Deltoid Ligament Repair in Bimalleolar Equivalent Ankle Fractures: A Technique Tip
Abstract
Deltoid ligament is injured in bimalleolar equivalent fractures. Though its acute repair is controversial, some recent studies have shown that anatomical reduction of the talus in the ankle mortise via deltoid repair in bimalleolar equivalent fractures correlates with better clinical outcomes. Various techniques used for Deltoid repair have relied on repairing the ligament after fibular fixation +/- syndesmostic repair. We are presenting a technique, where the fixation starts medially first, exploiting the widened medial tibiotalar clear space. This facilitates anatomic repair of both the superficial and deep components of deltoid ligament. In addition, it allows a thorough lavage of the joint and removal of loose fragments from the joint as necessary.
Keywords
Bimalleolar equivalent, Deltoid Ligament, Repair, Technique
Introduction
Deltoid ligament can rupture with supination external rotation, pronation abduction and pronation external rotation ankle injuries [1-4]. When fibular fractures are associated with medial ligamentous injury instead of medial malleolus fracture, they are considered bimalleolar equivalent fractures [5,5].
The Deltoid ligament has two main parts - superficial and deep - each with its subcomponents. Deltoid has some variable bands but the tibio-navicular and tibio-spring bands of the superficial part and posterior deep band of the deep part are the constant components [7]. The last is the thickest and strongest of all the components [6-8]. The superficial deltoid ligament is the primary restraint to eversion, while the deep deltoid prevents eversion and external rotation of the talus in the ankle mortise and tethers the talus to the medial malleolus [9-11].
The deep deltoid is avulsed from the medial malleolus in the majority of injuries, whereas intra-substance rupture and avulsion from the talus are less common [1,12,13]. A widened medial clear space on initial injury radiographs is considered an important radiological indicator of deep deltoid rupture -when this space is more than 6 mm, it has a diagnostic accuracy of about 93% [3].
Traditionally Deltoid ligament repair has not been considered necessary as a part of the treatment of unstable ankle injuries [14,15]. However, in some recent studies its repair has been reported to result in better radiological restoration of the medial clear space, congruent reduction of the talus in the mortise, and reduced post-operative medial side pain and instability [13,14,16-20]. In most of these studies, the repair was deemed necessary