Fear and its Influence on the Healthcare Seeking Behaviour of Jamaicans during the Coronavirus Disease 2019 (COVID-19) Pandemic
Abstract
Introduction: In March 2020, Jamaica recorded its first case of COVID-19. Since then, fear has become a dominant factor and a possible hindrance to health-seeking behaviour.
Objective: The purpose of this study was to 1) Examine the level of fear among Jamaicans since the COVID-19 pandemic began, 2) Investigate how the fear of COVID-19 impacted Jamaicans in seeking health care, 3) Determine the health status of Jamaicans since COVID-19 and 4) Find out whether the respondents experienced problem seeking health care before COVID-19.
Methods: The research design consisted of a non-probability sampling survey created in Google Forms to collect data from 711 sampled respondents across Jamaica. The data was converted from Google Forms into Statistical Packages for the Social Sciences (SPSS) for Windows, Version 26.0. Frequencies, percentages, and bivariate analysis (chi-square) facilitated data analysis. The researchers used a p-value of 5.0% to determine statistical significance.
Findings: Before COVID-19, 89.2% (n = 634) of the respondents indicated they did not have a problem seeking health care compared to 53.4% (n = 249) who reported being afraid to visit healthcare facilities since COVID-19. Furthermore, 66% (n = 469) of the respondents indicated that they were fearful of contracting the Coronavirus. 75.4% (n = 536) mentioned that they knew someone who had contracted COVID-19, and 18% (n = 128) reported that this caused them to feel very fearful. 94.8% of respondents changed their daily habits to adhere to COVID-19 protocols.
Conclusion: With the emergence of COVID-19, fear has become a prominent variable and a possible barrier that affects healthcare seeking behaviour. Jamaica's Ministry of Health and Wellness should promote health and wellness during these challenging times to prevent later strains on the healthcare system from non-communicable diseases.
Keywords
Fear, Healthcare-seeking behaviours, COVID-19, Jamaica, Health belief model
Introduction
Historically, the human population has experienced deaths and physical harm caused by infectious diseases. Some of these infectious diseases included the Black Death (1346-to-1353), Spanish flu (during 1918), and Swine flu (or H1N1 virus occurred in 2009), all of which reached pandemic levels (Centers for Disease Control and Prevention [1-4]. According to Jarus 'the Black death,' caused by a strain of the bacterium Yersinia pestis spread throughout Asia and Europe, by fleas on infected rodents, killing over half of Europe's population. Approximately 100,000 people, including 15% of the population of London, died. An estimated 500 million people from the South Seas to the North Pole contracted the Spanish flu between 1918-1920. The 2009 swine flu pandemic resulted from a new strain of H1N1 in Mexico that spread globally. An estimated 1.4 billion infections occurred worldwide, with 80% of the deaths among people younger than 65-years-old [5].
In the year 2019, the first case of the Coronavirus disease 19 (COVID-19) started in Wuhan City of China in early December 2019 [6-9]. Within weeks the contagious disease had spread across the world, leading to a pandemic [9,10] As of December 29, 2021, statistics from the World Health Organization [11] indicated that COVID-19 has claimed 5,411,759 lives globally and has resulted in 281,808,270 infections, with the numbers increasing daily worldwide.
Statistics from Jamaica's Ministry of Health and Wellness (Ministry of Health and Wellness, 2021) revealed that as of December 29, 2021 [12]. Jamaica had recorded approximately 93,591 (i.e., females, 53,231; males, 40,357; unknown, 3) confirmed COVID-19 cases with 2,470 deaths. The context for the anxiety and fear of people as a result of COVID-19 is amply fitting in a comment by the World Health Organization that “…this outbreak around the clock and we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction” and account for the continuous statistical updates on the virus [13]. Hence, the COVID-19 pandemic is a source of fear, worldwide [14,15]. Fear is defined as “an emotional response to a threat perceived by an individual, and considered a functional, adaptive and transient response to stimuli, briefly resulting in physiological changes.” People fear the unknown, such as infectious diseases- viruses which are imminent and easily transmitted [16].
The impact of fear can result in negative and positive consequences. Adverse outcomes include avoiding healthcare services and settings due to the fear of becoming ill. Positive effects include greater adherence to infection control strategies such as frequent hand washing [17]. When individuals perceive a need for healthcare services, they undertake health-seeking behaviours [18]. Currently, in the Jamaican health system, patients do not seek healthcare services primarily because of fear. The fear currently experienced is directly attributed to the likelihood of exposure to COVID-19 in healthcare facilities. This justified fear exists because patients with underlying conditions may contract the disease during hospitalization [19].
