Grip Strength and Carpal Tunnel: What Interest in Management
Abstract
Introduction: Carpal tunnel syndrome (CTS) is one of the most common musculoskeletal disorders of the upper extremity. Initial treatment, indicated in sensitive forms, is generally nonoperative, with the strongest evidence supporting bracing/splinting. Strong evidence supports operative treatment, in motor forms, regardless of technique, as superior to nonoperative treatment. Severity of motor forms of CTS depend of clinicals (MRC score, amyotrophy) and Electroneuromyography aspects (motor latency, potential amplitudes and reduced trans-carpal motor velocities. In those forms, therapeutics decisions are difficults according to electroneuromyography aspects and clinicals symptoms come late. Some authors retained that an abnormal ENMG is an indication of surgical treatment. In others, surgical treatment depends of distal motor latency (MDL). Hook grip strength; which need contraction of superficial flexor carpi digitis and thenar eminency muscles could early diagnosed decrease strength, severity of CTS, and contributed of therapeutic decision.
Objectives : Our study aim to determine strength grip characteristics in diffents class of severity in CTS.
Patients and methods: We conducted a multicenter study including patients with unilateral CTS, followed at the laboratory of Neurophysiology, Fann teaching Hospital, Orthopediae Department of Malt, Dakar Senegal and Physical Medicine Fann teaching Hospital. Study was conducted on two phases. Were not included, patients with bilateral CTS and those with pre-existing functional limitations of upper limb. We classed patients in 3 groups of severity according to motor ENMG parameters. Hook grip strength measured in all patients by a dynamometer with a maximum strength of 90 kg on both sides and Functional capacity evaluated by Functional dimension of Boston Crapal Tunel Questionary (FBCTQ). We classes strength grip on three groups of severity according to differences of both sides.
Results: We collected 33 patients. Median age was 48.33 ± 11.67 years. Sex-ratio was 0.27. Dominant side interested in 72.7% of patients. Clinical symptoms of CTS dominated by numbness (66.7%). CTS was severe in 54. 5% of patients and idiopathic (75.8%). Grip strength decreased in 81.8% of patients. Minor reduced grip strength interested 45.5% of patients. FBCTQ score is less than 2/5 in 64% of patients. Most difficult activity of patients with CTS was open a covercle (score of FBCTQ: 2.52). Functional prognosis factor in CTS were FBCTQ (P = 0.035), trans-carpal Tunel Velocity (p = 0.025).
Conclusion: Therapeutics decisions in CTS must included evaluation of Hook Grip strength. In some part which Hook Grip strength can’t be evaluated, patients need an evaluation of FBCTQ or trans-carpal tunnel velocity.
Keywords
Tunnel, Carpal, Syndrome, Strength grip, Dynamometer
Introduction
Carpal tunnel syndrome (CTS) is one of the most common musculoskeletal disorders of the upper extremity [1]. CTS represented 90% of all neuropathy [2]. Annual incidence estimated at 3.8 per 1000 in general population, 1 to 2/1000 in men, 4 to 5/1000 in women [3]. It is most often linked for compression of median nerve at the wrist [4]. Idiopathic CTS is most frequent [5]. Clinicaly, syndrome characterized by hand pain, numbness and tingling in median nerve distribution. Classically, Carpal tunnel syndrome is first sensory, then sensorimotor. Motor assessment of CTS can be done using MRC scale or a dynamometer, which measures grip strength. Studies suggest that subjects with CTS lose grip strength, and Higher severity levels of CTS result in greater reduction in grip strength [6]. Initial treatment, indicated in sensitive forms, is generally nonoperative, with the strongest evidence supporting bracing/splinting. Strong evidence supports operative treatment, in motor forms, regardless of technique, as superior to nonoperative treatment. Severity of motor forms of CTS depend of clinicals (MRC score, amyotrophy) and ENMG aspects (motor latency, potential amplitudes and reduced trans-carpal motor velocities). In those forms, therapeutics decisions are difficult according to ENMG aspects and clinics symptoms come late. Somes authors retained that an anormal ENMG is an indication of surgical treatment [7,8]. In others, surgical treatment depends of distal motor latency (MDL). Our hypothesis is, decrease hook grip strength could diagnosed severity of CTS and contributed of therapeutics decisions.
