Sensing Devices to Aid Coaches and Sports Training of People with Motor and Intellectual Limitations
Abstract
There is a growing development of systems using IoT involving the training and monitoring of people with special needs. These sensing techniques are important to guarantee the correct analysis of the information. Also, these systems aim to provide parameters for the coach while tests and activities are performed by the selected individuals, whether these people are athletes, a person doing a rehabilitation program or a group with special needs. This work presents the development of a coaching system for people with motor and intellectual disabilities integrating IoT technologies for reading the data and transmitting to the cloud, in order to be analyzed by the coach remotely. This application allows the trainer to obtain the information online and intervene on the test process, organizing the individuals into homogeneous groups based exclusively on their performance characteristics. To perform the tests, the individuals were selected and divided into subgroups, and the tests were conducted using the equipment developed by the authors. For each group, the necessary adaptations were made in the equipment to meet the existing limitations, and the protocols for each case were also defined. With the correct use of the equipment and the appropriate protocol, positive results were obtained, with averages of improvements above 31% in some cases. This work aims, to demonstrate that the developed equipment can be used to assist the trainer in the activities with different public, based on the results obtained. Also, future devices are being studied to continue this research.
Keywords
IoT: Intellectual Disability, Physical disability, Sports training
Introduction
The development of systems for coaching and monitoring involving people is a growing area, which involves sports applications, rehabilitation, and people with special needs [1,2]. The advance is due to the development of sensor techniques and information processing, such as the Internet of Things (IoT) [3-5]. As a first step, the sport sensing systems requires a data acquisition to detect movements (using infrared sensors), to obtain variables such pressure and force (applying piezoelectric, piezoresistive, and capacitive sensors), and capturing bioelectric signals (with the use of electrodes). Although these mentioned sensors have simple features, the data fusion that they provide allows coaches and specialized people to make knowledgeable decisions about the training of their athletes and/or their population, using techniques such as IoT [6].
These sensing technologies impact the sports equipament development, improving practices and performance of athletes [7], which benefit with IoT. For starters, IoT for sports applications is related to data acquisition process, performance and movement tracking of athlets, and in coaching techniques. One factor that justifies the adoption of this method is paid attention to the health of an athlete, e. g., application to monitor the risk of injuries among soccer players, using sensors to aquire different types of data (body temperature, body motion, sweat, heart, and respiratory rate, besides temperature and illuminatiom from the environment) [8], mobile applications for neuromuscular and neurocognitive tests to evaluated the risk of lesion [9], and vertical jump analysis with smart watches, cameras, and EMG to avoid injury risk [10]. IoT systems to aid in coaching is a field that are starting to be explored and still has fewer applications. Among them, one can cite a framework, used to coach badminton where wearable inertial sensors, located on the wrist , are used to recognize three player actions (smash, clear, and drops) in several levels from different players [11]. Other application uses an IoT system envolving a balance board for ski coaching with a video game [12].
Thus, IoT Systems are increasingly in use and provide the device to acquire and store data for a remote processing [4], improving the decision-making of the coach. The possibilities with the use of IoT technologies applied in coaching are not only focused on the information obtained, sent, and saved, but the opportunity to allow a better decision-making during the training process. It allows the coaches to monitor theirs groups remotely and reassemble them to adjust their actions and activities. A differentiated proposal for this application is to allow the trainer to analyze a heterogeneous population (people with motor and mental disabilities, for example), obtaining information from systems and equipment with those technologies. This can support a development of a better program to improve the results and achieve homogeneous results for all individuals.
Focused on that, this work presents the development and application of equipment using low-cost sensors, capable of being applied to diverse audiences, including intellectually and physically disabled, integrating IoT sensing technologies. Among their differentials, the systems present their results online, sending their data to a cloud storage that allows remote monitoring.
Virtual Coaching and Special Groups
Virtual coaching
The use of the Internet in an everyday life has changed the society. Currently, there are several aspects of our lives that are determined by it, essentialy because of the easiness to obtain and use a smartphone. Cellphones are widely consumed because of their simplicity, since they are inexpensive and have an easy-to-understand interface. Because of this, the advantages of using a mobile handset technology have been growing significantly and covering many areas such as health, entertainment, and education [13,14].
In the health area, personal training and monitoring using applications has become a common and efficient methodology, since programs target individualized performance improvement [15]. This practice has been disseminated not only for personal training, but also for high-performance sports and for specific training of special groups. Thereby, in 2012, only 41% of the training sessions were conducted in person, 31% were made by using a telephone, 14% with video calls with webcams and Skype, 11% as an e-mail, and 3% using high quality video calls [13].
This fact highlights the need to develop technologies that provides online and remote training, so that more people can conduct the tests at the same time and there is no lack of monitoring from the physical education professionals. However, in addition to the technology involving techniques such as IoT, to be able to merge the application with the equipments, the devices requires a development focused on the internet compatibility, so it will be able to connect and send data to the cloud [14].