Patients have valid reasons for concern about contracting the COVID-19 disease while seeking care in COVID-19- designated receiving hospitals. As such, they understandably avoid or delay seeking care. However, this decision can be detrimental and can place many patients at risk for bad outcomes. Patients with emergent medical conditions who would usually visit the hospital or other health care facilities now choose to stay home, increasing their risk of complications or death [19-21] . In fact, Chileshe, et al. [22] articulated that some people have been brought in dead as a result of not seeking healthcare treatment during the COVID-19 pandemic. Chileshe, Mulenga, Mfune, Nyirenda, et al.'s brings into focus the hesitancy of people in seeking healthcare even during periods of pandemic, particularly those with non-communicable diseases including respiratory diseases.
Healthcare seeking behaviour (HSB) is “any action or inaction undertaken by individuals who perceive themselves to have a health problem or to be ill to find an appropriate remedy.” Healthcare seeking behaviour falls within the broader concept of health behaviour, which encompasses activities undertaken to maintain good health, prevent illness, and deal with any departure from a good state of health [23]. Despite the general belief that people ought to seek healthcare in periods of epidemic or pandemic, Czeisler, et al. [24] found that this was not the case in 2020. An important issue in the COVID-19 pandemic is whether people are seeking healthcare as indicated by policymakers, particularly in Jamaica. Currently, there is a paucity of research in the area of healthcare seeking behaviour of Jamaicans during the COVID-19 pandemic and this highlights a need for urgent empirical inquiry on the matter that will assist policymakers in understanding pending healthcare challenges.
The purpose of this research is to discover the extent of fear among Jamaicans during the COVID-19 pandemic and its influence on healthcare seeking behaviour. The researchers formulated three research questions to guide this research. They include: 1) Has the level of fear among Jamaicans increased since the COVID-19 pandemic? 2) Has a fear of COVID-19 impacted Jamaicans in seeking healthcare? and (3) What is the health status of Jamaicans since COVID-19? The researchers will explore whether Jamaicans sought healthcare before and during the COVID-19 pandemic and investigate health maintenance of Jamaicans during the pandemic.
Theoretical framework
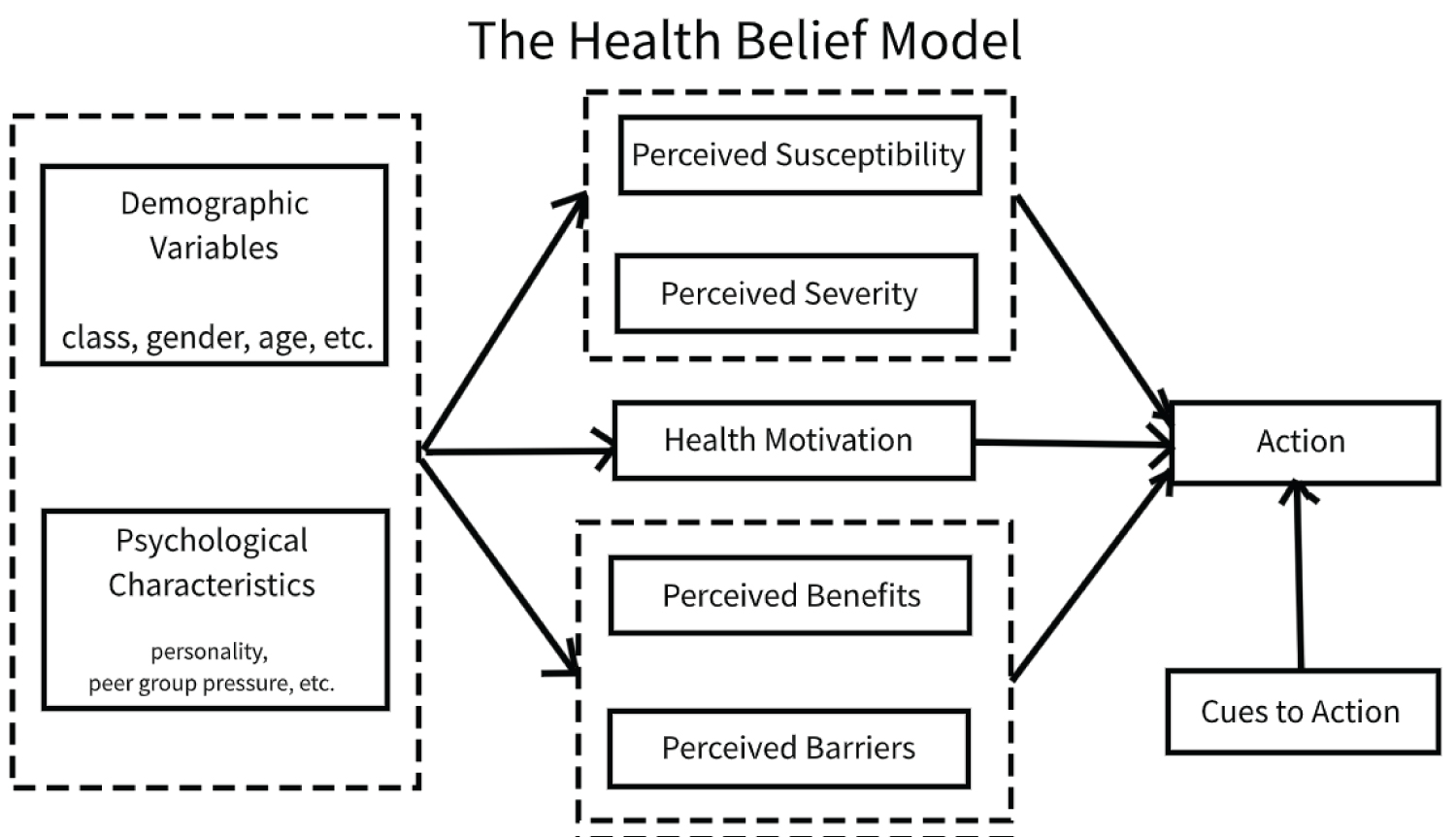
The Health Belief Model (HBM) was developed in 1950 by social psychologists in the U.S. Public Health Service and is the most used behaviour research model [25]. This model presents concepts about people's perceptions and motivations and the benefit-driven healthcare seeking decision steps. When it comes to an individual's healthcare seeking behaviour, it focuses on contextual elements of an individual and the prevailing health system characteristic. The focus of healthcare services utilization research from a behavioural perspective identifies the most relevant individual and environmental factors. Beliefs about the impact of illness and consequences depend on the person's perception of four critical areas: the severity of potential disease, the person's susceptibility to that illness, the benefits of taking preventive action, and the barriers to taking that action. Beliefs and health motivation are also conditioned by sociodemographic variables (class, age, gender, religion etc.) and by the psychological characteristics of a person [26].
