Outcome of Limb Salvaging Procedure for Bone Tumor Using Liquid Nitrogen Technique: A Case Series of 21 Patients
Abstract
Introduction and importance: Autologous bone graft treated with liquid nitrogen is an option for biological reconstruction of bone defects in patients receiving tumor resection. This is the first report in Hong Kong on the outcome of this biological reconstruction in terms of functional outcome, local recurrence rate, and prognosis.
Case presentation: From 2015 to 2021, 21 patients with bone tumor resection and reconstruction using liquid nitrogen treated autologous bone graft were recruited. The medical records and radiological images were retrieved for retrospective review. After delivery of the specimen, all the soft tissue of the excised bone was removed at the back table before cryotherapy. The auto graft was immersed in liquid nitrogen for 20 minutes, and thawed at room temperature for 10 minutes.
After that the autograft was immersed in distilled water for 15 minutes before being incorporated into the reconstruction. All of them were followed up for at least one year post-operation.
Clinical discussion: The mean union time was 13.3 months (from 4 to 31 months). The mean Musculoskeletal Tumor Society (MSTS) score was 22.6 (from 12 to 30). The mean follow up time was 38.2 months (from 12 to 64 months). There were two local soft tissue recurrences and one local recurrence from host bone.
Conclusion: Autologous bone graft treated with liquid nitrogen is a safe option for biological reconstruction of bone defects after tumor resection. It provides satisfactory outcomes with low local recurrence rate, as well as comparable complications with other reconstruction methods.
Keywords
Frozen autograft recycling, Liquid nitrogen, Bone tumour, Biological reconstruction case series
Introduction
The goal of treatment for bone tumor is tumor resection with clear margins. In the past, limb sparing surgery was difficult especially in extensive tumor involvement, which was usually treated with amputation. With the advancement of technologies for better pre-operative planning, surgical instruments, operative techniques, and design of prosthesis, the outcome of limb sparing operation becomes more promising.
Patients with bone tumors undergoing wide local excision often result in extensive bone loss. Limb salvage operation with prosthetic reconstruction can be expensive, and may delay the surgery, especially by the custom-made implants design and manufacturing processes. Biological reconstruction requiring a large amount of bone graft is difficult while the availability of allograft is limited. Several autograft recycling techniques were developed such as autoclaving, irradiation, pasteurization and cryotherapy. Cryotherapy using liquid nitrogen has become more popular in view of multiple potential advantages, including simplicity, low infection rate, low recurrence rate, preservation of osteoinduction and osteoconduction, adequate biomechanical strength, no storage issue, preservation of cartilage, and cryo-immunological effect [1-3]. 21 patients underwent biological reconstruction with autologous bone graft treated with liquid nitrogen after wide local excision of bone tumors are reviewed in this series. The work has been reported in line with the SCARE 2020 guideline and PROCESS criteria [4,5].
Method
From 2015 to 2021, 21 patients with bone tumors underwent wide local excision of the tumors and reconstruction with autologous bone graft treated with liquid nitrogen. Their medical records and radiological images were retrieved for this retrospective review.
All the operations were performed by a team of sub specialized orthopedics oncology surgeons, led by a consultant with more than 20 years experience in orthopedic oncology in a university- affiliated tertiary referral center.