Nevertheless, besides the equipments, one must know the characteristics of each audience to be approached. Each individual, even in similar groups, has its own particularity, which directly affects the use of a predetermined protocols that will require to be reviewed and adapted. Furthermore, for people with intellectual or physical disabilities, adaptations and caution should be even greater, since they may need a subdivision so they can improve their abilities more homogeneously [16]. This may be more evident when a group of individuals are coached together (para-Olympic sports), even tough they present distinct locomotive and/or intellectual restrictions, different levels of autism or other mental limitations. For this reason, it is important that the coach is prepared and fully understands the peculiarities of each group, as well as how to process the information efficiently.
Thus, with the correct acquisition and quick transmission of the data, the Physical Education or Physiotherapy professional has the possibility to idealize a personalized training program, increasing not only the quality of life, but also the performance of each person.
Special groups
In order to have a good applicability of the technological equipment focused on physical evaluation, as well as to allow coaches and health professionals to analyze the performance of their athletes in a remote and online way, it is necessary to know the specific performance characteristics of a variety of public. This information is important to evaluate the correct training application, modify the protocols, and also adapt the devices. Therefore, to gather more data and comprehend the aspects of some particular individuals, this research focused on working with a more specific audience, defined by a heterogeneous group diagnosed with intellectual and physical disabilities.
Intellectual disability
According to the American Association on Intellectual and Developmental Disabilities (AAIDD), Intellectual disability (ID) is defined as a deficiency characterized by significant limitations in both intellectual functioning (learning and problem solving), and in adaptive behavior, which is related to daily functions needed to work, have fun, and live in a community [17]. In Brazil, 0.9% of the population between birth and 14 years of age have ID [18].
Diagnostic and Statistical Manual of Mental Disorders (DSM-5®) are used by clinicians and researchers to diagnose and classify mental disorders [19].
To classify the individual who has ID, it is common to use the Intelligence Quotient Test, or I.Q. In addition to analyzing the classifications from this test, we must also take into account the classification of adaptive behaviors.
• Mild and Moderate ID: Classification between 70-55 and 55-40, according to the results of the I.Q. test. Regarding the adaptive aspect, the individual who has mild and moderate ID presents a deficiency in the ability to communicate and have social contact, as well as a slight sensory motor delay. The focus of this problem lies in developing ideas and solving problems.
• Severe ID: Results of the I.Q. test below 25. Individuals in this category have a major impairment in speech and motor development, and may even be unable to communicate, making them totally dependent. In addition, they may present a balance problem, causing them to move with difficulty.
In addition to the classification with the I.Q. Test, it is necessary to apply further tests to verify possible subgroups among the individuals analyzed, so that a better distribution and adaptation of the tests can be performed. These subgroups can be identified accordingly to a verification of different deficiencies, such as visual or auditory disabilities, or even an advanced motor impairment [16].
Children with ID have a cognitive delay that directly affects the speed of their cognitive and motor skills. However, studies have shown that by attending to the mental and motor skill needs of children with ID, it is possible to reduce their motor delay [20] and achieve a satisfactory level of development for some tasks [21]. Thus, it is possible to provide a better experience for all the individuals and also ensure that better results are achieved.
Physical disability
Physical disability is defined as one that affects the mobility of a person. Someone with a physical disability may need to use some type of equipment to assist with their mobility. It is also characterized as a physically disable individual, someone who lost limbs or who, due to a variation on some part of the body, requires small adaptations so they can have an active participation on society [22].
Generally, what is most recurrent to people regarding physical disability is a paraplegic or quadriplegic deficiency. The first one results from a spinal cord injury, occurring below the neck, while the second one is often related to damage to the spinal cord in the neck. These both deficiencies can result from various degrees of limb loss and other conditions. There are also other ways to be physically disable, such as from the result of polio, cerebral palsy (damage to brain tissue during fetal stages), and some genetic conditions [23].
Materials and Methods
This section will present the developed equipment and their modes of operation, in addition to presenting the concepts and benefits of using the Internet of Things. The methodology that were used to apply the tests with the individuals who participated in this research is also presented. The equipments presented here can be used with different public, from people with physical disability to professional athletes for example, without the need for significant constructive modifications.
Equipments
Each equipment used for this research was developed at the Center of Studies in Instrumentation in Biomedical and Sports Engineering (CIEBE), at UTFPR Ponta Grossa. For all of them, after a evaluation and definition of the design requirements (response time of sensors, consumption and autonomy, need for signal conditioning, among other parameters), one of the main objectives of the development was to seek the use of low cost sensors (lack of financial resources is a critical problem in the reality of many societies) that, despite their low cost, present a reliable response [24].
For the developed devices that will be presented next, the microcontroller ATmega2560 was used because it has a 16 MHz crystal oscillator, it has 54 I/O pins which are enough to attend all the peripherals that make up the devices, besides having the capacity of storage for the existing routines and for new routines that can be integrated later.
Different types of sensors have been analyzed for use in the devices such as capacitive sensors, which provide accurate values but are capable of detecting only distances of a few centimeters and are costly when compared with other sensors. Ultrasonic sensors, which would be able to detect the distance required for this application, were also analyzed, but the response time presented is not satisfactory for use in the developed devices. Finally, it was verified that photoelectric sensors meet the established requirements for correct operation of the equipment.
