An Overview of Sixteen Years Control Program against Rift Valley Fever in Saudi Arabia: A Review Study
Abstract
Rift Valley Fever (RVF) is a serious life-threatening disease with severe clinical manifestations and health consequences for humans and a wide range of domestic animals. In September 2000, a RVF outbreak was reported in Jazan region south-west Saudi Arabia with 886 human cases including 124 deaths. This review provides: 1) An overview of RVF control program in Saudi Arabia and current control measures; 2) A feasibility assessment of some intervention measures that have been launched since the early recognition of RVF. Currently, with the exception of Saudi Arabia, devastating outbreaks of RVF continue to occur frequently in the 21st century and the number of countries reporting cases have increased rapidly. Around 19 large outbreaks including substantial numbers of human and animal deaths have been reported for the period between 2000-2018. In contrast to the aforementioned situation in endemic areas, control program against RVF in Saudi Arabia has completely reversed the risk of outbreaks over the past 16 years and provide long term protection against RVFV exposure. The successful control program had the following parts: Vector control campaigns using ULV; fog and sprinkle sprayers; draining and filling of water swamps with soil; biological control; mosquito surveillance; sustaining vaccination campaigns; regular examination of sentinel herds; serological examination of clandestine imports at Al-Twal quarantine station (at the border with Yemen); and targeted sero-surveillance during rainy seasons.
The effectiveness of the current control program can be demonstrated not only by the decreased in prevalence of RVF from 12.3% in 2000 to 0.015% in 2015, but also by the absence of human and animal active cases since the 2000 outbreak. Additionally, vector control measures that targeted outdoor habitats in Jazan region, contribute to significant reduction in malaria case incidence from 2000 to 2014. The Saudi's current control initiative could be used as a guideline for control or as a suitable model to replicate in other endemic countries.
Keywords
RVF-control-prevention
Introduction
RVF is a serious infectious disease in humans and a wide range of domestic ruminants, caused by mosquito-borne virus that belongs to the family Bunyaviridae, genus phlebovirus. Human can be infected either by mosquito bites or through the exposure to blood, aborted fetal materials, body fluids, or tissues of infected animals [1]. It was first reported among livestock in Kenya in 1931, since then it has been reported not only in most African countries, but also in Arabian Peninsula, particularly in Saudi Arabia and Yemen in the year 2000 [2,3]. This outbreak was the first appearance of the RVFV in new geographical areas outside Africa [4] Jazan region-South west Saudi Arabia-has had the hardest hit by the disease. Out of the total animal cases, (65.6%) were occurred in Jazan region, (26.9%) in Asir and (7.5%) in Alquenfeda [5]. High mortality rates from RVF in hospitalized patients were reported during the outbreak including 124 deaths. Small percentage of people developed much more severe signs involving, hemorrhagic manifestations, retinitis, meningoencephalitis and death (19.4%, 9.7%, 4.2% and 33.9%) respectively. The main factors leading to deaths in humans could be attributed to hepatocellular failure (75.2%), followed by acute renal failure (41.2%) [6]. This outbreak raised concerns about the potential incidence and establishment of the disease in different environmental conditions and could affect areas haven't ever experienced the disease before as a consequence of climate change and globalization of trade in animals and its products [7]. Surprisingly, it has been proved in a retrospective study that Saudi Arabia was free from RVF until 1995 and most probably before the 2000 epidemic [8]. The virus apparently introduced to Saudi Arabia during the religious festivals (Eid Aladha) through importation of live animals from African Horn countries, since, the virus isolated from the first patients during 2000 outbreak had an RNA sequence similar to the virus isolated in 1997-1998 East African outbreaks [9,10]. The adverse effects of the disease and the serious socio-economic impacts obliged the relevant veterinary authorities in Saudi Arabia to devote an effective control program based on breaking the transmission cycle and raising herd immunity. This paper specifically aims to: 1) Summarize control measures against RVF that operated in Saudi Arabia since 2000; 2) Assess the effectiveness and benefits of the current RVF control program.