and carried out only if the medial clear space was found widened after lateral fixation [13,17,20]. However, we have personally noted that once the lateral side has been fixed, satisfactory repair of the deltoid ligament, in particular the deep bands, becomes technically challenging and difficult to confirm, because of the limited operating space available medially.
In this report, we describe a new technique for deltoid ligament repair that we believe has not been described before. It facilitates a precise repair of both deep and superficial parts of the deltoid ligament. We started medially before the lateral side was fixed which made definition of the medial injury and precise positioning of reparative sutures especially in the deep deltoid ligament much easier. The medial sutures were only tightened after the lateral side had been exposed and fixed as appropriate. We also report our pilot series of 8 patients, who have been prospectively followed up.
Technique
This technique was used for patients with bimalleolar equivalent ankle fractures having deltoid ligament disruption.
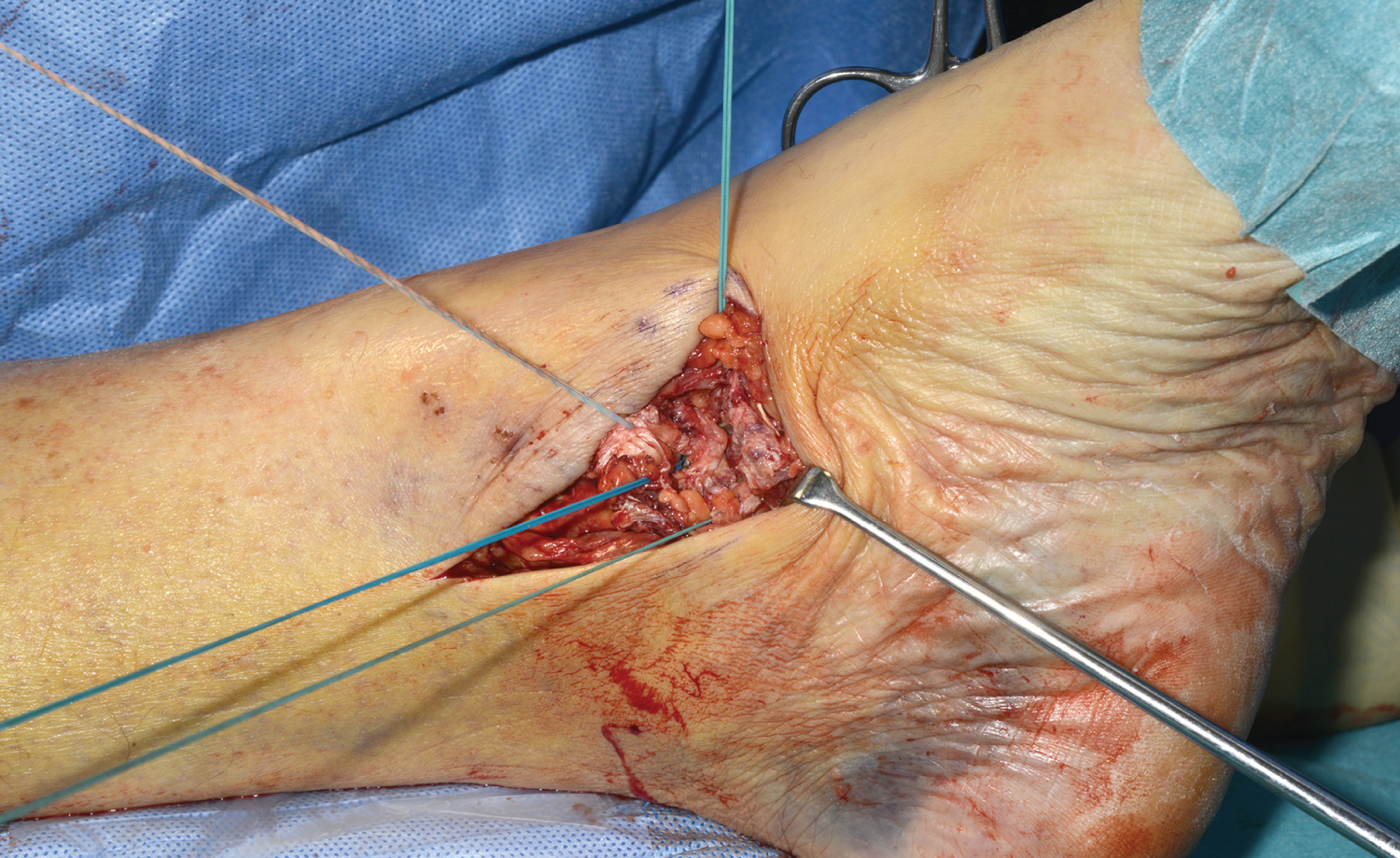