Objectives
Our study aim to determine strength grip characteristics in diffents class of severity in CTS.
Patients and Methods
We conducted a transversal, descriptive and analytic study at two phases (15 th August-15 th november 2022; 01 January - 3 August 23; at the Departments of Neurophysiology and Physical Medicine, Fann teaching hospital, Malt Orthopedia Department, Dakar, Senegal. Study included patients followed at those centers, for treatment of unilateral CTS. Diagnosis of CTS were clinical and or ENMG. Clinicals symptoms retained were Pain and paresthesia in three first fingers, associated of tinel and or Phalen signs. ENMG aspects were reduced trans-carpal velocity more than 10 m/second, in comparison of velocity at forearm and high motor distal latency in median nerve (superior of 4 ms). Patients with bilateral CTS and those with pre-existing functional limitations of upper limb were excluded. We establish a questionary for noted sociodemographics aspects, clinical and results of ENMG aspects. We class patients in 3 groups of severity according to trans-carpal tunnel velocity (Table 1). We used Functional domains of Boston Carpal Tunel Questionary (FBCTQ) for evaluation of functional limitations of CTS. This questionnaire evaluated 8 domains of activities of hand. Domains of BCTQ are write (Wr), buttoning clothes (BC), taking a book (TB), taking a telephone (TT), cleaning (Cl), opening a bottle lid (OBL), taking shopping bags (TSB), washing (Wa) and dressing (Dr). Patients who cannot write or do not use affected side to write are evaluated on the remaining items. Items are answered on a 5-point scale ranging from 1 (no difficulty) to 5 (cannot perform activity at all). A single score is calculated as the average of the FCTQ in 69 by adding scores of different items of questionary divided by 8 (or 7 in patients who cannot write). The averages were represented by classes: [1; 2]/[2;3]/[3;5]. Assessment of pain was done by Neuropathic Pain Scale. Hook grip strength was measured in all patients by a dynamometer with a maximum strength of 90 kg (Figure 1), twice in pathologic side, one in normal side. Our choice for evaluation of hook grip strength supported by necessary contraction of superficial flexor carpi digitis and muscles of thenar eminency, innerved by median nerve. We retained best strength on pathologic side. Grip strength of pathologic side, compared to normal side and we retained difference of strength and classed patients in three groups of severity (Table 2). Data collection and analysis were carried out with strict respect of identity and informed consent.
Data Analysis
We used Excel database to perform data entry. Statistical analysis was carried out using statistical software SPSS version 20.0. A quantitative analysis is carried out based on averages and frequencies. The qualitative analysis made it possible to correlate grip strength with degrees of clinical severity, electroneuromyographic, types of treatment and the FBCTQ. Significance threshold was set at 0.05.
Results
Sociodemographic aspects
Thirty three (33) patients included in our study with an average age of 48.33 ± 11.67 years. Sex-ratio was 0.27. Classes of 40-60 years were largely predominant (62%). Patients aged more than 60 years represented 9% and those less than 40 years 29%. Married patients represented 85%. Women domestic activities (26.2%) and sellers activities (36.4%) were most represented. Dominant side was right in 84.8% of patients.
Clinics and ENMG aspects
Numbness (66.7%), electric shocks pain (51.5%) and burning pain (30.3%) were predominant symptoms. Intensity juged minimal in 31.3% and moderate (53.1%). Mechanism of pain was neuropathic in 51.5% of cases. Symptoms worse at night in 84.4% of patients. Others symptoms of CTS found were paresthesia (21.3%), Tinel (67%), Phalen (33%), hypoesthesia of median territory (48.5%) and thenar amyotrophy (18.2%). Trans-carpal tunnel velocity reduced in 54.5% of patients. Reduced velocity Trans-carpal Tunnel was minimal (24.2%), moderate (12.2%) and severe (54.5%). CTS was idiopathic in 75.8%, traumatic (9.1%). It’s occured in pregnancy (9.1% and Renal failure (3%). Operator treatment curried in 9.1% of patients. Conservator treatment used pregabaline (66.3%), local corticosteroids (24.2%), physical rehabilitation (27.3%), association paracetamol + opioides (69%).