A decision-making process precedes health-seeking behaviours and is usually governed by individuals, household behaviour, community norms and expectations, provider-related characteristics, and behaviour [18]. As the coronavirus pandemic ravages the world, it induces fear, worry and concern among the world's population. Inappropriate health seeking behaviour results in poor health outcomes, increased morbidity and mortality, and poorer health statistics [23].
The HBM proposes that two significant factors influence whether a person performs a particular health behaviour. These factors are the degree to which the person perceives the disease (negative outcome) as threatening and the degree to which the health behaviour effectively reduces the risk of an adverse health outcome [18]. One idea from this model is that the perceived threat (fear) of a disease can challenge the healthcare seeking behaviour and motivational intention of individuals. This idea may underpin the explanation for fear of the COVID-19 disease and its influence on Jamaicans' healthcare seeking behaviours for this current study.
Expanding on the notions of fear, one study reported a higher level of fear of COVID-19 in females. Researchers found that females were 3.45 times more likely to display high levels of fear than low levels compared to males. Moderate fear of COVID-19 could increase risk perception against the disease and promote preventive behaviours [27].
The HBM applies to the research question: “Has the fear of COVID-19 impacted you in seeking health care?" The degree of fear that an individual has, can determine a particular health behaviour. Several factors, such as the extent to which the person perceives COVID-19 as threatening, risk of contracting COVID-19, its impact on their health condition, and practising preventive care measures may influence healthcare seeking behaviours. Therefore, this model supports investigating how the fear of COVID-19 influences an individual's health care seeking behaviour (Figure 1) [28].
Literature Review
This study focuses on the extent of fear among Jamaicans during the COVID-19 pandemic and its influence on their healthcare seeking behaviours. From a comprehensive review of the literature, no existing research on the specific topic emerged for the targeted population; however, some studies support the argument that the outbreak of COVID-19 caused fear globally, impacting health seeking behaviours [29,30].
Therefore, this research explores the influence of fear on healthcare seeking behaviours within a specific population.
Fear is an adaptive emotion that serves to mobilize energy to deal with potential threats. However, when fear is not well calibrated to the actual threat, it can be maladaptive. For instance, when fear is too excessive, this may have detrimental effects at the individual level (e.g., mental health problems such as phobia and social anxiety) and the societal level (e.g., panic shopping or xenophobia) [29]. On the other hand, when there is insufficient fear, this may also harm individuals and society (e.g., people ignoring government measures to slow the spread of COVID-19 or reckless policies ignoring the risks). Furthermore, fear triggers safety behaviours (e.g., hand washing) that can mitigate specific threats (e.g., contamination). Still, they may paradoxically also enhance fear (e.g., contamination concerns and health anxiety) [29].
In two studies of university students, findings indicated that more health anxiety was associated with increased fear for the H1N1 "Swine flu" pandemic [30] and the outbreak of the Zika virus in 2015-2016 [31]. Hence, we expect that health anxiety is predictive of increased fear of the coronavirus [29].