Methods of Data Collection
A systematic review was conducted by searching Google Scholar (https://scholar.google.com/) up to November 15, 2018. The search terms "RVF" and "Saudi Arabia" were combined using the operator "AND" to identify the original research articles. A total of 1610 articles were identified by searching Google Scholar. The identified studies were screened on the basis of its relevance to the aim of study and published in English-language. Of 1610 screened reports, 17 articles were finally selected. Additional data were obtained from Veterinary records in Ministry of Environment, Water and Agriculture K.S.A as well as from World Health Organization (WHO), Centers for Disease Control and Prevention (CDC).
Component of the RVF control program
Various control measures have been implemented in Jazan over the past sixteen-years including the following: 1) Restriction of animal movement, which was implemented in the affected areas in Jazan, Tohamet Aseer, Tohamet Mekkahand Tohamet Al-bahah. Unvaccinated animals are not allowed to leave the outbreak zones; 2) Vector control campaigns using ULV, fog and sprinkle sprayers in rural farms, cities and villages were routinely adopted; 3) Draining and filling of water swamps with soil as well as biological control; 4) Mosquito surveillance and virus detection in mosquitoes by molecular techniques. Finally, sustaining vaccination campaigns, regular examination of sentinel herds, serological examination of clandestine imports at Al-Twal quarantine station (at the border with Yemen), and targeted sero-surveillance during rainy seasons.
Vaccination against RVF: The live attenuated vaccine (Smithburn strain) has been used as the gold standard vaccine in Jazan region since the outbreak of 2000. Although, the annual vaccination program of RVF in high risk areas is restricted to nonpregnant animals above six months of age before or at the mating season to ensure maternal antibodies and to avoid abortion, it has been proved through serological surveys that vaccination is effective and highly beneficial in controlling infections
Sentinel herds: Sentinel animals are unvaccinated animals, related to the local breeds and imported from regions free from RFV infection. These animals were subjected to IgM and IgG antibodies tests against RVF before they were placed on ideal habitats for RVF vectors so as to investigate the potential circulation of RVFV during inter-epizootic period (Table 1) [12].
Land spraying: Outdoor land spraying with residual insecticides that is targeting adult mosquitoes is used to control mosquito populations in vegetation or resting sites such as animal shelters at times relevant to mosquito activity, mainly 1-2 hours after sunset or 1-2 hours before sunrise. Both of ULV spraying and thermal fogging equipment are usually mounted on ground vehicles Figure 1.
Arial spraying: Arial spraying targeting adult and immature stages has effectively reduced the insect populations over a large scale, notably, in areas not accessed by roads or ground vehicles such as dense vegetation, forested lands, valleys, streams, lakes and sewage stations. Both of helicopter and fixed wing aircrafts contribute importantly to vector control Figure 2.
Biological control: The numerous disadvantages of insecticides such as increasing resistance to commonly used pesticides and the global growing concerns over the use of insecticides in the environments, have promoted the use of biological control and environmental management rather than chemical control. Biological control aimed to kill larvae without polluting or damaging the environment by using living organism like bacteria Bacillus thuringiensis var. israelensis (B.T.I) (Table 2).
Environmental management: Environmental management is an effective approach in vector control to maintain permanent control of mosquito via altering or removing vector breeding sites, which can be obtained by covering water containers, removal of small used cans or tires, flushing streams, draining water to follow the natural flow, filling in ditches with soil or stones, subsoil drainage
Entomological surveillance: Mosquito surveillance commonly conducted before insecticides treatments to test the density of mosquitoes in breeding habitats and post treatments to evaluate the efficiency of spraying. A light CO2 baited traps placed overnight at different locations where mosquito breeding sites are found (Table 3). These traps are usually collected the following morning before sending to the laboratory Figure 4.