There are various types of photoelectric sensors such as barrier sensors, in which emitter and receiver are aligned and detection occurs when the light beam formed between them is interrupted by a person or object, and also diffuse sensors, in which emitter and receiver are in the same enclosure, and the light reflection on the object or person in front of sensor performs the detection. The infrared sensor in diffuse mode (IR) with adjustable sensing distance (3 to 80 cm) was chosen for these equipments. As main characteristics, they have an acceptable time response (less than 2 ms), relative small sensing angle (less than 15 degree), low electrical power consumption, which reflects positively on the autonomy, and are a low-cost sensor.
Action time test device (ATTD)
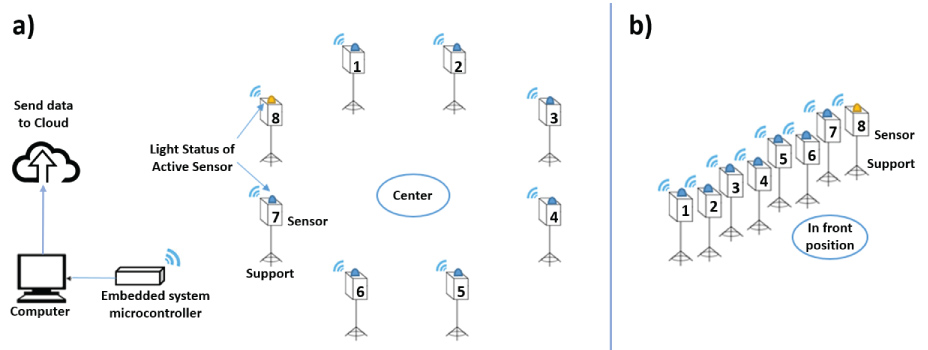
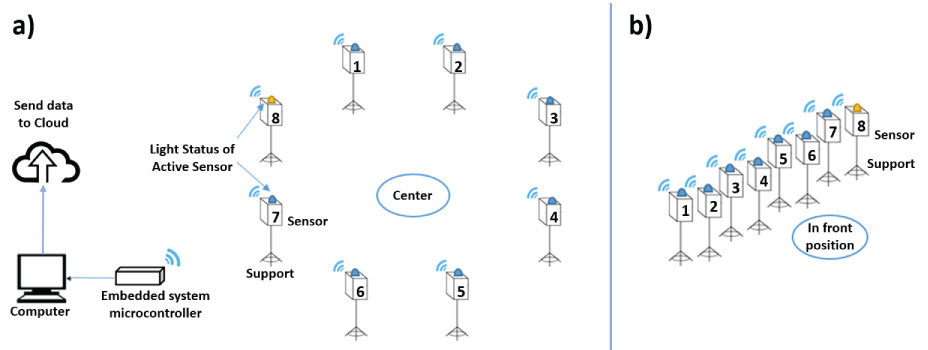
To obtain an action time of an individual, the ATTD was developed. The purpose of it is to assist in the evaluation of a response capacity performed by a user. It consists of a control unit that is responsible for managing and monitoring the sensor terminals, which has a Bluetooth communication with a PC for eventual connection to the Internet.
The device can be used with four different modes of operation, described by a random routine, sequential routine, random routine with a preset time, and a preset time random routine with error detection. The equipment can be used with 3 to 8 sensor terminals installed, determined by the needs of the evaluator, as shown in Figure 1.
The sensor terminals are provided with indicative lights. When the sensor terminal is activated, a green LED is lit for visual indication. The subject should approach his or her hand at a shorter distance from the sensor than the one set (adjusted by us by 10 cm) so that the control unit receives information from the individual's passage. By doing that, the green LED is turned off and a red LED is lit, indicating that this terminal is not currently active. After that, a new sensor terminal is activated by the control unit.
From the moment that the system is started, the control unit counts the time elapsed between the activation of each sensor terminal and the passage of the user through it, which corresponds to the moment when the user identified the active sensor terminal and moved to block the signal emitted by the sensor. The evaluator is able to define the number of steps that each user must take. After the test is finished, the data is both saved to a memory card and is available to be analyzed on the application using a smartphone.