Because of the COVID-19 pandemic, there is a reluctance within the population to seek urgent medical care. A study underway in the United States indicates a 38% fall in heart attack patients calling 911 or going to the emergency rooms. Stroke centres in the United States and Europe showed a decrease in stroke patients presenting to emergency rooms. Furthermore, doctors in Europe and China reported emergency cardiac patient admissions decreased significantly [20].
According to Saah, et al. [32] individuals with cold or flu symptoms avoided visiting healthcare facilities, fearing a COVID-19 diagnosis. This fear compounded by the heightened awareness of COVID-19 infected persons interacting with healthcare professionals in health facilities [32].
Method
This research employed quantitative research design in order to answer the research question, "Has the level of fear among Jamaicans increased since the COVID-19 pandemic?" Mishra & Alok [33] contended that quantitative research involves systematic experimental analysis of observable phenomena via statistical, mathematical, or computational techniques in numerical form such as statistics and percentages [33].
The structure of the quantitative study entails a web-based cross-sectional descriptive research design by way of a convenience sampling method. A team of data collectors were trained for a period of six weeks in data collection, research design, and ethics. During the training each prospective data collector had to successfully pass an Online course in Ethics. Following the completion of the Online Ethics course, the data collectors were allowed to solicit respondents from Jamaicans across the nation. Each of the collectors were given a particular set of parishes, and they were to collect data only from people with those specified geographic areas. The data collection occurred between April to July 1, 2021 and consisted of 711 male and female participants from ages 18 years and older from all 14 parishes in Jamaica.
A standardized instrument was design with the aid of Rea and Parker's [34] work and the works of other methodologists [35-37]. The instrument comprised of 16 close-ended items of which 3 were demographic characteristics (i.e., age, gender, and parish of residence). The item on healthcare seeking behaviour was adopted from the Jamaica Survey of Living Conditions (Planning Institute of Jamaica (PIOJ) & Statistical Institute of Jamaica (STATIN) [38] and other items were drafted by the research team in keeping with the research questions. On completion of the instrument design, it was forwarded to a methodologist and statistician who provided guidance on the content validity of the items. The researchers used Google Forms to create the online survey questionnaire. Study participants received a WhatsApp message containing information on the nature and purpose of the study and a survey link. The completed survey consisted of 11 closed-ended questions and took approximately 2 minutes to complete. Guaranteeing confidentiality and anonymity ensured that the participants would be honest with their responses. Researchers displayed information retrieved from respondents on graphs and tables using Microsoft Excel, IBM Statistical Packages for the Social Sciences (SPSS), and Microsoft Word. Frequencies, percentages, and bivariate analysis (chi-square) facilitated data analysis. The researchers used a p-value of 5.0% to determine statistical significance.
Findings
Table 1 showed that majority of the respondents were females and within the 18-24 years age group with majority of the respondents resided in Kingston & St. Andrew (25.3%), followed by Manchester (21.8%). The least number of respondents (0.7%) came from St. Mary and Hanover. The demographic characteristics of the sampled respondents (n = 711). There were 509 females (71.6%) and 202 (28.4%) males. The respondents' ages were as follows: 18-24 years, 210 or 29.5% of the sample, 25-31 years 183 (25.7%), 32-38 years 118 (16.6%), 39-45 years 83 (11.7%), 46-52 years 51 (7.2%), 53-59 years 43 (6%) and 60+ years 23 (3.2%).
Table 2 presents selected issues on the matter of COVID-19. The majority of the respondents (66%) indicated that they were fearful of contracting COVID-19, while 34% denied fear. The findings revealed that 536 or 75.4% of the respondents knew someone with COVID-19, 18 or 26% of the respondents reported that this caused them some feelings of fear, and 18% reported feeling very fearful. Since COVID-19, 380 (53.4%) respondents stated that they are afraid to visit healthcare facilities; however, 86% did not cancel their medical appointments, while 13% cancelled their appointments due to the fear of contracting COVID-19.
Table 3 depicts data on health behaviours during COVID-19. The findings revealed that 79.3% (n = 563) of the respondents did not exercise. Similarly, 79% (n = 561) of the respondents did not maintain a proper diet. Majority 67.3% (478) of the respondents stated they are not taking vitamins, and 32% (n = 232) stated they were taking vitamins. Majority of the respondents 60.8% (n = 432) did not do all of the above (exercise, proper diet, and taking vitamins) and only 39.2% (n = 278) of the respondents selected all of the above. Majority of the respondents 94.8% (n = 674) of the respondents changed their habits since COVID-19 to include frequent hand washing, hand sanitization and the use of masks.
