet procedure: An anatomic study. Arthrosc J Arthrosc Relat Surg 28: 316-321.
- Young AA, Baba M, Neyton L, et al. (2013) Coracoid graft dimensions after harvesting for the open Latarjet procedure. J Shoulder Elb Surg 22: 485-488.
- Mattern O, Young A, Walch G (2017) Open Latarjet: Tried, tested and true. Ann Joint 2: 65.
Corresponding Author
Dr. Rebecca Lauren Emma Tang, MBBS, FRACS (Orth), Sydney Shoulder Research Institute, Suite 201, 156 Pacific Highway, St Leonards, Sydney, New South Wales 2065, Australia
Copyright
© 2022 TANG RLE, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.