Mid-thigh tourniquet was applied but inflated only if required. The patient was positioned supine with the limb resting on two cushions. On table evaluation was done with image intensifier to endorse the widened medial tibio-talar clear space found on the injury radiographs. Medial lazy S shaped incision was used for deltoid ligament repair, starting postero-medially behind the medial malleolus crossing the tip of the medial malleolus and curving anteriorly to terminate inferiorly anterior and distal to the tip of medial malleolus. This incision may be extended proximally and distally if needed (Figure 1).
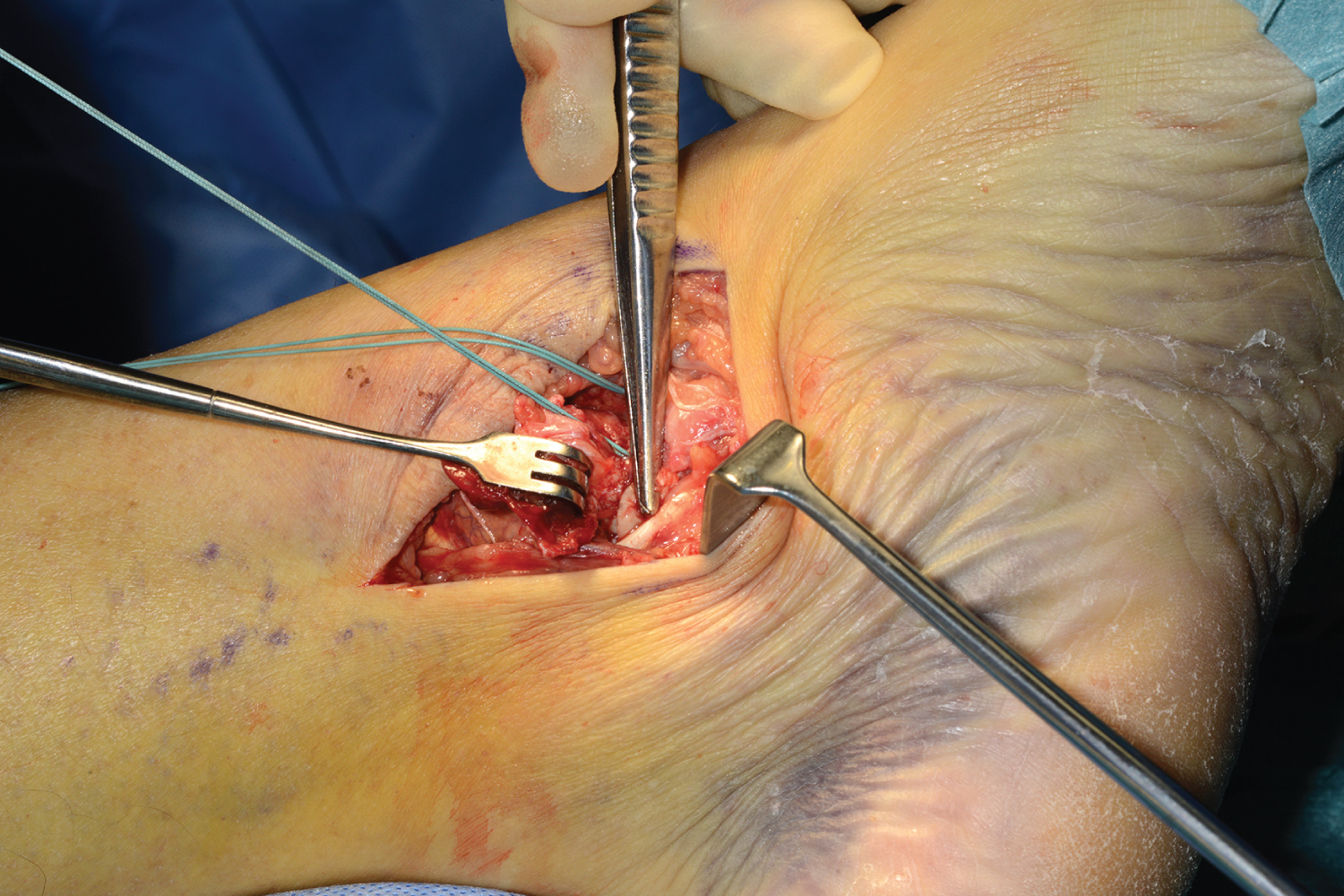
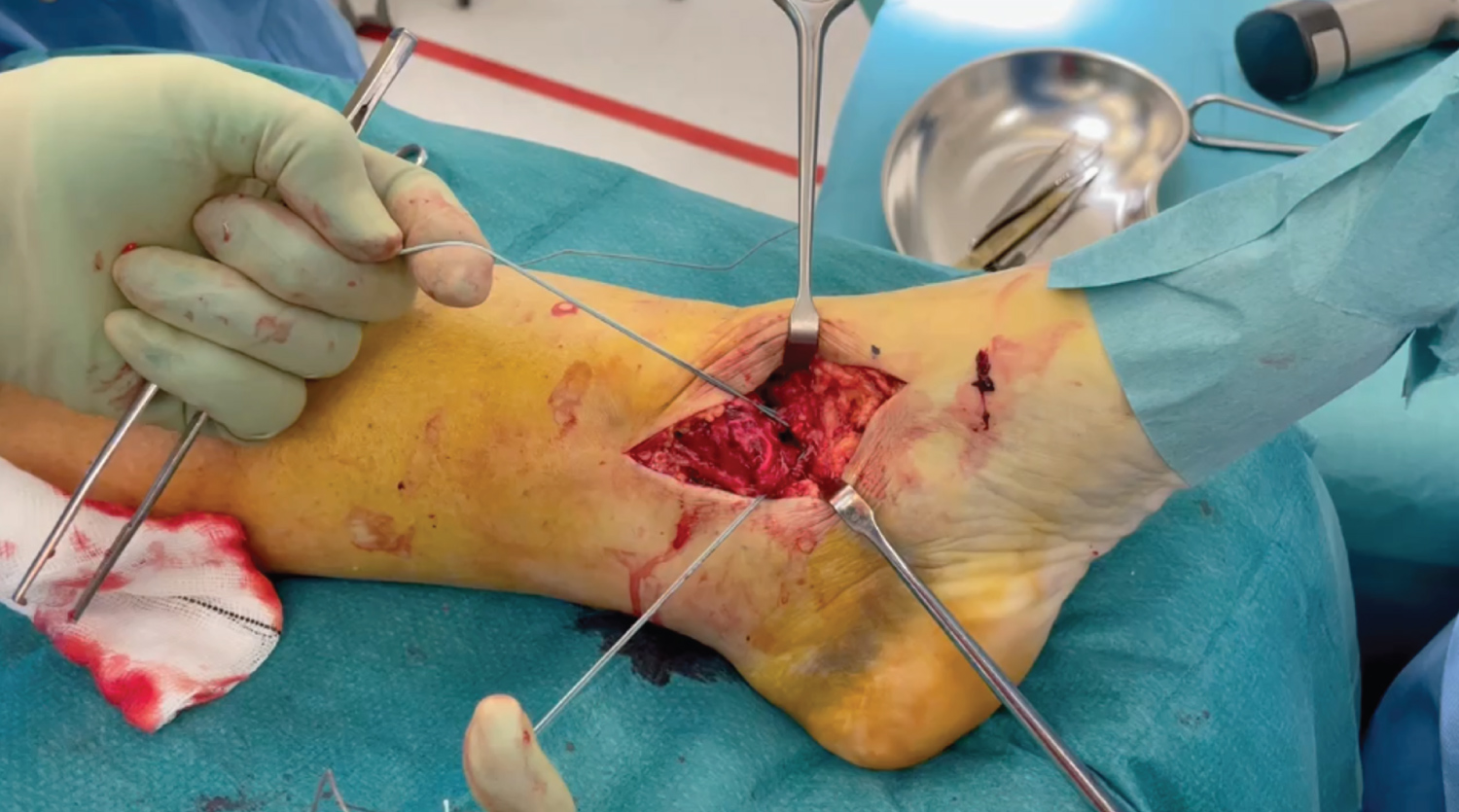
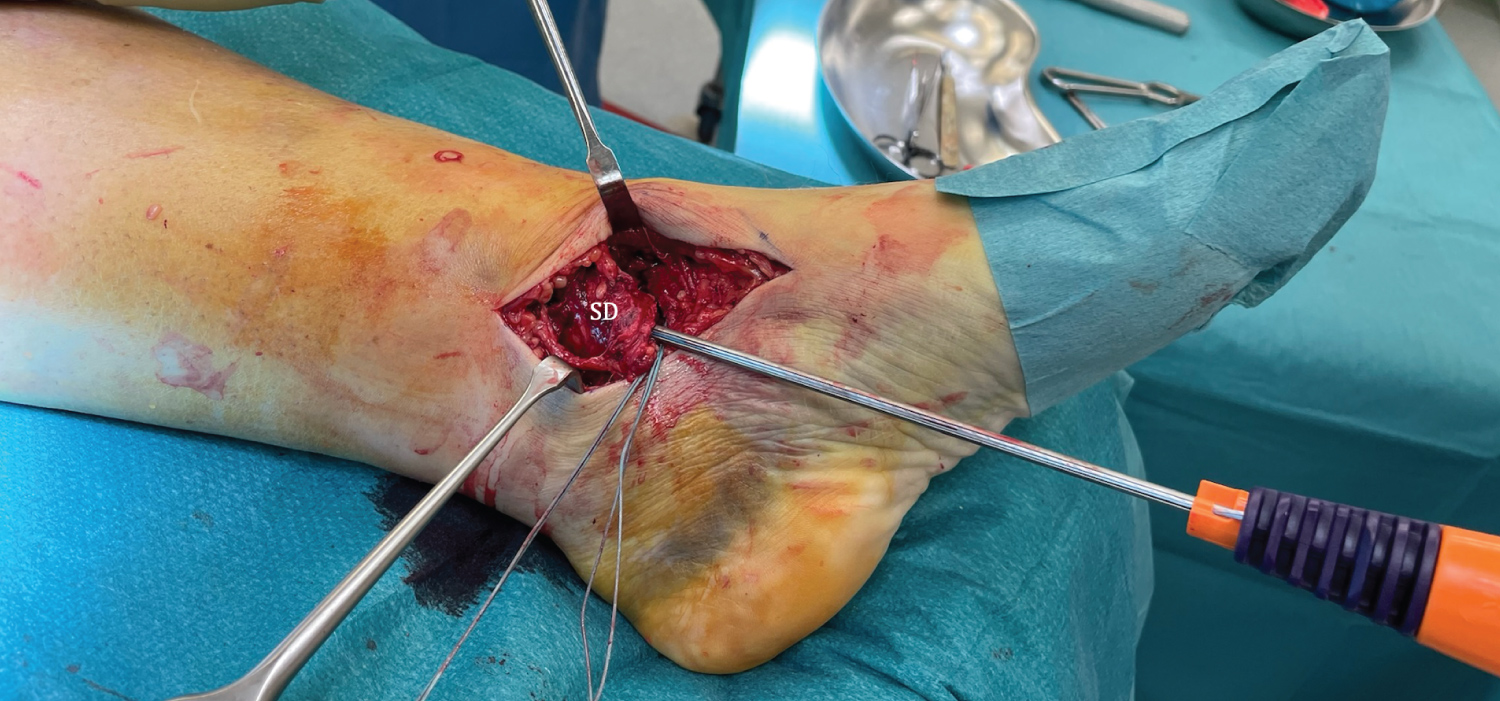
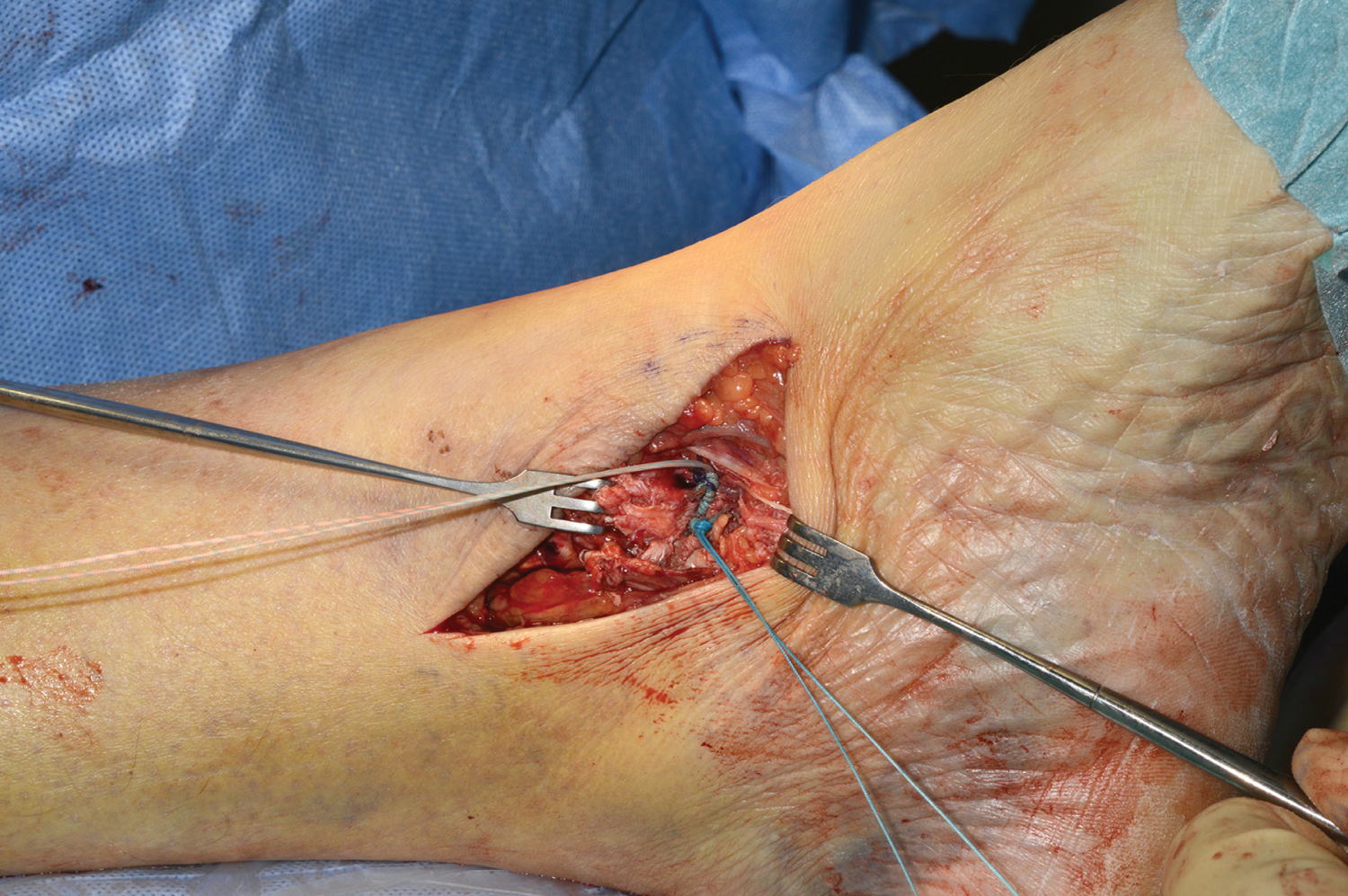
This medial exposure before lateral side fixation made the definition of medial structures better and simple (Figure 2, Figure 3 and Figure 4) and the process of deltoid ligament repair more precise.
The deltoid injury repair is carried out in the following steps.
Step 1
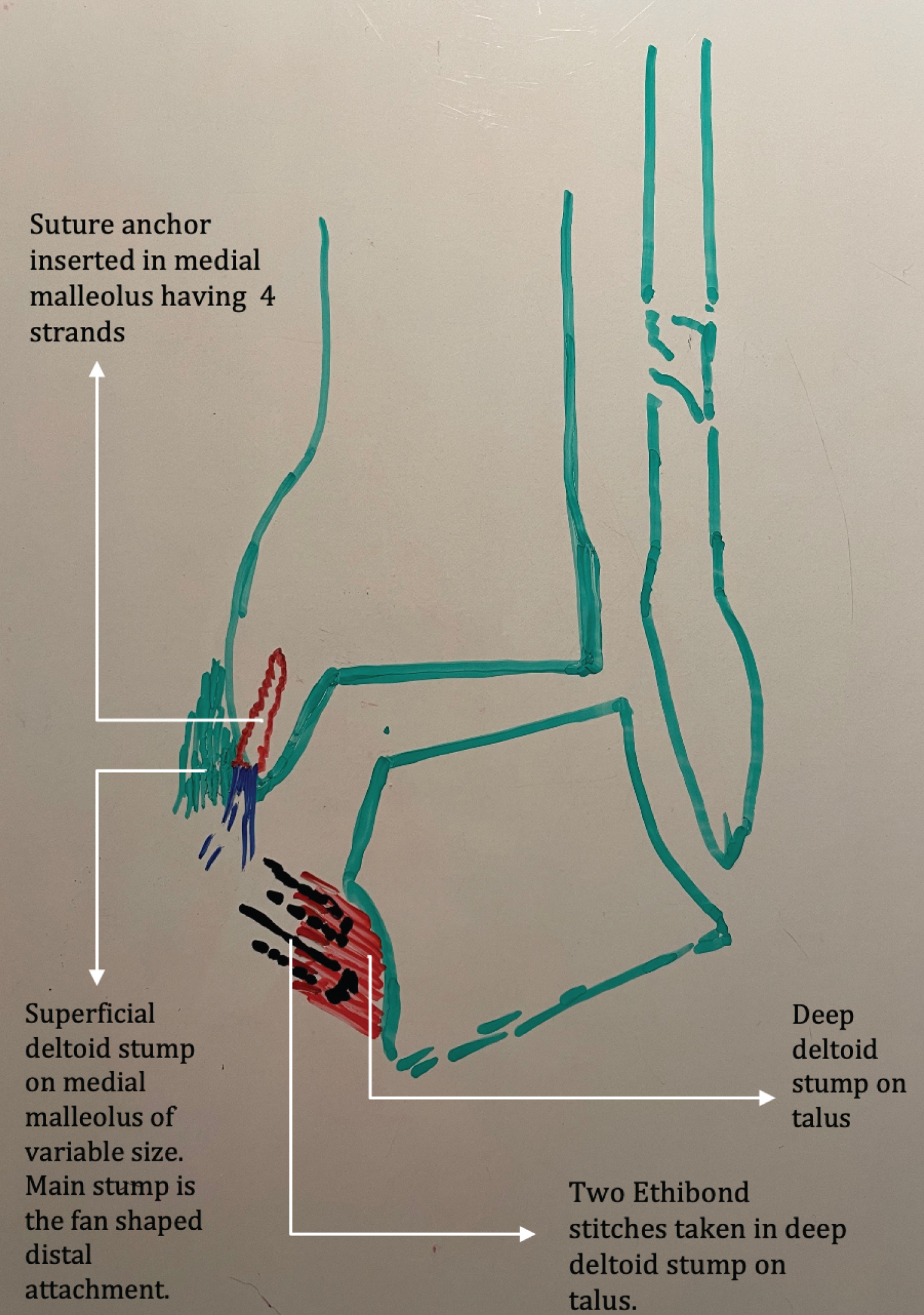
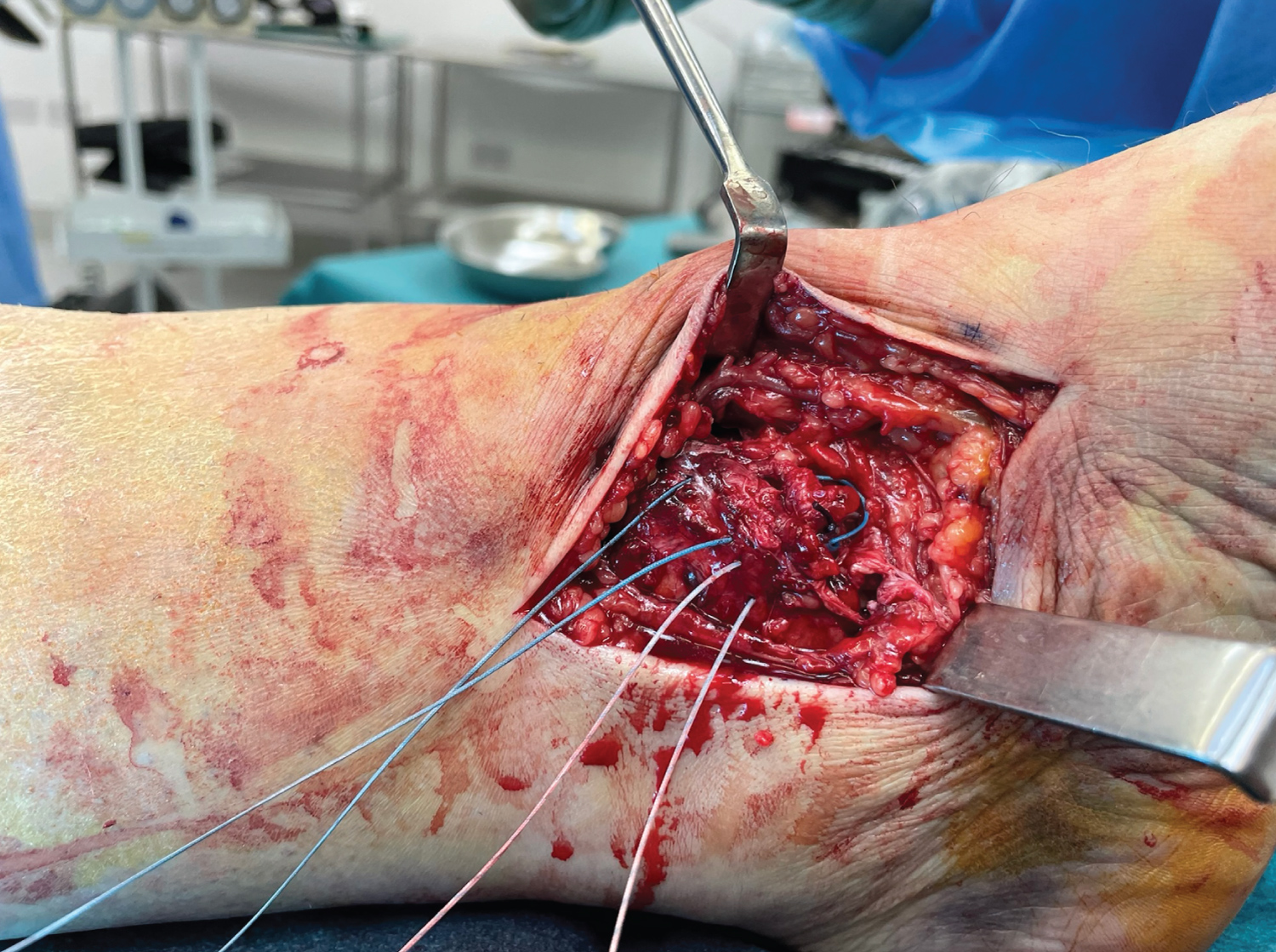
Suture placement in the deep deltoid stump on the talus and anchor placement in the medial malleolus: Since the lateral side is still mobile, after exposing the medial side via the above incision, the talus is displaced laterally in the mortise for better visualization of the deep deltoid attachment. If necessary, the tibialis posterior tendon sheath may be opened, and