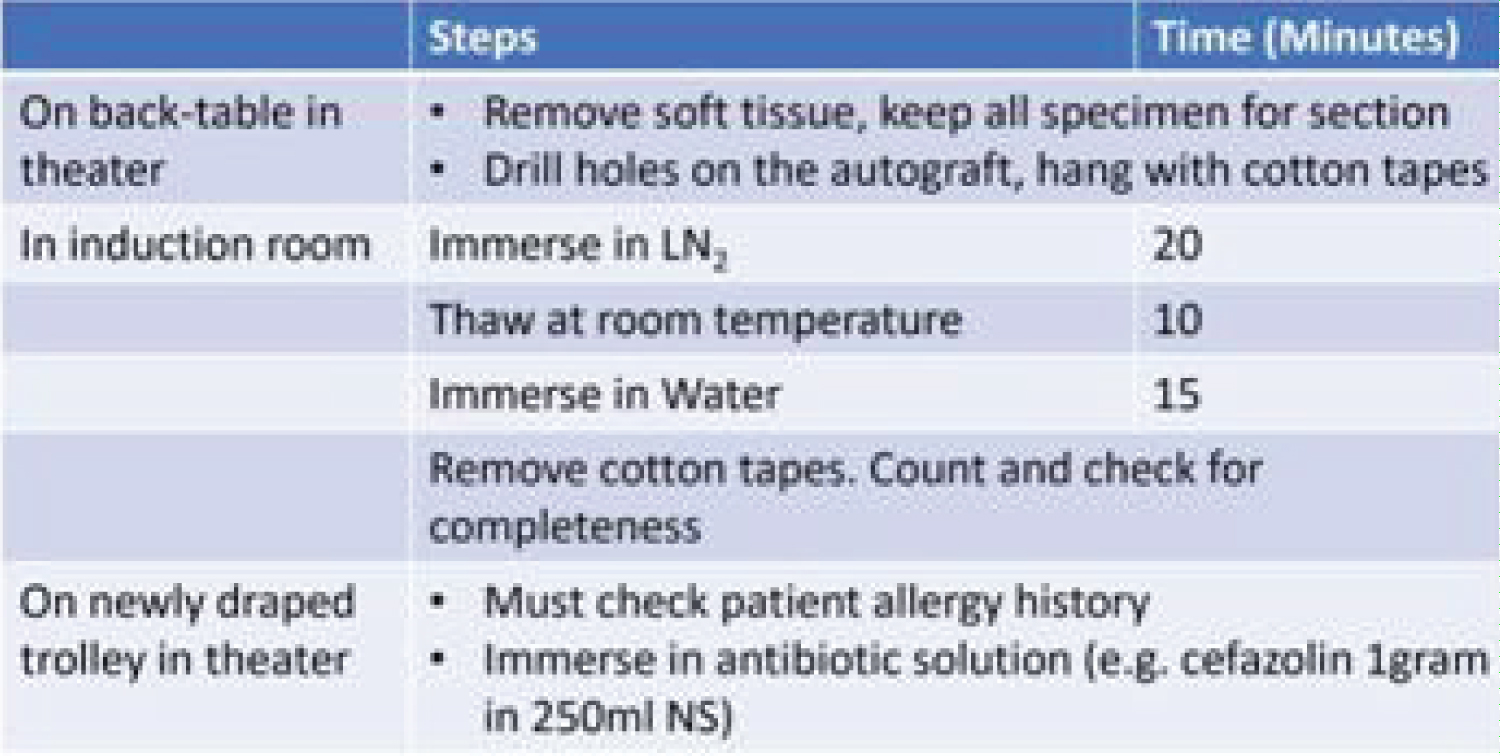
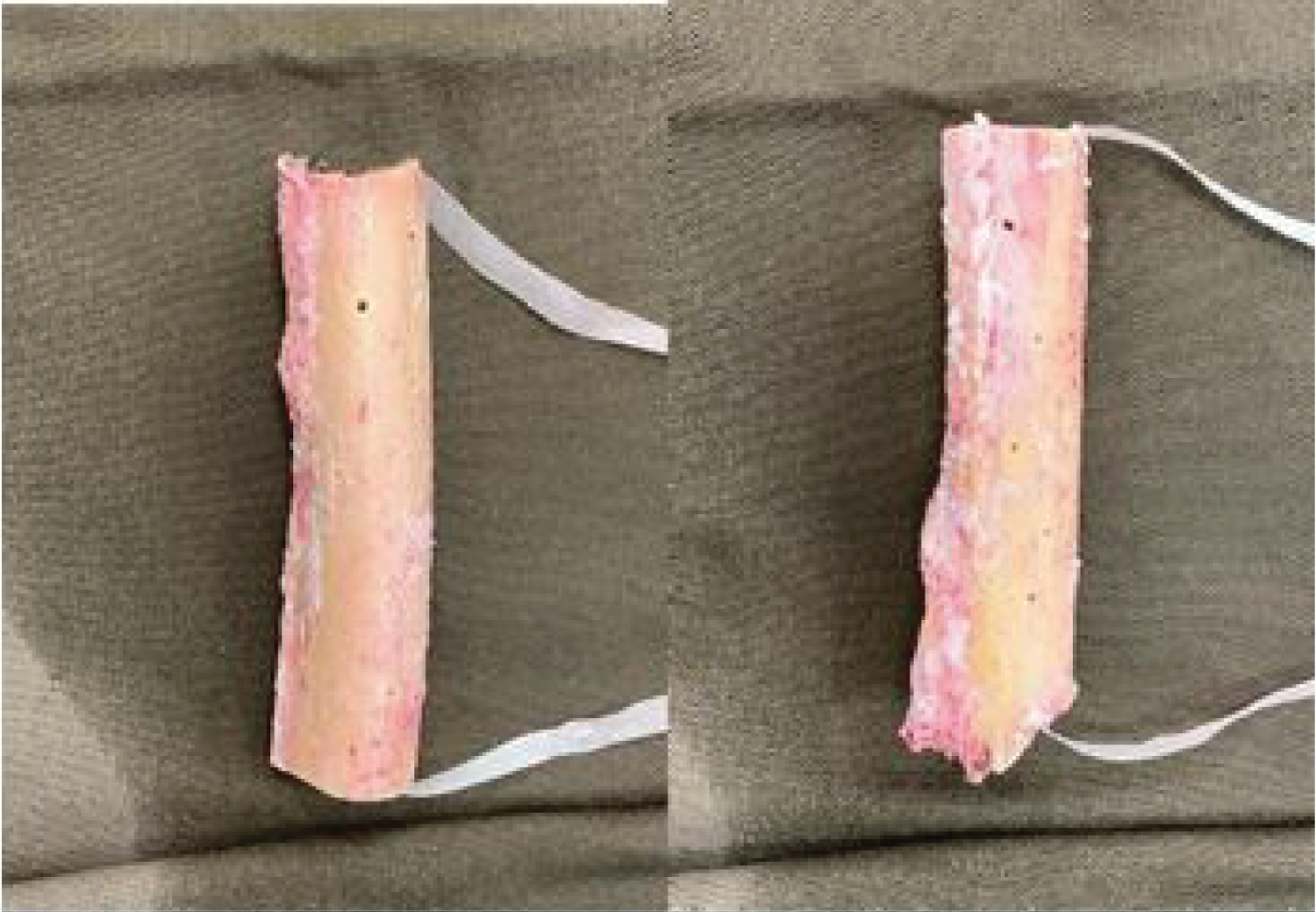
Liquid nitrogen treatment to the autograft was performed under our standardized protocol (Figure 1). After delivery of the specimen, all the soft tissue on the excised bone was removed at the back table before cryotherapy and was sent for an intraoperative frozen section and postoperative histological examination. We drilled holes on the autograft, and hung it with cotton tapes. In the induction room, the autograft was immersed in liquid nitrogen for 20 minutes (Figure 2), and thawed at room temperature for 10 mins. After that the autograft was immersed in distilled water for 15 minutes before being incorporated into the reconstruction (Figure 3). All of them were followed up for at least one year. The clinical outcome of affected limbs was assessed using the Musculoskeletal Tumor Society (MSTS) scoring system. Union time was assessed by plain radiograph, defined as complete bridging of both ends of cortexes.
Results
10 males and 11 females were treated. The age ranged from 8 to 84-years-old, with a mean of 43.8. The mean follow up time was 38.2 months (from 12 to 64 months). Six patients had loss of follow up without documented MSTS score. The mean MSTS score from 15 out of the 21 patients was 22.6 (from 12 to 30). The mean union time was 13.3 months (from 4 to 31 months). Two patients had no sign of union in the latest radiograph (Table 1).
There were two local soft tissue recurrences and one local recurrence from host bone. One patient with pelvic cervical carcinoma local soft tissue recurrence confirmed by histological examination was treated with abdominopelvic amputation. One patient with proximal femur chondrosarcoma tumor developed local soft tissue recurrence away from the autograft confirmed by MRI. The patient had lung metastasis and died of disease. The last patient with pelvic chondroid tumor had local recurrence from host bone confirmed by MRI, and was treated with palliative radiotherapy.
