The Hyper Wag Fluoroscopic View for Cephallomedullary Screw Placement in Hip Fracture Treatment
Keywords
Cephalomedullary nail, Articular penetration, Hip fracture, Intraoperative fluoroscopy, Low calcar
Background
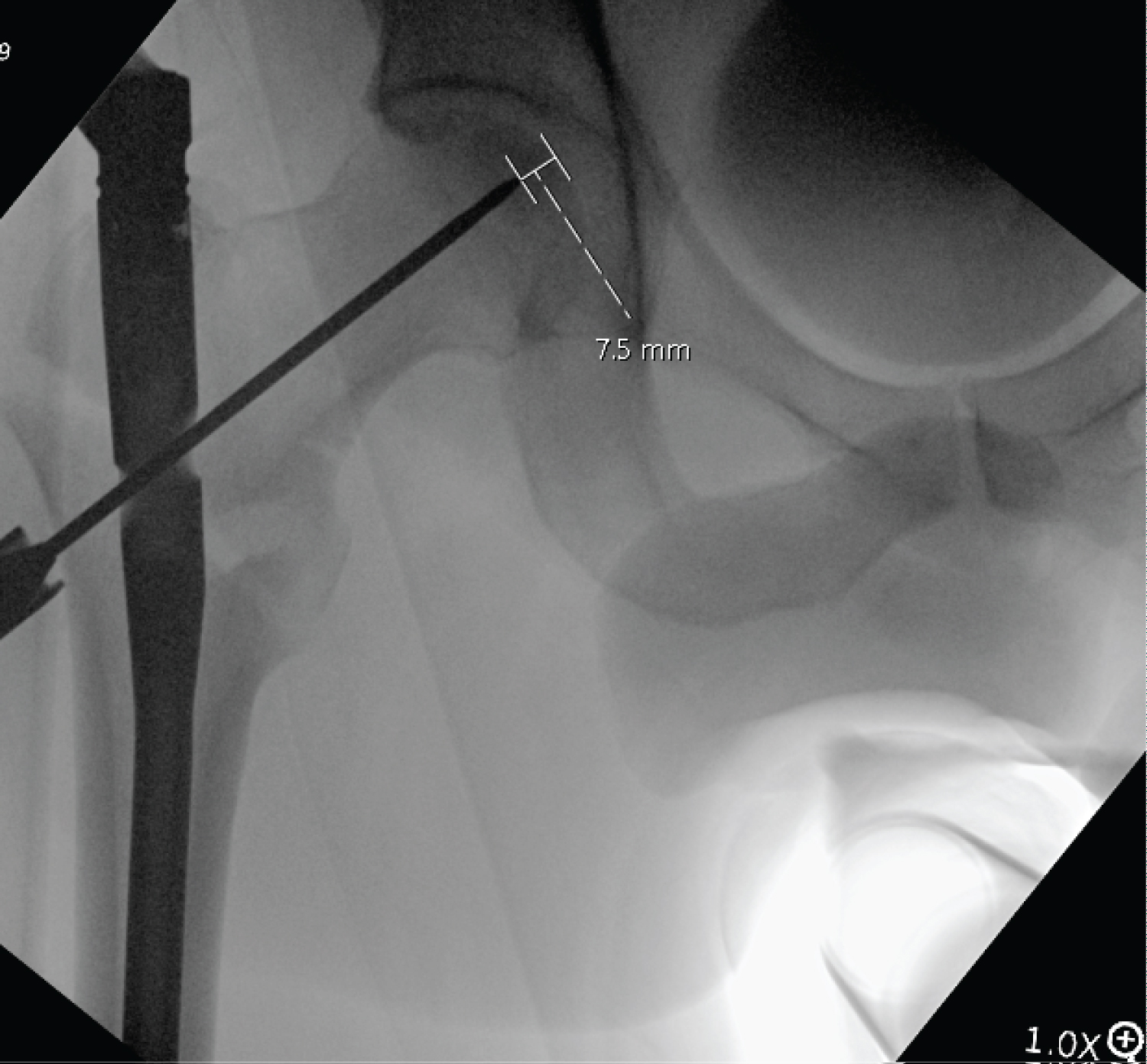
Intraoperative fluoroscopy is routinely used to guide appropriate guide wire placement and eventual lag screw placement during internal fixation of a proximal femoral fracture. The femoral head and neck are evaluated in at least two planes to avoid articular screw penetration but also ensure adequate lag screw purchase within the femoral head. The importance of this concept was originally highlighted by Baumgaertner describing the tip to apex distance, which is routinely evaluated on AP and lateral views [1]. The fluoroscopic C-arm is typically positioned contralateral to the operative extremity, traversing the field to the operative hip at a 45-degree angle relative to the axis of the patient. The source and image intensifier are centered at the hip for an AP view (Figure 1). The lateral view is traditionally "rain bowed' to 90 degrees to flat or adjusted for an appropriate lateral view of the proximal femur depending on the orientation of the bony anatomy (Figure 