Evaluation of RVF control program
A zero incidence of RVF infection in human: Currently, with the exception of Saudi Arabia, outbreaks of RVF continue to occur frequently in the 21st century and many countries were harder hit by the disease. Around 19 large outbreaks with a substantial numbers of animals and humans deaths have been reported for the period between 2000-2018, in particular, Mauritania which has been affected in (2010, 2012, 2013 and 2015) (Table 4). By contrast, no human fatalities have ever been reported in Saudi Arabia since the 2000 outbreak. It is obviously that the control program plays a significant role in RVF prevention over the past sixteen-years, despite the recent climate change in Arabian peninsula and early warning alerts that issued form the National Aeronautics and Space Administration (NASA) and indicated elevated risk of RVF activity in Saudi Arabia due to above normal rainfall in 2005 and 2015 [14,15].
Low incidence of RVF in local herds and sentinel animals: The efficacy of the current control program can be demonstrated not only by the absence of human cases, but also by the high decrease in prevalence of RVF in local herds from (12.3%) in 2000 to (0.015%) in 2015 [5,16], Currently, the circulation of RVFV mainly be restricted to sporadic cases without clinical signs mostly in sentinel herds. The absence of clinically active cases in humans as well as in animals since the first outbreak reflects the high efficiency performance in control program [17].
Evaluation of vaccination (a pooled analysis of cross-sectional surveys): A pooled Analysis of positive cases of RVF that were diagnosed through cross-sectional surveys in high risk areas and sentinel herds screening program (information taken from veterinary records) has been done to evaluate whether or not vaccination has a significant effect in preventing outbreaks as long as both of sentinel herds and local animals are exposed to the same level of RVFV infection (Table 5).
The risk of RVF infection in sentinel herds is 36/330 = 10.9 cases per 100 animals. While the risk in vaccinated animals is 53/18287 = 0.29 cases per 100 animals. The odd ratio is (0.02) P-values < 0.05, which tells us that vaccination seems to be protective against RVF.
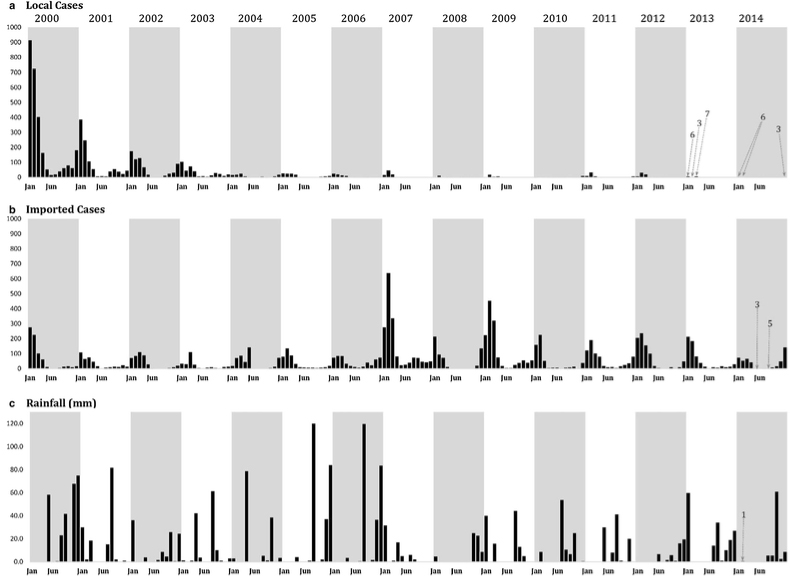
A significant decrease in malaria incidence: From 2000 to 2014, efforts to control malaria in the Kingdom of Saudi Arabia has successfully reduced malaria cases, particularly in locally acquired cases wherein a significant decline was observed from (2756 cases; 35.3 per 10,000 population) in 2000 to (15 cases; 0.11 per 10,000 population) in 2014 Figure 5. This reduction attributed to coincidental expansion of control efforts including RVF vector control program that targeted outdoor habitats [18].
Conclusion
To sum up, the study has provided some results which can be reviewed as follows: 1) RVF can be controlled through routine vaccination in combination with vector control in high risk zones as well as effective surveillance system based on sentinel surveillance, targeted surveillance during rainy season and mosquito surveillance; 2) The study has recognized the control program in Saudi Arabia has as highly effective in preventing outbreaks as long as; a) No clinically active cases in humans and animals since the first outbreak; b) The prevalence of RVF is remarkably decreased from (12.3%) in 2000 to (0.015%) in 2015; 3) The integrated vector control strategies that have been implemented in the region could help to reduce incidenence of emergent mosquito borne diseases such as malaria; 4) The current control program could be used as a successful model to replicate in other endemic countries.
