Bicortical Screw Fixation into an Intramedullary Nail in Peri-Implant Femoral Fractures
Abstract
Peri-implant femoral fractures following trochanteric fixation with a cephalomedullary nail are becoming increasingly common in elderly patients. These fractures require operative treatment to achieve fracture healing and restore alignment. Conventional augmentation methods-such as unicortical screws, cerclage wiring, cable wiring, and locking-attachment plates-provide stability but only partial cortical purchase because the intramedullary nail occupies the femoral canal, which may limit construct strength.
We describe a bicortical screw fixation technique in which a screw is inserted from an extramedullary plate through the interlocking hole of the intramedullary nail, thereby integrating the proximal bone fragment, the nail, and the plate into a single construct.
Introduction
A peri-implant fracture is defined as a fracture occurring in bone that already contains an implant [1], such as an extramedullary plate or an intramedullary nail. Cephalomedullary nailing is the standard treatment for trochanteric femoral fractures in elderly patients, but peri-implant fractures after such fixation are increasingly encountered due to underlying osteoporosis [2].
These fractures require operative management to restore mobility, allow patients to care for themselves, prevent complications of immobility, and ensure fracture healing without deformity or disability. The choice of surgical technique depends on the healing status of the original fracture [3]. In elderly patients with cephalomedullary nails, fracture healing may be difficult to assess, and implant removal may risk creating a new fracture [4]. For this reason, surgeons often retain the original nail and augment fixation with an extramedullary plate.
Traditional methods for connecting the plate to the proximal fragment [5]-unicortical screws, cerclage wiring, cable wiring, and locking-attachment plates-can provide stability but achieve only partial cortical purchase because the nail blocks bicortical screw placement. This limitation motivates the bicortical screw fixation technique, in which a screw is inserted through a plate hole aligned with the interlocking hole of the cephalomedullary nail, creating a unified plate-nail-bone construct.
Surgical Technique
Material and methods
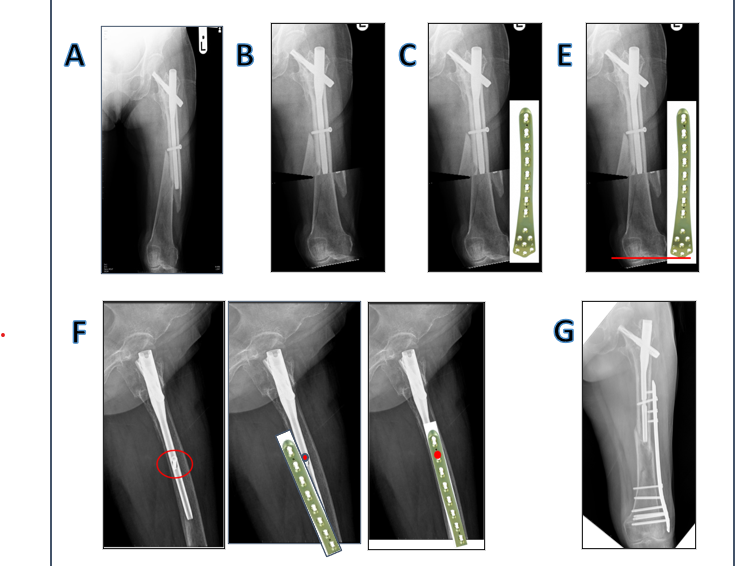
The patient is positioned supine on a fracture table with the contralateral leg placed in hemilithotomy. Indirect reduction is achieved with table traction, followed by fluoroscopic confirmation of leg length and alignment. Once satisfactory, the operative field is prepared and draped in a sterile fashion.
A minimally invasive plate osteosynthesis (MIPO) approach is performed. Small incisions are made at the proximal and distal fragments, and a submuscular tunnel is developed along the lateral femur. The original interlocking screw of the cephalomedullary nail is identified and removed.
An appropriately sized extramedullary plate is selected using fluoroscopic measurement and inserted through the MIPO tunnel. The distal end of the plate is positioned and temporarily secured with a Kirschner wire placed through a combi-hole.
The interlocking hole of the intramedullary nail is then identified. By sliding the plate slightly proximally or distally, a conventional plate hole is aligned with the nail’s interlocking hole. A screw is inserted through the plate and into the interlocking hole to achieve bicortical fixation.
Additional screws are placed into the distal fragment. Because the nail prevents proximal bicortical purchase, supplementary proximal fixation is added using one of the following: unicortical screws, cerclage wiring, cable wiring, or a locking-attachment plate. Final fluoroscopic assessment confirms alignment and implant placement. The wounds are closed in layers (See Figure 1).