the tendon retracted posteriorly and inferiorly to expose the posterior deep deltoid ligament stump on the talus. Two Ethibond stitches are precisely placed in the anterior and posterior bands of the talar stump of the deep deltoid ligament (Figure 4 and Figure 5).
Thereafter, a suture anchor (Smith & Nephew Twin fix suture anchor size 3.5/4.5 mm, or Arthrex 3.5 mm Corkscrew suture anchor) with four strands is inserted after pre-drilling the medial malleolus (Figure 6). Once the sutures and the anchor are in place, we move our attention to the lateral side; at this stage, the medial sutures are left untied.
Step 2
Lateral fixation: The lateral side is fixed as routine using standard techniques, including lag screw application (where necessary), fibular plating +/-syndesmostic fixation as appropriate (Figure 7).
Step 3
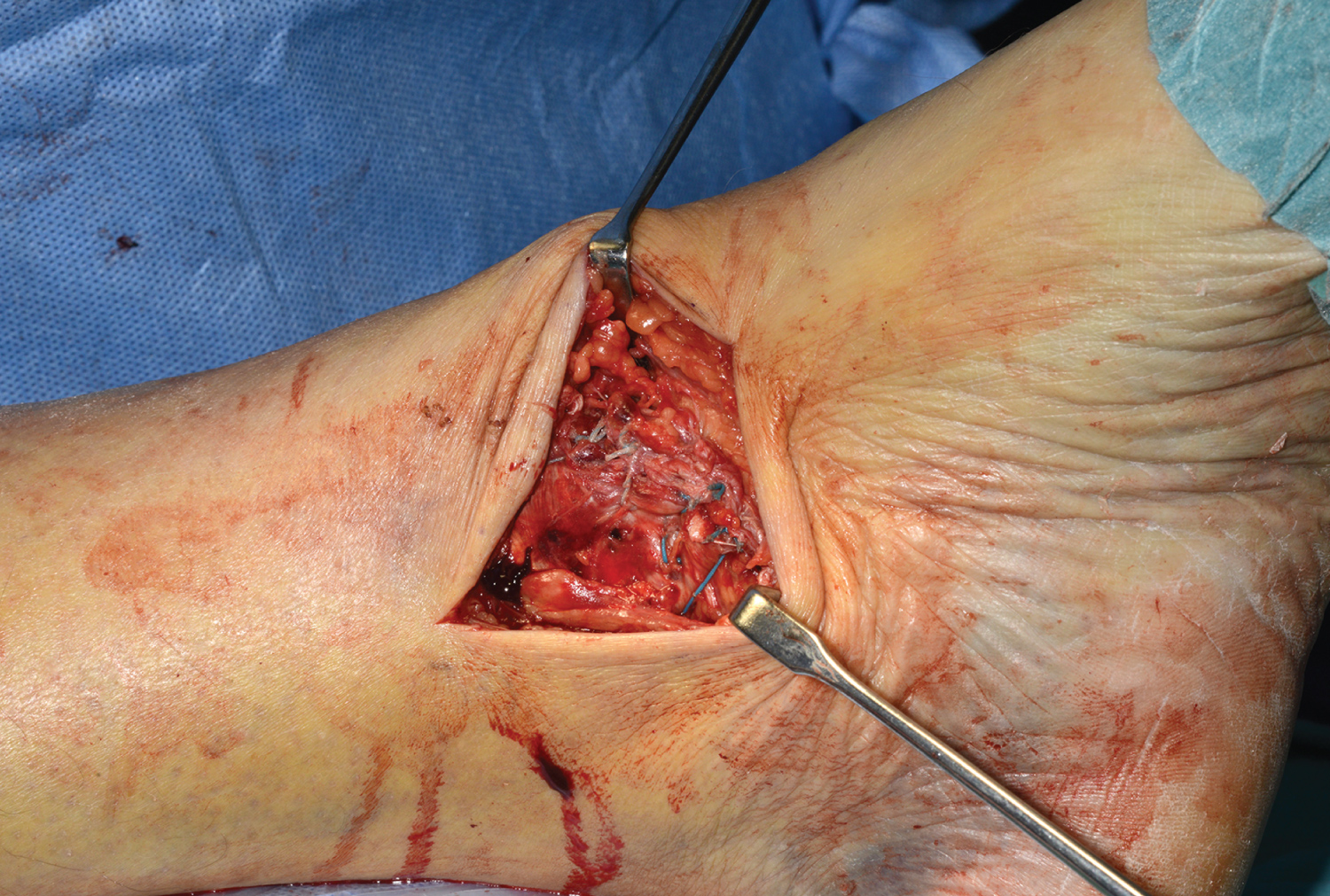
Repair of deep deltoid: Once lateral fixation is complete, we return to the medial side to tie off the medial sutures thus repairing the deep deltoid ligament. The ends of the ethibondsuture from the anterior deep deltoid ligament stitch are tied to the one of the two sets of sutures (blue or striped) on the medial malleolus suture anchor and those from the posterior deep deltoid are tied to the remaining set of the suture anchor strands (Figure 8). The deep deltoid sutures are then cut, while the threads of the anchor conserved for the next step (Figure 9).