Functional abilities
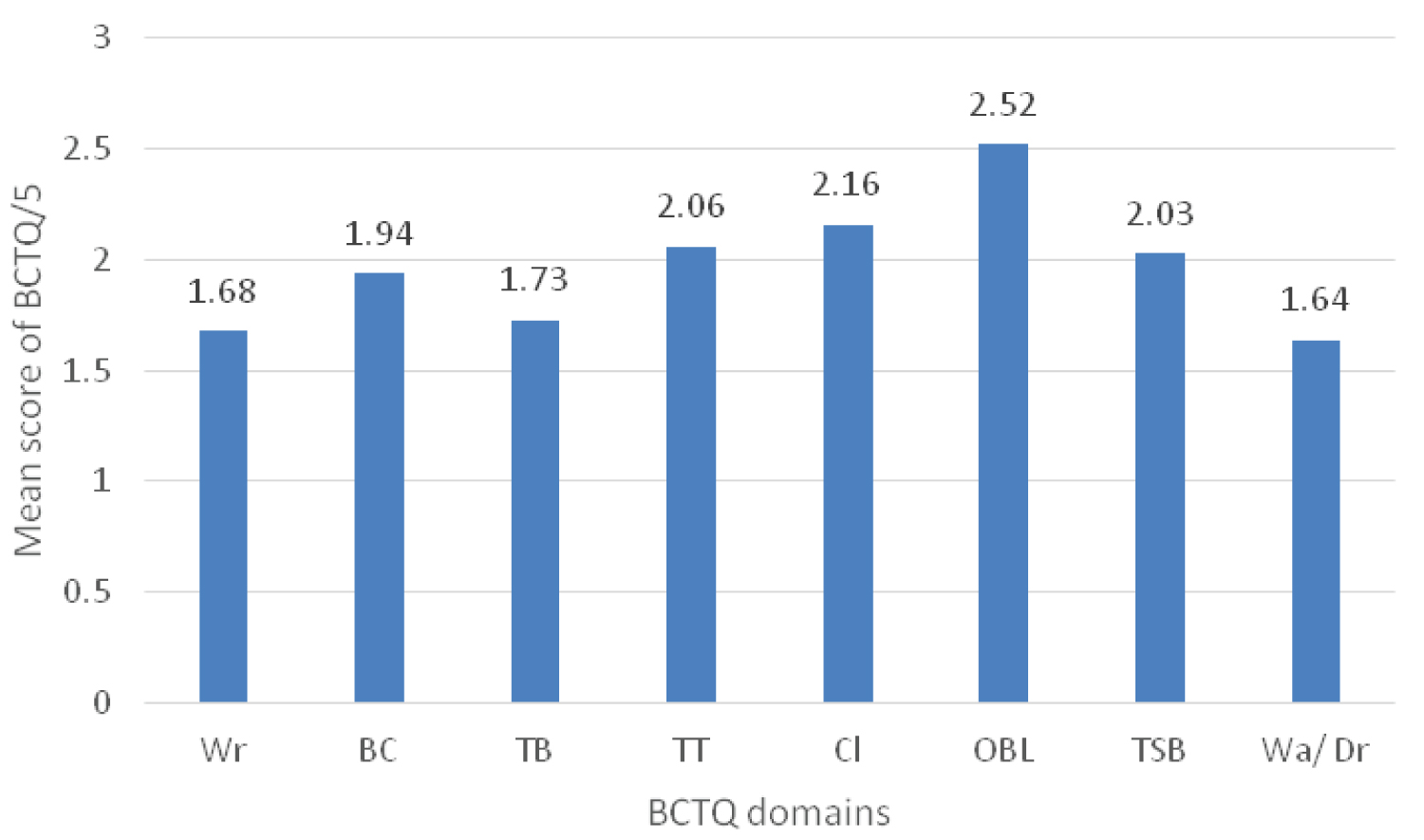
Strength grip reduced in 81.8% of patients with CTS. Reduced strength was minimal (45.5%), moderate (24.2%), severe (12.1%). According to FBCTQ, limitations were minimal, score (1-2) in 64%. Moderate limitations represented by score 2-3 noted in 24% of patients and severe limitations in 12%. Overage score of FBCTQ was 2/5. Most difficult activity for patients with CTS was open a covercle (score BCTQ: 2.52) (Figure 2). Correlations between strenght grip and clinicals, ENMG and functional abilities noted in Table 3.