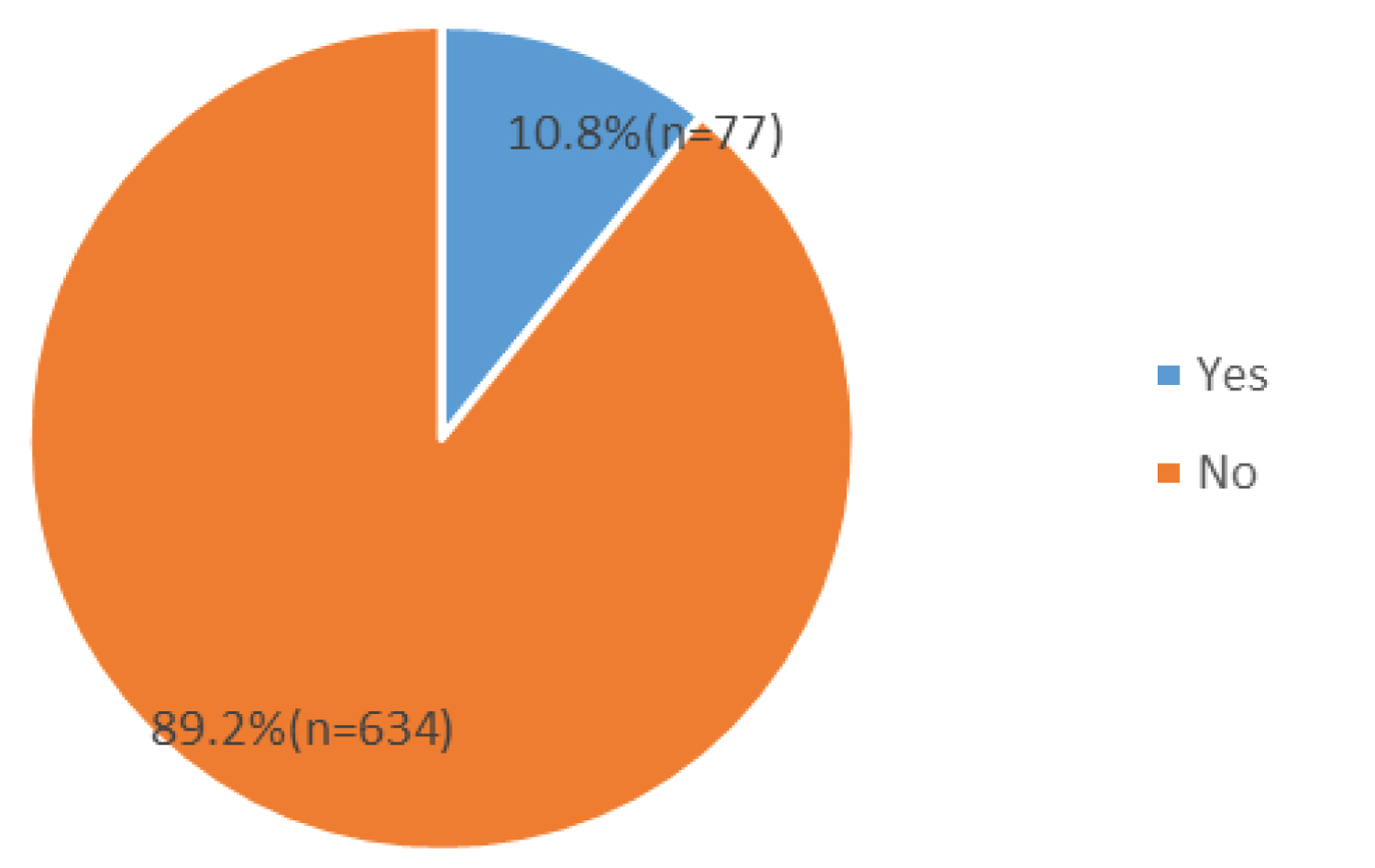
Figure 2 shows a pie chart depicting responses on whether or not respondents had a problem seeking healthcare before COVID-19. The pie chart shows that 89.2% (n = 634) of the respondents reported no problem seeking healthcare before COVID-19, while 10.8% (n = 77) stated that they had a problem seeking healthcare since COVID-19 began.
Table 4 presents a cross-tabulation on fear of COVID-19 changing Jamaicans' daily habits and health behaviours by gender.
H0: There is no statistical association between the fear of COVID-19 among Jamaicans and gender.
H1: There is a statistical association between the fear of COVID-19 among Jamaicans and gender.
Researchers used a chi-square test of independence to examine the relationship between the fear of COVID-19 of Jamaicans and gender. The findings revealed a statistical relationship between the fear of COVID-19 among Jamaicans and gender (χ2 critical = 5.024 < χ2 calculated = 6.251, P = 0.012). Since the chi-squared calculated value was greater than the chi-square critical value, we rejected the null hypothesis. The findings indicated that females (68%) are more fearful of COVID-19 than males (58%).