Five patients having wound necrosis or wound dehiscence were managed with debridement. One patient who had periprosthetic joint infection was treated with revision total knee replacement twice. One patient had screw loosening and was managed with removal of the screw.
Discussion
Limb salvage procedure for bone tumors requires tumor removal with clear margins, and subsequent reconstruction using allograft, autograft, allograft prosthetic composite [6], mega prosthesis, or distraction osteogenesis. Reconstruction using allograft has promising results [6] in clinical and radiological outcomes. However, the drawbacks, including transmission of infectious diseases, recurrence, nonunion, fracture, limited sources, need of preservation, and incompatibility, limit the use of allograft, especially in extensive bone tumor resection [7-9]. Autograft is therefore an option for biological reconstruction. Recycling techniques include autoclaving, irradiation, pasteurization, and cryotherapy. Bone graft using autoclaving has lower strength compared to that using liquid nitrogen in the biomechanical study by Norio Yamamoto [10].
Cryotherapy for malignant bone tumors was first introduced in the 1960s by Marcove RC [11], and it was well established in Japan for treatment of bone tumors in the 2000s [12].
Histological examination of bone treated with liquid nitrogen revealed no malignant cell proliferation, and decreased tumor volume [10,13,14].
In our study, there were two local soft tissue recurrences and one local recurrence from host bone. Two of them had pelvic tumors, (chondrosarcoma and cervical carcinoma respectively), and the remaining one was chondrosarcoma in the proximal femur.
For the patient with cervical carcinoma recurrence, the intraoperative frozen section confirmed a clear resection bone margin. However, the histological examination revealed soft tissue margins involvement. The autologous bone graft was removed two years and eight months after the index operation due to pelvic collection and infected tumor. Histological examination of the removed bone graft confirmed no tumor recurrence or residual tumor tissue in the autograft [15]. There was fibrous union without revitalization of the bone graft. For the femur and pelvic chondrosarcoma recurrences, the resection margins were clear based on intraoperative frozen section and final histopathology. The patient with proximal femur chondrosarcoma developed soft tissue recurrence in the thigh, and radio logically there was no local recurrence from the autograft. The pelvic chondrosarcoma had initial local recurrence at left upper posterior ilium and left lower sacrum with soft tissue from host bone. It could be explained by satellite lesions or micro metastasis. There was no radiological proof of local recurrence from the autograft. No histological examination was performed for these two patients.
In the current studies on articular cartilage chondrocytes, the effects of cryopreservation on chondrocytes were investigated. Chondrocytes could survive under liquid nitrogen, though the survival and proliferation of chondrocytes were compromised after cryopreservation.
Chondrosarcoma cells may not behave the same as chondrocytes towards cryotherapy, however there is no study on it in our literature search. Chondrosarcoma has a local recurrence rate of 20- 50%, which is higher in pelvic chondrosarcoma or high grade tumors [16]. Two out of our three recurrence cases were chondrosarcoma. Histological proof of complete eradication of chondral tumor cells will be beneficial in guiding the use of liquid nitrogen treated autograft in chondroid tumors.
In our study, the mean bone union time was 13.3 months, which was longer than the reported 6.7 months [12]. This may be limited by the retrospective review with infrequent radiological reassessment. Despite the delayed union or nonunion of the bone graft, most of the reconstructions were mechanically stable and patients were pain-free. The mean MSTS score from 15 patients was 22.6. They were satisfied with the outcome and the limb functions were mostly preserved. Long term outcome of autologous bone graft was reported with favorable results [17].
The limitations of our study include the small patient numbers, the heterogeneity in diagnoses and the various combinations of procedures.
Conclusion
Autologous bone graft treated with liquid nitrogen is a safe option for biological reconstruction of bone defects after patients underwent wide excision of bone tumors for limb salvage. It is less expensive than reconstruction with mega prosthesis, and provides satisfactory outcomes with low local recurrence rate, as well as comparable complication rate with other reconstruction methods. We shall follow our patients up for long term outcomes. Further studies on the effectiveness of chondrosarcoma eradication by liquid nitrogen may help to guide the usage of the technique in chondrosarcoma patients.