Discussion
CTS is the most common peripheral nerve entrapment syndrome. In our study, CTS is more frequent in adult aged 40-60years and women. All most of study suggests that CTS occurs more commonly in women, with an annual incidence of 1.5 per 1000 compared to 0.5 per 1000 for men [9]. Variability of incidence with gender, can be explained by hormonal factors as pregnant and breast feeding women have increased risk of CTS [10]. In our study, in accordance with literature, CTS localized in dominant side in 84.8% and noted, in patients with occupational and manual activities [11]. Most frequent professional activities found in our study were domestic activity (26.2%) and sellers activity (36.4%). Married women, in Senegal, generally, with low level education, have rarely an renumered profession, and take care home activities like dressing, cleaning, cooking, laundry. Those activities constituted risk factors of CTS. Others risk factors found in our study were pregnancy, renal failure and traumatism. In 1992, Hagberg, et al. published a review of 21 studies including high quality information on occupational associations, and reported an increased risk of CTS in a number of jobs believed to involve repetitive and forceful gripping [12]. The typical presentation of CTS involves pain and/or dysaesthesia of the fingers (typically the radial 3½ digits but can be diffuse throughout the hand and can radiate proximal to the wrist). Symptoms are often worse at night or in the early morning. Examination in advanced cases may reveal wasting of the thenar eminence and/or weakness of thumb abduction. Provocation tests such as those of Tinel (tapping the flexor retinaculum) and Phalen (full passive flexion of the wrist for 1 minute) are widely used as confirmatory tests in clinical practice. However, the sensitivity and specificity of these tests seem to be much greater in patients with more advanced disease [11]. Place of ENMG in CTS is unclear. Some authors noted that in typical CTS, ENMG is unnecessary. ENMG can contribute for therapeutics decisions. In Department of Neurophysiology, Fann teaching hospital, we determine in all patients with suspicion of CTS, motor trans-carpal Tunnel velocity after stimulation in palm, wrist et elbow. Sensory trans-carpal tunnel velocity determined with classical methods. Reduced of trans-carpal tunnel velocity in the palm confirm CTS and represented an early symptoms of alteration of motor fibers. For therapeutic decisions, we referred to distal motor latency of median nerve and existing of denervation in detection. Our patients benificed for therapeutics used CTS [13] but we noted a few part of surgery which can be explain by socio-cultural consideration of surgery and financial statut of our patients. Senegalese patients are fear for surgery. In our study, average FBCTQ was approximately 2/5. This result is lower than Kang et al who obtain a average score of 2.8 before surgery. After surgery, they score decreasy (1.7) [14]. However, our score remains higher than Ndedi, et al. [15] and Alvin, et al. [16] studies, which found averages of 1.50 and 1.20 respectively. Strength grip reduced in 81.8% of patients with CTS. An study, which measuring the time course of three first finger's grip motion shown, in CTS group, grip time with the index, middle, and ring fingers was longer, and time which strength was lost after reaching the maximum was earlier [17 ]. Correlation between strength grip and severity CTS is variable in literature. A study using a conventional grip dynamometer noted no correlation [18]. Authors explain their results for an synergistic function of the intrinsic and extrinsic muscles of the hand at grip motion, so patients does not use the muscles affected by CTS [19]. Toru Sasaki, et al. found a correlation between strength grip of the ring and little finger and subjective symptoms of CTS and functional abilities [17]. Patients with severe subjective symptoms tended to not use the index and middle fingers during grip motion. In our study, a correlation found between grip strength and trans-carpal tunnel velocity and FBCTQ.