Hypothesis
H0: There is no statistical association between the changing of daily habits of Jamaicans and gender during COVID-19
H1: There is a statistical association between changing of daily habits of Jamaicans and gender during COVID-19
The findings from the cross-tabulation between changing daily habits during COVID-19 and gender of Jamaicans indicated a statistical relationship (χ2 critical = 5.024 < χ2 calculated = 15.419, P < 0.0001). Since the chi-squared calculated value was greater than the chi-square critical value, we rejected the null hypothesis. Even though both genders changed their daily habits, females were more likely to change their habits than males.
The cross-tabulation between health behaviours and gender of Jamaicans are as follows:
a) Hypothesis
H0: There is no statistical association between exercise and gender of Jamaican during COVID-19.
H1: There is a statistical association between exercise and gender of Jamaican during COVID-19.
The findings from the cross-tabulation between exercise and gender of Jamaicans reveal that there is a statistical association between the two variables (χ2 critical = 5.024 < χ2 calculated = 10.005, P = 0.002). Since the chi-squared calculated value was greater than the chi-square critical value, we rejected the null hypothesis. More males were likely to participate in exercise than females during COVID-19.
b) Hypothesis
H0: There is no statistical association between proper diet and gender of Jamaicans during COVID-19.
H1: There is a statistical association between proper diet and gender of Jamaicans during COVID-19.
The findings from the chi-square test between the proper diet and gender of Jamaicans revealed no statistical association between the two variables (χ2 critical = 5.024 > χ2 calculated = 0.058, P = 0.839). Since the chi-squared calculated value was less than the chi-square critical value, we failed to reject the null hypothesis. Both genders are likely to do dieting the same way.
c) Hypothesis
H0: There is no statistical association between taking vitamins and gender of Jamaicans during COVID-19.
H1: There is a statistical association between taking vitamins and the gender of Jamaicans during COVID-19.
The chi-square test between taking vitamins and gender of Jamaicans revealed a statistical relationship between the two variables (χ2 critical = 5.024 < χ2 calculated = 5.903, P = 0.016, do = 1). Since the chi-squared calculated value was greater than the chi-square critical value, we rejected the null hypothesis that more females are likely to take vitamins than males.
d) Hypothesis
H0: There is no statistical association between fear of COVID-19 and the age cohort of Jamaicans.
H1: There is a statistical association between fear of COVID-19 and the age cohort of Jamaicans.
Table 5 presents cross-tabulation between fear of COVID-19 and the age cohort of Jamaicans. The findings revealed no statistical association between the variables (χ2 critical = 14.449 > χ2 calculated = 7.745, P = 0.257). Since the chi-squared calculated value was less than the chi-square critical value, we failed to reject the null hypothesis. Therefore, there is no statistical association between age does and the fear of COVID-19.
e) Hypothesis
H0: There is no statistical association between fear of visiting health care facilities and place of residence
H1: There is a statistical association between fear of visiting health care facilities and place of residence.
Table 6 presents a cross-tabulation between fear of visiting healthcare facilities and place of residence of the sampled respondents. The findings revealed no statistical association between the variables (χ2 critical = 23.337 > χ2 calculated = 16.330, P = 0.177, df = 12). Since the chi-squared calculated value was less than the chi-square critical value, we failed to reject the null hypothesis, as there is no relationship between fear of visiting healthcare facilities and place of residence.
Discussion
Since the outbreak of COVID-19, 53.4% of the sampled respondents agreed that they were afraid of visiting any hospital or healthcare facility. However, only 13.1% stated that they had cancelled appointments due to the fear of COVID-19. Therefore, the results indicated that the fear of COVID-19 has minimal impact on health seeking behaviours. Although most Jamaicans were afraid to visit healthcare centres, only a small percentage of people cancelled their medical appointments due to COVID-19.
Researchers found that 44% of patients had delayed or avoided doctor's visits because of COVID-19 fears [39]. In this current study, 13.1% of respondents reported cancelling their medical appointments due to the fear of COVID-19. Wong indicated that higher cancellation percentages were among those diagnosed with certain chronic conditions, such as cardiovascular disease or respiratory illness. Both are risk factors for poor outcomes. Fear of coronavirus outbreaks has driven a public perception of all medical facilities being germy and overrun with highly contagious COVID-19 patients [39].
Based on our survey, the findings revealed that 66% (469) of the sampled respondents are fearful of contracting COVID-19. More than 70% stated that they knew someone who had contracted COVID-19. When asked how this made them feel, 18% (128) expressed that they were very fearful, while 26.7% (190) are somewhat fearful. 69.8% of our respondents who expressed fear of COVID-19 were females, while 30.2% were males. These results indicate that the level of fear among Jamaicans increased since the COVID-19 pandemic.