Results
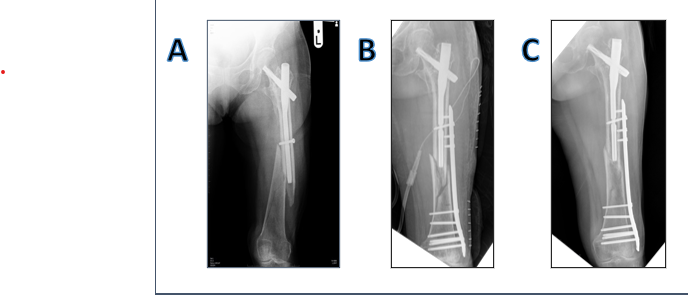
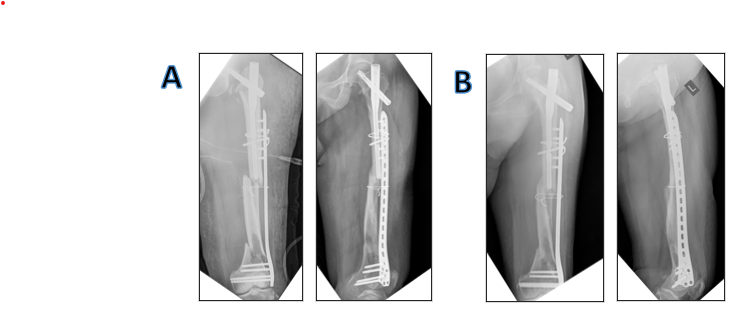
Postoperative radiographs should demonstrate improved alignment compared with preoperative imaging (See Figure 2 and Figure 3).
Pearls and Pitfalls
Pearls
- Indirect reduction using the fracture table must be completed before beginning the operation
- Plate length should be selected using fluoroscopic measurement
- Correct distal plate positioning must be confirmed, and temporary fixation with a K-wire helps maintain alignment.
- Because a single bicortical screw into the nail is insufficient for full construct stability, an additional method of proximal fixation is required
Pitfalls
- The bicortical screw should be 2 mm longer than the original interlocking screw to account for plate thickness
- The cephalomedullary nail, extramedullary plate, and interlocking screw should be of the same material to avoid galvanic corrosion
Advantages and Disadvantages
Advantages
- A conventional bicortical interlocking screw is less expensive than other augmentation techniques such as unicortical screws, cable wiring, or locking-attachment plates.
- Bicortical fixation provides greater stability than unicortical screws, cerclage wiring, cable wiring, or locking-attachment plates.
Disadvantages
- In some cases, the interlocking screw may sink into the surrounding bone, making insertion more difficult
Discussion
Bicortical screw fixation into an intramedullary nail provides improved stability to the extramedullary plate and may help prevent displacement of the fixation construct in peri-implant femoral fractures.
Several methods are available to connect the plate to the proximal bone segment:
• Unicortical screws engage only the near cortex and do not connect directly to the implant.
• Cerclage or cable wiring wraps around the bone but offers limited vertical stability and no direct implant connection.
• Locking-attachment plates allow multiple screw directions around the nail but have higher implant costs and still lack direct connection to the original implant.
The bicortical screw technique described in the PDF is relatively inexpensive, provides strong fixation, and integrates the proximal bone fragment, intramedullary nail, and extramedullary plate into a single system.
- There’s no any funding or research grants received in the course of study, research or assembly of the manuscript
- There's no financial/personal interest or belief that could affect their objectivity, or if there is, stating the source and nature of that potential conflict.
References
- Lester Chan WM, Antony Gardner W, Merng Koon Wong, et al. (2018) Non-prosthetic peri-implant fractures: Classification, management and outcomes Arch Orthop Trauma Surg 138: 791-802.
- Norris R, Bhattacharjee D, Parker M (2012) Occurrence of secondary fracture around intramedullary nails used for trochanteric hip fractures: A systematic review of 13,568 patients. Injury 43: 706-711.
- Yli Kyyny T, Sund R, Juntunen M, et al. (2012) Extra and intramedullary implants for the treatment of pertrochanteric fractures-results from a Finnish National Database Study of 14,915 patients. Injury 43: 2156-2160.
- Müller F, Galler M, Zellner M, et al. (2016) Peri-implant femoral fractures: The risk is more than three times higher within PFN compared with DHS. Injury 47: 2189-2194.
- Dunn J, Kusnezov N, Bader J, et al. (2016) Long versus short cephalomedullary nail for trochanteric femur fractures (OTA 31-A1, A2 and A3): A systematic review. J Orthop Traumatol 17: 361-367.
Corresponding Author
Chavalit Iemsaengchairat, MD, Department of Orthopedics, Nakhon Pathom Hospital, Nakhon Pathom, Thailand.
Copyright
© 2026 Iemsaengchairat C, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.