Competing Interests
The author declares that there is no conflict of interest regarding the publication of this paper.
References
- Rift Valley fever (2016) World Health Organization. Media centre.
- Daubney R, Hudson JR, Garnham PC (1931) Enzootic hepatitis or Rift Valley fever. An undescribed virus disease of sheep, cattle and man from East Africa. J Pathol Bacteriol 34: 545-579.
- Madani TA, Al-Mazrou YY, Al-Jeffri MH, et al. (2003) Rift Valley fever epidemic in Saudi Arabia: Epidemiological, clinical, and laboratory characteristics. Clin Infect Dis 37: 1084-1092.
- Balkhy HH, Memish ZA (2003) Rift Valley fever: An uninvited zoonosis in the Arabian Peninsula. Int J Antimicrob Agents 21: 153-157.
- Elfadil AA, Musa SM, Alkhamees M, et al. (2004) Epidemiologic study on Rift Valley fever in the south-west Kingdom of Saudi Arabia. J Sci Tech 5: 110-119.
- Al-Hazmi M, Ayoola EA, Abdurahman M, et al. (2003) Epidemic Rift Valley fever in Saudi Arabia: A clinical study of severe illness in humans. Clin Infect Dis 36: 245-252.
- Kim HJ, Lyoo HR, Park JY, et al. (2016) Surveillance of Rift Valley fever virus in mosquito vectors of the Republic of Korea. Vector Borne Zoonotic Dis 16: 131-135.
- Al-Afaleq AI, Abu EE, Mousa SM, et al. (2003) A retrospective study of Rift Valley fever in Saudi Arabia. Rev Sci Tech 22: 867-871.
- Davies FG (2006) Risk of a Rift Valley fever epidemic at the haj in Mecca, Saudi Arabia. Rev Sci Tech 25: 137-147.
- Bird BH, Khristova ML, Rollin PE, et al. (2007) Complete genome analysis of 33 ecologically and biologically diverse Rift Valley fever virus strains reveals widespread virus movement and low genetic diversity due to recent common ancestry. J Virol 81: 2805-2816.
- Alhaj M (2016) Safety and efficacy profile of commercial veterinary vaccines against Rift Valley fever: A review study. J Immunol Res.
- Elfadil AA, Hasab-Allah KA, Dafa-Allah OM (2006) Factors associated with rift valley fever in south-west Saudi Arabia. Rev Sci Tech 25: 1137-1145.
- Rozendaal JA (1997) Vector control: Methods for use by individuals and communities. World Health Organization.
- Anyamba A, Chretien JP, Formenty PB, et al. (2006) Rift Valley fever potential, Arabian peninsula. Emerg Infect Dis 12: 518-520.
- Almazroui M, Nazrul Islam M, Athar H, et al. (2012) Recent climate change in the Arabian Peninsula: Annual rainfall and temperature analysis of Saudi Arabia for 1978-2009. Int J Climatology 32: 953-966.
- Alhaj MS, Elmanea AA, Shazali LA, et al. (2015) Surveillance study on Rift Valley fever in Jazan region, Saudi Arabia. IJASTR 5.
- AlAzraqi TA, El Mekki AA, Mahfouz AA (2013) Rift Valley fever among children and adolescents in southwestern Saudi Arabia. J Infect Public Health 6: 230-235.
- El Hassan IM, Sahly A, Alzahrani MH, et al. (2015) Progress toward malaria elimination in Jazan province, Kingdom of Saudi Arabia: 2000-2014. Malar J 14: 444.
- OIE (2012) World Organization for Animal Health.
- WHO (2018) World Health Organization.
- CDC (2017) Centers for Disease Control and Prevention.
Corresponding Author
Mutaz S Alhaj, Campaign for Control of Rift Valley fever, Gizan City, Saudi Arabia.
Copyright
© 2019 Alhaj MS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.