The sensor terminals can be positioned in different forms accordingly to the characteristics of the person taking the test or the need of the coach. Some forms determined to be used with the selected groups was in line, in a circle, and in a form of an arc. In addition, the protocol used can be changed with each new test and can be observed from Figure 2, Figure 3, Figure 4 and Figure 5. These different modes of operation are explained as follow:
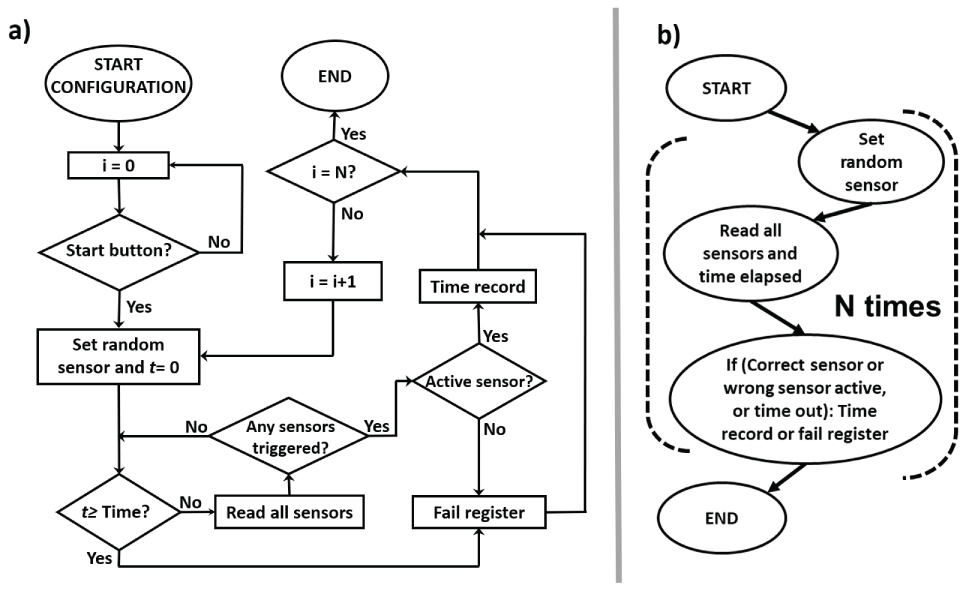
• Random routine: The control unit will randomly activate one of the connected sensor terminals, and wait until the user performs the passage through it. Then, another sensor is activated and the central saves the elapsed time and which sensor terminal was used for each stage. Figure 2a ilustre the technical and detailed flowchart and Figure 2b the intuitive and simplified flowchart.
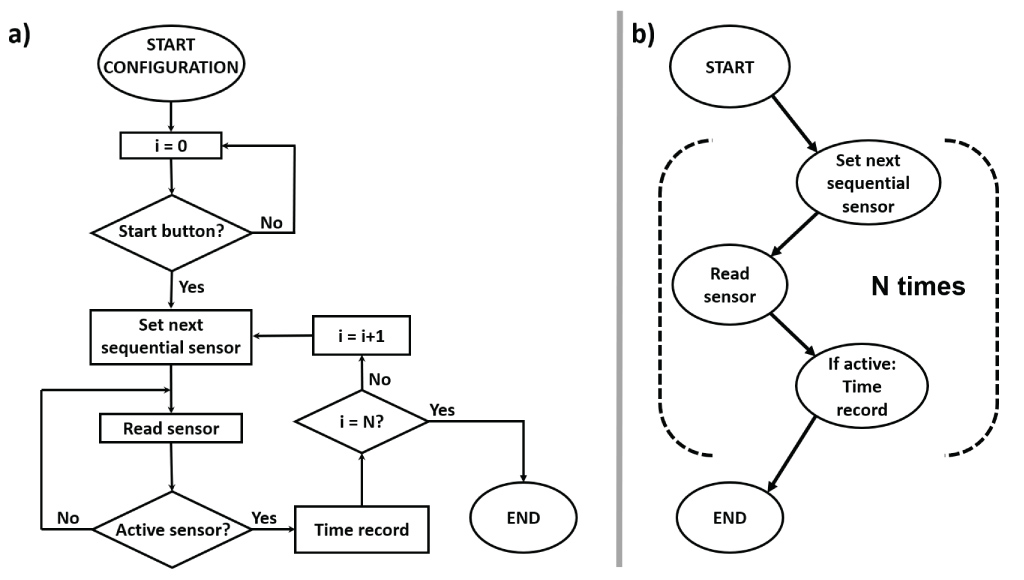
• Sequential routine: The control unit activates the sensor terminals in an increasing sequence, from sensor terminal 1 to the last sensor terminal that is connected, until the set number of steps is reached. Figure 3a ilustre the technical and detailed flowchart and Figure 3b the intuitive and simplified flowchart.
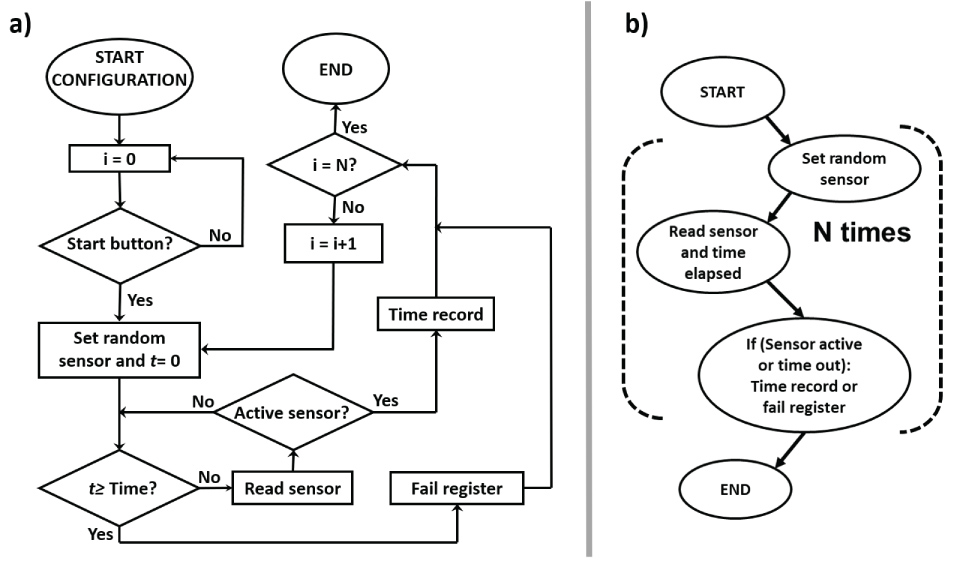
• Random routine with a preset time: For this protocol, the control works in the same way as in the random routine, but the user must be able to reach out to the sensor in a certain time defined by the coach. If the user cannot complete the action, the control unit activates another sensor terminal and records the previous information with a "fail" result. Figure 4a ilustre the technical and detailed flowchart and Figure 4b the intuitive and simplified flowchart.