In our study, there was no statistical relationship between fear of Coronavirus and age. Therefore, regardless of age group, the fear of COVID-19 among Jamaicans was moderately high, as an average of 66% (469) across all age cohorts were fearful, while 34% (242) were not fearful. The current study provided quantitative research data on the extent of fear among Jamaicans during COVID-19 and its influence on health care seeking behaviours. In a study conducted by Wang, et al. results showed that females suffered a more significant psychological impact from the outbreak of COVID-19 and higher levels of stress, anxiety, and depression than men during the COVID-19 pandemic. This research corroborates our findings that females (69.8%) are more fearful of COVID-19 than males (30.2%).
Analysis of the collected data for this study found that 94.8% (674) of the sampled respondents adapted to the current pandemic by including COVID-19 protocols in their daily lives. These include frequent hand washing, hand sanitization, and the use of masks. Our findings also reveal that females, accounting for 69.3% (493) of respondents, were more likely to change their habits to adhere to COVID-19 protocols.
One study explored the patterns of adherence to COVID-19 mitigation measures. Researchers found that participants from vulnerable populations took steps to increase efforts to protect themselves or vulnerable household members. Many of the participants who considered themselves or their households to be at risk and felt that the risk of exposure to the virus was high, reported engaging in additional preventive measures to safeguard themselves and their families [40].
The current study revealed that 18% expressed that they were doing none of the above. Furthermore, the comparison between gender and health behaviour revealed that females were more inclined to take vitamins than males. For exercise, males were more dominant in this aspect, as 28.4% stated they exercised to maintain health, while 17.7% of females said the same. Regarding proper dieting, no significant statistical difference emerged between both genders, as males were 20.4% of the respondents while females were 21.2%. This result indicates that only a few Jamaicans were maintaining a good health status during COVID-19 within the targeted population. The results indicate that proper dieting and exercise are correlated because the respondents who participated in exercise were more likely to maintain an appropriate diet and vice versa. This current research showed that 79% of the participants were not engaged in either exercise or maintaining a proper diet and 67% were not taking vitamins.
Limitations
This research is not without limitations. Even though a maximum of 1,067 respondents was desired, researchers only received 711 responses, which was relatively small for an online study. This limitation may have resulted from not having the survey widely disseminated. Therefore, the survey had limited responses from various parishes such as Portland (2.3%), Hanover (0.7%) and St Mary (0.7). The sampling method of this study limits the ability to generalize to the wider Jamaican population, as the sample size may not be representative of the larger population.
Another limitation is disproportionate representation among genders. There were more female respondents than males. Studies on survey responses found that women are more likely to participate in online surveys than men (See Curtin et al., 2000; Moore & Tarnai, 2002; Singer et al., 2000). Therefore, a sample that includes an equal number of men and women would make findings more generalizable and further explore gender differences.
Conclusions
This study is a descriptive one and while an empirical model would provide more information on the factors affecting healthcare seeking behaviour inclusive of fear; this was not the purpose of the current study. From the results of the study, it can be concluded that respondents did not maintain a proper diet; are not taking vitamins; did not practice health principles such as exercise, eating proper diet, and taking vitamins; changed their habits since COVID 19 to include frequent hand washing, hand sanitization and the use of mask.
From the chi-square statistic it can further be concluded that females are more fearful of COVID-19 than males, females were more likely to change their habits than males, males were likely to participate in exercise than females during COVID-19, and females are likely to take vitamins than males. Therefore, the null hypothesis that did not show any statistical association between gender and the mentioned variables was rejected.
With the emergence of COVID-19, fear has become a prominent variable and a possible barrier that affects health-seeking behaviour. Our research revealed that most Jamaicans are indeed fearful of COVID-19. However, this fear has minimal influence on them seeking healthcare. However, it is essential to note that most Jamaicans have not maintained their health during the pandemic.
Recommendation
Thus, Ministry of Health and Wellness should commence promoting health and wellness in addition to health promotion during COVID-19.
References
- (2019) 2009 H1N1 pandemic (H1N1pdm09 virus). Centers for Disease Control and Prevention.
- Howard J (2020) Plague was one of history's deadliest disease-them we found a cure. National Geographic.
- Saul T (2021) Inside the swift, deadly history of the Spanish flu pandemic. National Geographic.
- Shipman PL (2021) The bright side of the Black Death. American Scientist 102: 410.
- Jarus O (2020) 20 of the worst epidemics and pandemics in history. Live Science.
- Mohan BS, Nambiar V (2020) COVID-19: An Insight into SARS-CoV-2 Pandemic originated at Wuhan city in Hubei province of China. J Infect Dis Epidemiol 6: 146.
- Song F, Shi N, Shan F, et al. (2020) Emerging coronavirus 2019-nCoV pneumonia. Radiology 297: E346.
- Nkengasong J (2020) China's response to a novel coronavirus stands in stark contrast to the 2002 SARS outbreak response. Nat Med 26: 310-311.