Conclusion
CTS most affected adults women with manual activities, and symptoms are initially subjective, affected three first fingers, more frequent at night. Severity appreciated clinically, ENMG aspects, Functional limitaions. Measurement of Strength grip, which decrease at time in CTS, can diagnosis early alteration of motor fibers of median nerve in CTS and help for therapeutics decisions.
References
- Calandruccio JH, Thompson NB (2018) Carpal tunnel syndrome: Making evidence-based treatment decisions. Orthop Clin North Am 49: 223-229.
- Aboonq MS (2015) Pathophysiology of carpal tunnel syndrome. Neurosciences (Riyadh) 20: 4-9.
- Petrover D, Richette P (2018) Prise en charge du syndrome du canal carpien: de l’échographie diagnostique à la libération percutanée sous échographie. Rev Rhum 85: 243-250.
- Pommerol P, Travers V (2014) Thérapie manuelle du canal carpien avant chirurgie. KS n°553 - avril.
- Genova A, Dix O, Saefan A, et al. (2020) Carpal tunnel syndrome: A review of literature. Cureus 12: e7333.
- Singh GK, Srivastava S (2020) Grip strength of occupational workers in relation to carpal tunnel syndrome and individual factors. Int J Occup Saf Ergon 26: 296-302.
- RAND Center for Health and Safety in the Workplace (2011) RAND/UCLA quality-of-care measures for carpal tunnel syndrome. Pittsburgh: RAND Corporation.
- Maggard MA, Harness NG, Chang WT, et al. (2010) Indications for performing carpal tunnel surgery: Clinical quality measures. Plast Reconstr Surg 126: 169-179.
- Stevens JC, Sun S, Beard CM, O'Fallon WM, Kurland LT (1988) Carpal tunnel syndrome in Rochester, Minnesota, 1961 to 1980. Neurology 38: 134-138.
- Nordstrom DL, Vierkant RA, DeStefano F, et al. (1997) Risk factors for carpal tunnel syndrome in a general population. Occup Environ Med 54: 734-740.
- Newington L, Clare Harris E, Walker-Bone K (2015) Carpal tunnel syndrome and work. Best Pract Res Clin Rheumatol 29: 440-453.
- Hagberg M, Morgenstern H, Kelsh M (1992) Impact of occupations and job tasks on the prevalence of carpal tunnel syndrome. Scand J Work Environ Health 18: 337-345.
- Seye M (2022) Intérêt de l’étude de la force de préhension dans le syndrome du canal carpien: étude préliminaire à propos de 20 cas. [thesis], UCAD, N 351.
- Kang HJ, Koh IH, Lee TJ, et al. (2013) Endoscopic carpal tunnel release is preferred over mini-open despite similar outcome: A randomized trial. Clin Orthop Relat Res 471: 1548-1554.
- Ndedi Penda X. Résultats obtenus aprés libération endoscopique du canal carpien: à propos de 23 cas. 2019. Disponible Sur.
- Chao-Yu Chen A, Wu M-H, et al. (2011) Single portal endoscopic carpal tunnel release: Modification of Menon’s technique and data from 65 cases. Int Orthop 35: 61-65.
- Sasaki T, Makino K, Nimura A, et al. (2020) Assessment of grip-motion characteristics in carpal tunnel syndrome patients using a novel finger grip dynamometer system. J Orthop Surg Res 15: 245.
- Atalay NS, Sarsan A, Akkaya N, et al. (2011) The impact of disease severity in carpal tunnel syndrome on grip strength, pinch strength, fine motor skill and depression. J Phys Ther Sci 23: 115-118.
- Geere J, Chester R, Kale S, et al. (2007) Power grip, pinch grip, manual muscle testing or thenar atrophy - which should be assessed as a motor outcome after carpal tunnel decompression? A systematic review. BMC Musculoskelet Disord 8: 114.
Corresponding Author
Diagne Ngor Side, Physical Medicine and Rehabilitation Department, Fann Teaching Hospital, Dakar, Senegal.
Copyright
© 2024 Diagne NS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.