• Preset time random routine with error detection: Similar to the previous one, this routine complements the monitoring of all the terminals, regardless of which one is activated, to identify if the user makes the passage through a wrong sensor (not activated at that time). When the timeout is exceeded or the user passes through a wrong sensor terminal, this information is saved by the control unit. Figure 5a ilustre the technical and detailed flowchart and Figure 5b the intuitive and simplified flowchart.
The application then receives via Bluetooth the information and performs the processing of the data to provide a comparative graph of the action times between the selected users. This graph, in addition to detailed elapsed time information, is available so that the evaluator can remotely analyze the data and compare the results. To do so, the application must be installed in a smartphone with an active connection to the internet.
Sprint time test device (STTD)
This device is able to electronically control the evaluation process of a sprint realized by one or more athletes in a predetermined distance. To do so, the equipment is responsible for measuring the time spent on a particular physical activity (sprint or race). The time recorded can be correlated with the performance of the athlete in this particular activity. This variable has long been used in a variety of physical evaluation protocols, mainly to obtain physiological factors such as anaerobic and aerobic power and fatigue index.
The STTD uses a photoelectric sensor unit that capture the passage of the athlete with high precision, thereby determining the start and the end of the timed activity. To illustrate the importance of measuring the correct time that the athlete spends on a given physical activity, the evaluation protocol denominated RAST (Running Anaerobic Sprint Test) is used to determine the anaerobic power output (peak and mean) of the athlete, equation (1). This protocol consists on running six times a distance of 35 meters in the shortest possible time. For each try, the athlete must start in a still position, and rest for 10 seconds between every test [25]. The power measured [Watts] is composed by three values: Mass [kg] of the athlete, distance [m] of the test, and the time [s] spent.
In addition to the power output, the same protocol can determine the fatigue index of the athlete related to the physical activity, equation (2).
With those collected values, it is possible to develop a training program to improve the performance of the athlete or to target and enhance a particular activity. However, to be able to do that, the data collection of the time needs to provide precision, functionality, and credibility.
The logic implemented is presented by the detailed flowchart as shown in Figure 6a, while the simplified flowchart is ilustrated in Figure 6b. There are three variables, two to identify the sensors being used and one called FLAG (auxiliary variable). After reading the status of the sensors, the device compares them and make a decision: To trigger or to cease the stopwatch. Both sensors can trigger or cease the stopwatch that only depends on the status of the FLAG. If the FLAG has a low value, the stopwatch will be triggered. If the FLAG has a high value the stopwatch will be stopped.
Internet of Things (IoT)
The concept of virtual training can be defined as being all the action that a given device can perform to assist the development of a physical activity. In this scenario, the devices may present the feedback from the actions of the user to the trainer, just enough do develop a series of exercises. On the other hand, sensing systems (with information feedback) can be used so that a series of exercises can be monitored an/or managed remotely. These remote activity monitoring devices uses communication systems and allow professional people to access the data collected and stored in the cloud, so they can analyze, process these data, and interfere in these remote processes [4].
This process of remote access is one of the foundations of IoT, in which things (in this case, sensors), are monitored and their data is collected by a device connected to the internet, which can operate as a data server (cloud) or as a communication device with other servers. On the other hand, mobile devices with Internet access can aquire the data from these services at any time and provide their analysis [26]. In this scenario, the application of the IoT technology within health care applications, and even in sports, has been highlighted by promoting interactivity in a remote and effective way [27,28].
Therefore, the entire application was developed using IoT, and each sensor was connected to the internet. From this connection, the signals were sent to a cloud system, in order to reach the trainer.
Application for online communication
To perform the communication between the equipment and the cloud, a LabVIEW™ application was developed in order to receive the data from the devices, perform the processing, and separate the information of each user in different tables. Furthermore, the app generates a comparative graph between the users for overall performance verification. After processing the received data, they are directed to an online server where they are stored.
A smartphone application has also been developed to remotely receive the data stored on the server and display them on the screen. The data with the individual performance of each user is shown, as well as the graph that compares the selected users. This functionality allows a deep analysis by the coach and a possible division of users in subgroups accordingly to their performance.