- Zhu H, Wei L, Niu P (2020) The Novel Coronavirus Outbreak in Wuhan, China. Glob health res policy 5, 6.
- Cucinotta D, Vanelli M (2020) WHO Declares COVID-19 a Pandemic. Acta Biomed 91: 157-160.
- (2021) WHO Coronavirus (COVID-19) Dashboard.
- (2021) Clinical Management Summary for Wednesday, December 29, 2021. Ministry of Health and Wellness.
- (2020) WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020.WHO.
- Tuncer FF (2020) The spread of fear in the globalizing world: The case of COVID-19. Journal of Public Affairs e2162.
- (2021) Mental health and COVID-19. World Health Organization.
- Muller A, Himmels J, Van de Velde S (2021) Instruments to measure fear of COVID-19: A diagnostic systematic review. BMC Medical Research Methodology 21.
- Sit S, Lam T, Lai A, et al. (2021) Fear of COVID-19 and its associations with perceived personal and family benefits and harms in Hong Kong. Transl Behav Med 11: 793-801.
- Oberoi S, Chaudhary N, Patnaik S, et al. (2016) Understanding health seeking behaviour. J Family Med Prim Care 5: 463-464.
- Madu D, Edwards D (2020) COVID-19 and its impact on care of non-virus patients.
- Brunier A , Harris M (2020) COVID-19 significantly impacts health services for noncommunicable diseases. Washington DC: WHO.
- Tan H, Tan M, Chang Z, et al. (2021) The impact of COVID-19 pandemic on the health seeking behaviour of an Asian population with acute respiratory infections in a densely populated community. BMC Public Health 21: 1196.
- Chileshe M, Mulenga D, Mfune RL, et al. (2020) Increased number of brought-in-dead cases with COVID-19: Is it due to poor health-seeking behaviour among the Zambian population?. The Pan African Medical Journal 37: 136.
- Latunji O, Akinyemi O (2018) Factors influencing health-seeking behaviour among civil servants in Ibadan, Nigeria. Ann Ib Pg Med 16: 52-60.
- Czeisler M É, Marynak K, Clarke KE, et al. (2020) Delay or Avoidance of medical care because of COVID-19-related concerns - United States. Morb Mortal Wkly Rep 69: 1250-1257.
- La Morte W (2019) The health belief model.
- Kanbarkar PN, Chandrika K (2017) Health care seeking behaviour- A theoretical perspective. Paripex Indian Journal of Research.
- Broche-Pérez Y, Fernández-Fleites Z, Jiménez-Puig E, et al. (2020) Gender and fear of COVID-19 in a Cuban population sample. Int J Ment Health Addict 12: 1-9.
- Walker LJ (2004) Components of the health belief model and HIV testing decisions. A Thesis Submitted to the University of North Carolina at Wilmington in Partial Fulfilment Of the Requirements for the Degree of Master of Arts Department of Psychology University of North Carolina at Wilmington.
- Mertens G, Gerritsen L, Duijndam S, et al. (2020) Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J Anxiety Disord 74: 102258.
- Wheaton MG, Abramowitz J, Berman N, et al. (2011) Psychological Predictors of Anxiety in Response to the H1N1 (Swine Flu) Pandemic. Cognitive Therapy and Research 36: 210-218.
- Blakey SM, Abramowitz JS (2017) Psychological predictors of health anxiety in response to the zika virus. J Clin Psychol Med Settings 24: 270-278.
- Saah F, Amu H, Seidu A, et al. (2021) Health knowledge and care seeking behaviour in resource-limited settings amidst the COVID-19 pandemic: A qualitative study in Ghana. PLoS One 16: e0250940.
- Mishra D, Alok D (2017) Handbook of Research Methodology 1st edition. EDUCREATION.
- Rea LM, Parker RA (2014) Designing and conducting survey research: A comprehensive guide. 4th edition. John Wiley & Sons Inc.
- Babbie E (2010) The Practice of Social Research 12th edition. Wadsworth, a Division of Thomson Learning, Inc.
- Creswell JW (2014) Research design qualitative, quantitative and mixed methods approaches. Los Angeles: Sage.
- Neuman WL (2014) Social research methods: Qualitative and quantitative approaches, 7th edition. Pearson/Allyn and Bacon.
- Bourne Paul A (2021) Planning institute of Jamaica (PIOJ), Statistical institute of Jamaica (STATIN). Jamaica survey of living conditions. Kingston: PIOJ, STATIN 4: 2.
- Wong E (2020) Fear of COVID-19 keeps patients from seeking medical care.
- Denford S, Morton K, Lambert H, et al. (2021) Understanding patterns of adherence to COVID-19 mitigation measures: A qualitative interview study. J Public Health (Oxf) 43: 508-516.
Corresponding Author
Paul Andrew Bourne, Acting Director of Institutional Research, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI.
Copyright
© 2022 Bourne PA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.