2a and Figure 2b). These two views have been described for evaluating the tip to apex distance of the helical blade or lag screw, with the goal of obtaining a measurement of less than 25 mm; as 25 mm or greater is accepted to be positively correlated with screw cutout. However, recent studies have directed a push towards more inferior positioning of the lag screw to a "low calcar" or inferior position. Veering from the traditional "center-center" screw position can render tip to apex distance somewhat unreliable. However, this position has been shown to create a biomechanically superior construct when analyzed using calcar referenced tip to apex distance (Figure 3), and we believe it provides additional calcar support, increasing stability and resistance to cutout. The resulting positioning technique is commonly referred to as the "hyper wag" view at our institution and has gained popularity due to its utility. It allows for multiplanar visualization of the spherical femoral head to prevent articular screw penetration [2]. The hyper wag view is especially useful when using the inferior screw position, as articular penetration through the inferior aspect of the femoral head is a risk due to its shape.
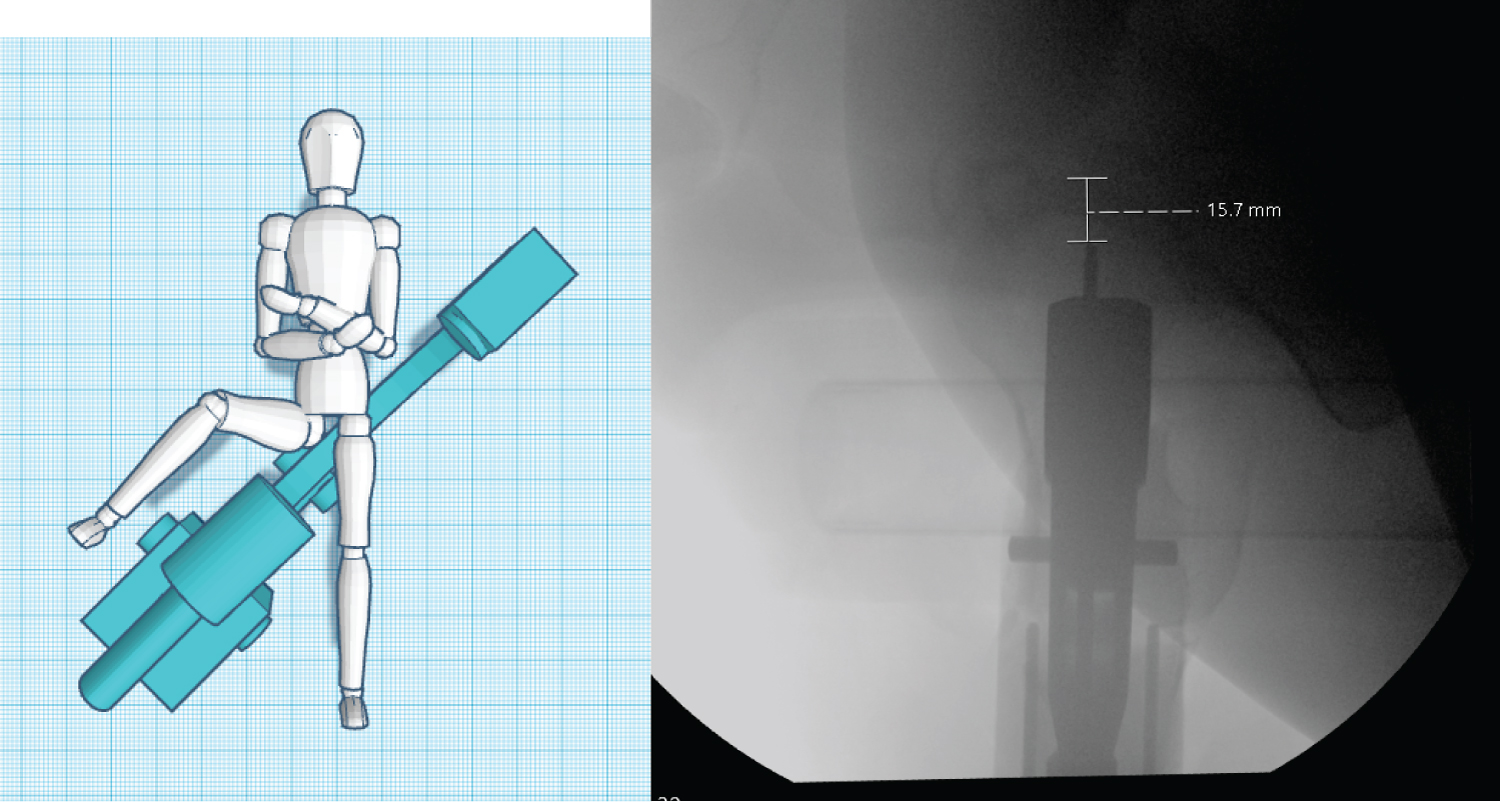
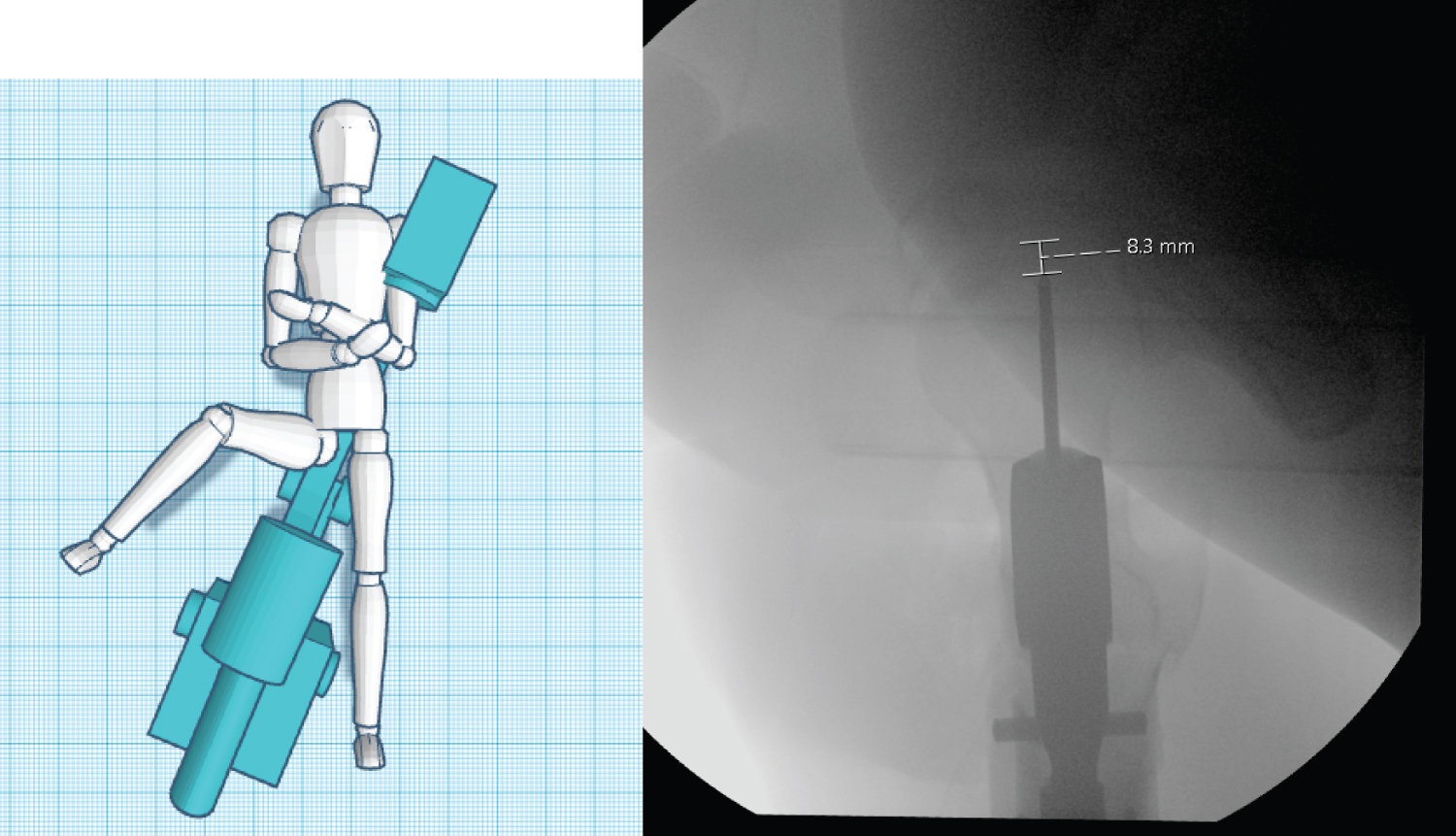
Since the leading edge of the guide wire is not central within the femoral head, hardware penetrating the inferior medial aspect of the femoral head may appear acceptable on traditional lateral imaging. An example of this is highlighted in the sample images, wherein, the traditional lateral image shows the tip of the threaded guide wire 15.7 mm from the articular surface. However, the hyper wag view reveals that this is misleading, as the guide wire is 8.3 mm from the cartilage from that point of view. In this instance, further advancement of the guide wire without utilizing orthogonal views of the proximal femur could lead to articular guide wire penetration.
Technique
To obtain the hyper wag view intraoperatively, the patient is positioned supine on a fracture table. The view is obtained by transitioning from the traditional lateral view. Unlock the C-arm and maneuver the beam source handle at approximately 20-30 degrees to the longitudinal axis of the patient, a "flatter" angle. In addition, we recommend utilizing the "rainbow" to obtain an AP image 15 degrees from flat, to account for the typical anteversion of the femoral neck. This will allow for excellent visualization of the femoral head and neck when performing guide pin positioning.
Conclusion
The hyper wag view has become a mainstay technique for intraoperative visualization of the lag screw of a cephalomedullary implant within the femoral head during the treatment of proximal femur fractures at our institution. It adds minimal additional radiation exposure and operative time with a properly oriented technician, while providing additional reassurance of optimal hardware placement. When implementing this technique into practice, utilization of common practice verbiage between the orthopedic surgeon and the X-ray technician facilitates communication, maintains operating room efficiency, and reduces radiation exposure to the patient and staff.
References
- Baumgaertner MR, Curtin SL, Lindskog DM, et al. (1995) The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am 77: 1058-1064.
- Kuzyk PR, Zdero R, Shah S, et al. (2012) Femoral head lag screw position for cephalomedullary nails: A biomechanical analysis. J Orthop Trauma 26: 414-421.
Corresponding Author
Matthew Weber, Riverside University Health System Medical Center, USA.
Copyright
© 2023 Weber M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.