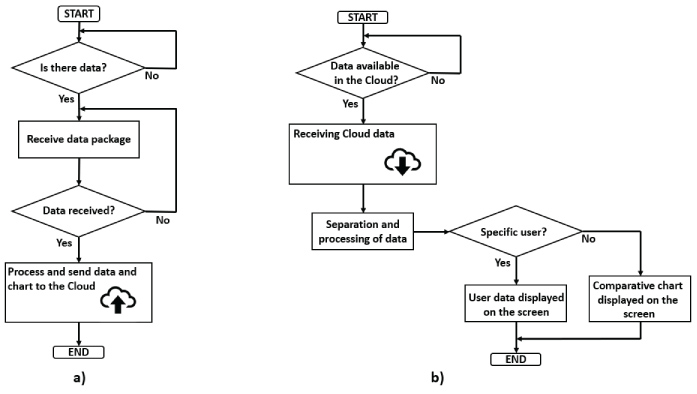
The simple access to the application on a smartphone with internet connection allows the evaluator to view the data obtained in the training. Besides, the coach can select the desired user so the specific data will be displayed, or choose more than one user to get a comparative chart. For a better understanding of the application, Figure 7 illustrates the flowchart of its operation.
Methodology
Device development
For the development of the equipment, it was initially verified the demand presented by physical education professionals, aiming to create an initial basis of the functions that the devices should present. After that, the authors tried to adapt the constructive aspects of the equipment , verifying the specifications, such as modes of operation, reliability, and low cost, which were defined as prerequisites to guide the development. With the assembled prototypes, initial tests were performed to ensure the correct functioning of the devices, as well as to verify the need for modifications to be made to attend the public that would participate in the research.
Recruitment of public
Knowing the main characteristics of individuals with ID, a group of twenty children from the Association of Parents and Friends of the Exceptional (APAE) in the city of Ponta Grossa/PR/Brazil was selected to perform the tests using the equipment. As a result, it was possible to identify adaptations on both the test protocol and the devices. For the application of the equipment with physically disabled people, a group composed by nine wheeling basketball athletes in a team located in the city of Ponta Grossa/PR/Brazil was selected. The use of the wheelchair of this specific public can be resulted from many factors, such as cerebral palsy, an accident or congenital diseases.
Experimental application
As mentioned before, each classification of the I.Q. test has its own peculiarity, which implies adaptations on the protocols for each of the tests. In addition, after an initial analysis with the groups of people with ID, subgroups of individuals with similar characteristics were defined so it would also focus on those with visual or motor disabilities, besides the results of the I.Q. test.
Thus, for those with mild and moderate disabilities, equipment adjustments did not have to be performed, but there was an improvement on the protocol. These individuals have a difficulty in developing ideas and solving problems, so the test should be explained in a clear manner, and the children should be enable to do the tests as a training before actually performing them.
However, for individuals with a severe ID, there is a need to change the protocol and make adjustments in the devices. Due to the fact that these children have balance problem, the sensors should be fixed on the floor to avoid falls, intimidation, and damages to the equipment. In addition, these children have a hard time keeping their attention on something for a long period of time. Therefore, an auxiliary sound stimulation needs to be added to the visual stimulation.
These modifications also included the two subgroups that were identified during the tests, that are children with motor and visual impairment. For those with intellectual and visual impairment, the brightness of the room should be reduced and the sound stimulation facilitates the application of the tests. For those with motor and ID, the fixation of the sensors at a reduced distance allowed their correct motion and testing.
Thus, among the twenty children selected for the test, five groups were separated with different protocols for each one. In total, eight tests were performed over four months in order to follow the performance of each individual.
For the group of wheelchair athletes, the adaptations of the protocols were simpler, so as to meet the need of them all. Thus, for the ATTD, the sensors must be arranged in a circle, fixed to the ground and with a radius of two meters. This allows a comfortable movement of the parathletes without the wheelchair being able to knock down the sensor units. Regarding STTD, the height of the device should be adjusted to the height of each individual, ranging from 60 to 70 cm in order to standardize the triggering moment of the sensor.
After discussing the characteristics of the group with physical disability, the tests were performed with nine athletes twice a month, in a period of three months. However, due to the calendar of games and personal difficulties, only four athletes participated on the majority of the tests.
Furthermore, all protocols could only be adapted and performed efficiently due to the use of IoT technology, since the coach had access to the data remotely and was able to determine the changes that had to be made. To illustrate the execution of the tests, the Figure 8 shows the development of some of the monitored exercises.
It is important to emphasize that the devices developed and used in this research have only and aid functionality, being the responsibility of the coach to carry out the triage of the people who participate in the tests as well as to evaluate the performance. Thus, he can perform possible interventions and provide an opinion or diagnosis from the data obtained.
Results
The development of the application to consult data remotely (IoT application) during the tests was made with an open source code, to an Android platform. An example of the user interface is shown in Figure 9, as well as how the information is provided to the coach during a data collection of a specific user. The information, as mentioned before, can also be analyzed using graphs with the results distribution of the selected users. These graphs were obtained using the Fusion Tables available on the Google Drive platform and presented to the app user. However, they could also be made using LabVIEW™ processing or directly with Excel.
After completing the tests with the ID children, the graphs showed in the Figures 10 and Figure 11 could be drawn, identifying each person as a letter. The graphs show that the correct application of the tests, using devices that enables different groups of people to perform and allows coaches to remotely intervene with the tests, could be a way to improve the quality of life of some individuals.