Funding
No funding was provided for the preparation of this manuscript.
Declaration of Interest
There were no conflicts of interest.
Ethical Approval
Ethical Approval was provided by the authors institution.
Consent
Written consents were obtained from the patients for publication of this case series and accompanying images. All the documentations were logged in the computerized clinical management system of the hospital.
References
- Soanes WA, Gonder MJ, Ablin RJ (1970) A possible immunocryothermic response in prostatic cancer. Clin Radiol 21: 253-255.
- Nishida H, Tsuchiya H, Tomita K (2008) Re-implantation of tumor tissue treated by cryo-treatment with liquid nitrogen induces anti-tumour activity against murine osteosarcoma. J Bone Joint Surg 90: 1249-1255.
- Nishida H, Yamamoto N, Tanzawa Y, et al. (2011) Cryo-immunology for malignant bone and soft-tissue tumors. Int J Clin Oncol 16: 109-117.
- Agha RA, Borrelli MR, Farwana R, et al. (2018) The process 2018 Statement: Updating consensus preferred reporting of case series in surgery (process) guidelines. Int J Surg 60: 279-282.
- Agha RA, Franchi T, Sohrabi C, et al. (2020) The scare 2020 guideline: Updating consensus surgical case report (scare) guidelines. Int J Surg 84: 226-230.
- Donati D, Colangeli M, Colangeli S, et al. (2008) Allograft-prosthetic composite in the proximal tibia after bone tumor resection. Clin Orthop Relat Res 466: 459-465.
- Brien EW, Terek RM, Healey JH, et al. (1994) Allograft reconstruction after proximal tibial resection for bone tumors: An analysis of function and outcome comparing allograft and prosthetic reconstructions. Clin Orthop 303: 116-127.
- Harrington KD (1992) The use of hemipelvic allografts or autoclaved grafts for reconstruction after wide resections of malignant tumors of the pelvis. J Bone Joint Surg 74: 331-341.
- Donati D, Liddo M, Zavatta M, et al. (2000) Massive bone allograft reconstruction in high grade osteosarcoma. Clin Orthop 377: 186-194.
- Yamamoto N, Tsuchiya H, Tomita K (2003) Effects of liquid nitrogen treatment on the proliferation of osteosarcoma and the biomechanical properties of normal bone. J Orthop Sci 8: 374-380.
- Marcove RC, Miller TR (1969) The treatment of primary and metastatic localized bone tumors by cryosurgery. Surg Clin North Am 49: 421-430.
- Tsuchiya H, Wan SL, Sakayama K, et al. (2005) Reconstruction using an autograft containing tumor treated by liquid nitrogen. J Bone Joint Surg Br 87: 218-225.
- Tanzawa Y, Tsuchiya H, Shirai T, et al. (2009) Histological examination of frozen autograft treated by liquid nitrogen removed after implantation. J Orthop Sci 14: 761-768.
- Yamamoto N, Inatani H, Shirai T, et al. (2012) Histological study on liquid nitrogen treated tumor- bearing bone of the proximal femur excised eight years after transplantation. Low Temp Med 38: 5-8.
- Leung ASM, Yeung MCF, Yau RCH, et al. (2021) Case report on metastatic pelvic bone tumor treated with frozen autograft by liquid nitrogen. Int J Surg Case Rep 82: 105910.
- Fromm J, Klein A, Baur Melnyk A, et al. (2018) Survival and prognostic factors in conventional central chondrosarcoma. BMC Cancer 18: 849.
- Igarashi K, Yamamoto N, Shirai T, et al. (2014) The long-term outcome following the use of frozen autograft treated with liquid nitrogen in the management of bone and soft-tissue sarcomas. Bone Joint J 96: 555-561.
Corresponding Author
Anderson SM Leung, Department of Orthopaedics and Traumatology, Queen Mary Hospital, The University of Hong Kong Pokfulam, Hong Kong.
Copyright
© 2023 Cheng CW, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.