As mentioned before, the children had to be divided into five groups accordingly to their specific characteristics. In Figure 10a, the group of five children were arranged as with mild ID. For Figure 10b, nine individuals were identified as having moderate intellectual deficiency. For those with severe ID, the results are shown in Figure 11a.
Four children could not be placed with the classification of mild, moderate, and severe ID because they also presented visual or motor impairment. For this reason, the results from these children were separated into two different graphs, showed in the Figures 11b and Figure 11c.
From the results collected with the ID individuals, it was possible to obtain Table 1, showing how they were separated and the total population studied.
For the physically disable group (wheelchair players), the results are showed in Table 2, with the action time, and Table 3, with the sprint time. Both tests, using the ATTD and STTD, were performed at the same day so their game practices would not be compromised. Even though the dates of the tests were predetermined, some of the parathletes did not perform all the evaluations. Because of that, the results are focused on the four individuals that participated in all the tests.
Discussion
Group of ID individuals
The results obtained in Figure 7 and Figure 8 showed that in all the groups there was a significant performance improvement, characterized as a decrease in the action time for all individuals.
In particular, two major considerations can be discussed. The first relates to the individuals with mild and moderate intellectual disabilities. Both groups had decreased the action time in about 3500 ms by the end of the tests. By visualizing that, the first grouping of the population does not need to be related to their I.Q. results but to their performance during the tests. On the other hand, individuals placed in different groups can be allocated into one group only. This is one case about individuals who had similar results with visual and motor impairment.
Analyzing the results of the average performances based on the groups, we can affirm that the group with mild ID obtained a mean performance improvement of 20.09%, with only one child showing an improvement much lower than the average, 6.2%, justifying the group change. On the other hand, the group with severe ID showed a performance improvement of 4%, with a one particular child achieving a result inferior to 4 seconds. This also presents an opportunity for this child to change groups. For the group with visual disability, there was an average improvement of 24.53%, where a child also presented a performance below 2.5 seconds, justifying its redistribution. Finally, the children with motor disability showed an average improvement of 31.48%.
Physically disable group
In the group with physical disability the tests were not performed by all the athletes. For this reason, the results vary between an improvement and a decline of their performance. However, it is possible to notice that with a correct training and regular application of the tests, the system could allow the parathletes to enhance their abilities and renovate training techniques applied to them.
However, based on the Table 2 and Table 3, it is possible to notice that the athletes performing the action test presented an average performance improvement of 11.02% at the end of the training period. Also, for the sprint time, there was a 17.38% improvement on the average performance.
The devices as an aid to the trainer
The results obtained with the two groups participating in the research show that, despite being formed by heterogeneous individuals, they improved during the tests. However, the devices used only have the function of assisting the trainer in the work to be carried out with the groups, being of fundamental importance the capacity and experience of this professional to analyze the obtained data and to direct the training and protocols used.
For heterogeneous groups, it has been shown that the devices can help in the classification of the individuals, thus allowing a redistribution of the groups in order to optimize the individual and group performances, since the training can be directed in a specific way.
In this way, it is verified that an equipment like the one proposed, aims at assisting a group of professionals of the area of physical education (coaches), and does not intend to substitute them, since the sensitivity for decision-making comes precisely from the experience. However, the use of electronic devices aims to improve the service to groups of users, allowing the coaches to optimize their training, focusing on performance. Thus, the objective of this study is to demonstrate the feasibility of using the devices to aid the trainer, and the benefits derived from such use, therefore, the fact that the application of the tests was performed and the results obtained demonstrate that the goal was achieved.
Conclusions
In this research, systems using low-cost sensors were presented to assist the training of people with motor and intellectual disabilities applying IoT. The systems presented have sensors that are connected to the internet and provide, through data recording into the cloud, the information so that the coach can follow the development of the activities and interfere during the training.
These systems require a homogenization of groups during the activities, especially those with disabilities and special needs. Thus, the grouping occurs not only by the physical or mental limitations of the individuals but also by their abilities and difficulties, improving aspects on their personal life.
It is clear that the efficiency of the performance improvement results are a combination of the use of equipment that allows the monitoring of performance and the experience of the trainer who, with the use of this equipment, reclassifies his audience and reorients the training. Based on this, during the process of applying these instruments, we can see an improvement of up to 17% in the performance of motor-deficient athletes (wheelchair users) and up to 31% for children with intellectual disabilities, which allows us to consider that they are positive results.
The difficulties of developing these applications are focused on the construction of applications using IoT, especially in the integration of information, since different platforms are communicating with one another, such as the virtual instrumentation software (LabVIEW), smartphone, google fusion tables, among others. Besides, it also requires a correct application of the equipment and the adaptations on the protocols for each group.
Thus, future work in this area is to integrate other devices on the IoT technology, such as instrumented insoles, vertical jump platforms, and electromyographic signal acquisition systems, evaluate new audiences, and cross the information and conditions for each separated group.
Acknowledgments
The authors would like to thank the UTFPR for the scholarship during the time of this research.
Author Contributions
Caroline Peixoto Santos and Leticia Eloy Smaniotto conceived the tests; Caroline Peixoto Santos and Lucas Vacilotto Bonfati developed the devices and wrote this paper; José Jair Alves Mender Jr. wrote this paper; Leandro Martinez Vargas helped with the theory about sports science and evaluation; Sergio Luiz Stevan Jr. managed the research and wrote the paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen JJ, Chung YF, Chang CP, et al. (2014) A wearable virtual coach for marathon beginners. 20th IEEE International Conference on Parallel and Distributed Systems (ICPADS), Taiwan.
- Siewiorek DP (2012) Invited talk: Virtual coaches in health care. International Conference on Dependable Systems and Networks Workshops, USA.
- Amato A, Coronato A (2017) An IoT-Aware architecture for smart healthcare coaching systems. IEEE 31st International Conference on Advanced Information Networking and Applications, Taiwan.
- Gil D, Ferrández A, Mora-Mora H, et al. (2016) Internet of things: A review of surveys based on context aware intelligent services. Sensors (Basel) 16.
- Marin J, Blanco T, Marin JJ (2017) Octopus: A design methodology for motion capture wearables. Sensors (Basel) 17: 1875.
- JJA Mendes Jr, Vieira MEM, Pires MB, et al. (2016). Sensor fusion and smart sensor in sports and biomedical applications. Sensors 16: 1569.
- James DA, Petrone N (2016) Sensors and wearable technologies in Sport: Technologies, trends and approaches for implementation. SpringerBriefs in Applied Sciences and Technology.
- Ikram MA, Alshehri MD, Hussain FK (2015) Architecture of an IoT-based System for football supervision. IEEE 2nd World Forum on Internet of Things (WF-IoT), Italy.
- Gruetzemacher R, Gupta A, Wilkerson GB (2016) Sports injury prevention screen (SIPS): Design and architecture of an internet of things (IoT) based analytics heatlh app. AIS CONF-IRM 2016.
- Senanayake SMNA, Naim AG (2019) Smart sensing and biofeedback for vertical jump in sports. Modern Sensing Technologies.
- Wang Y, Chen M, Wang X, et al. (2018) IoT for next-generation racket sports training. IEEE Internet of Things Journal.
- Kobeissi AH, Chible H, Berta R, et al. (2017) Design and implemenration of an IoT system for enhancing proprioception training. 29th International Conference on Microelectronics (ICM), Lebanon.
- Harald G, Melanie H, Stella K, et al. (2014) E-coaching: Conceptual and empirical findings of a virtual coaching programme. International Journal of Evidence Based Coaching and Mentoring 12: 165.
- Ling R (2004) The Mobile Connection: The Cell Phone's Impact on Society, San Francisco, Elsevier.
- Watson A, Bickmore T, Cange A, et al. (2012) An internet-based virtual coach to promote physical activity adherence in overweight adults: Randomized controlled trial. J Med Internet Res 14: e1.
- Baddeley AD, Kopelman MD, Wilson BA (2002) The Handbook of Memory Disorders. (2nd edn), West Sussex, John Wiley & Sons.
- Schalock RL, Duffy SAB, Bradley VJ, et al. (2010). Intellectual disability: Definition, classification, and systems of supports. (11th edn), Washington.
- (2010) Demographic Census 2010: General characteristics of the population, religion and people with disabilities. Brazilian Institute of Geography and Statistics, Brazil.
- American Psychiatric Association, DSM-5 Task Force (2013) Diagnostic and statistical manual of mental disorders (DSM-5®). American Psychiatric Publishing.
- Scarpato M (2007) Educação física: Como planejar as aulas na educação básica. Avercamp, São Paulo.
- Nunes RL, Godoy JRP, de Barros JF (2003) Efeitos de um programa de exercícios resistidos em indivíduos adultos portadores de deficiência mental. Educacion Fisica y Deportes 64: 1-25.
- Wright BA (1983) Physical disability-a psychosocial approach. (2nd edn), Haper Collins Publishers, USA.
- Thomson RG (2017) Extraordinary bodies: Figuring physical disability in american culture and literature. Columbia University Press, New York.
- Hasan OA, Rashid AT, Ali RS, et al. (2017) A practical performance analysis of low-cost sensors for indoor localization of multi-node systems. 2017 Internet Technologies and Applications, UK.
- Zagatto AM, Beck WR, Gobatto AC (2009) Validity of the running anaerobic sprint test for assessing anaerobic power and predicting short-distance performances. J Strength Cond Res 23: 1820-1827.
- Moharana SR, Jha VK, Satpathy A, et al. (2017) Secure key-distribution in IoT cloud networks. 2017 Third International Conference on Sensing, Signal Processing and Security, India.
- Ray PP (2015) Internet of things for sports (IoTSport): An architectural framework for sports and recreational activity. 2015 International Conference on Electrical, Electronics, Signals, Communication and Optimization, India.
- Gope P, Hwang T (2015) BSN-care: A secure IoT-based modern healthcare system using body sensor network. IEEE Sensors Journal 16: 1368-1376.
Corresponding Author
Sergio Luiz Stevan Jr, Graduate Program in Electrical Engineering (PPGEE), Department of Electronic Engineering, Federal Technological University of Parana (UTFPR), Ponta Grossa (PR) 84016-210, Brazil, Tel: +55-42-3220-4825.
Copyright
© 2018 Bonfati LV, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.