Stage 4
Superficial deltoid ligament repair: The four strands of the anchor suture (Figure 10) are now passed through the superficial deltoid ligament (Figure 11) and tied off on its surface in a fan-shaped configuration repairing the subcomponents of superficial deltoid ligament. This suture generally approximates the edges of the torn superficial ligament anatomically (Figure 12) and then can be cut off. This technique also ensures that the sutures securing the deep deltoid ligament are buried under the superficial deltoid repair and thus unlikely to contribute to any soft tissue irritation post-op.
Discussion
Deltoid ligament is an important medial stabilizer of ankle [8,21-23]. Its two components together prevent anterior, posterior and lateral translation of the talus within the mortise as well limit its tilting.
In some recent studies, deltoid ligament repair in bimalleolar equivalent ankle fractures has been reported to give better radiological restoration of the medial clear space and better functional outcomes [13,16-19,24]. In the majority of them, the lateral side was fixed first and the medial repair only considered (and carried out) if the medial clear space was found to be wider than expected at the end of fibular +/- syndesmotic fixation [13,17,20].
The difficulty with this treatment sequence is that the lateral fixation closes the space on the medial side and makes assessment and repair of the deltoid ligament, especially its deep component, extremely difficult and generally unsatisfactory (unless one is willing to undo the lateral fixation or use extensile medial approaches). Placement of sutures in the stump of the deep ligament or suture anchors in the surface of the talus can be especially challenging and risks a suboptimal repair and/or articular cartilage damage.
In the current study, opening the medial side before securing the lateral allowed us to rotate, displace and translate the talus in the mortise as necessary, thus facilitating accurate assessment of the deltoid injury and optimum positioning of reparative sutures and anchors. This also improved access to other important medial structures like the tibialis posterior tendon and the medial ankle articular surface for assessment and repair as appropriate.
In our series, the tip of medial malleolus was found devoid of the attachment of deep deltoid ligament, however there was variable size stump of the superficial deltoid at or proximal to the tip of medial malleolus for sutures placement (Figure 2). The ruptured deep deltoid part was often found with a stump on the talus and avulsed from the medial malleolus (Figure 2 and Figure 4). This indicates variable rupture pattern of superficial and deep deltoid ligaments as has been reported in other studies too [6]. To further consolidate this knowledge, future per-operative and MRI studies would be helpful.
Different repair configurations have been recommended for deltoid ligament repair with the objective of ligament to bone healing in cases of avulsion injuries and end to end healing of ligament in cases of mid substance ruptures. For avulsion injuries, an anchor may be placed in the bone from where the ligament has avulsed - medial malleolus, talus, or sustentaculum tali, and for the end to end repair, different suture techniques have been used [5,6,12,13,17,24].
In our technique, the deep deltoid was repaired with a suture anchor in the medial malleolus and stiches in its talar stump (Figure 4, Figure 5, Figure 6, Figure 8, Figure 9 and Figure 10). For repair of the superficial deltoid, the sutures from the anchor were used, brought out on the surface of the superficial deltoid ligament, thus avoiding the need for more suture material with the added benefit of secure additional anchorage of the superficial deltoid repair (Figure 11 and Figure 12).
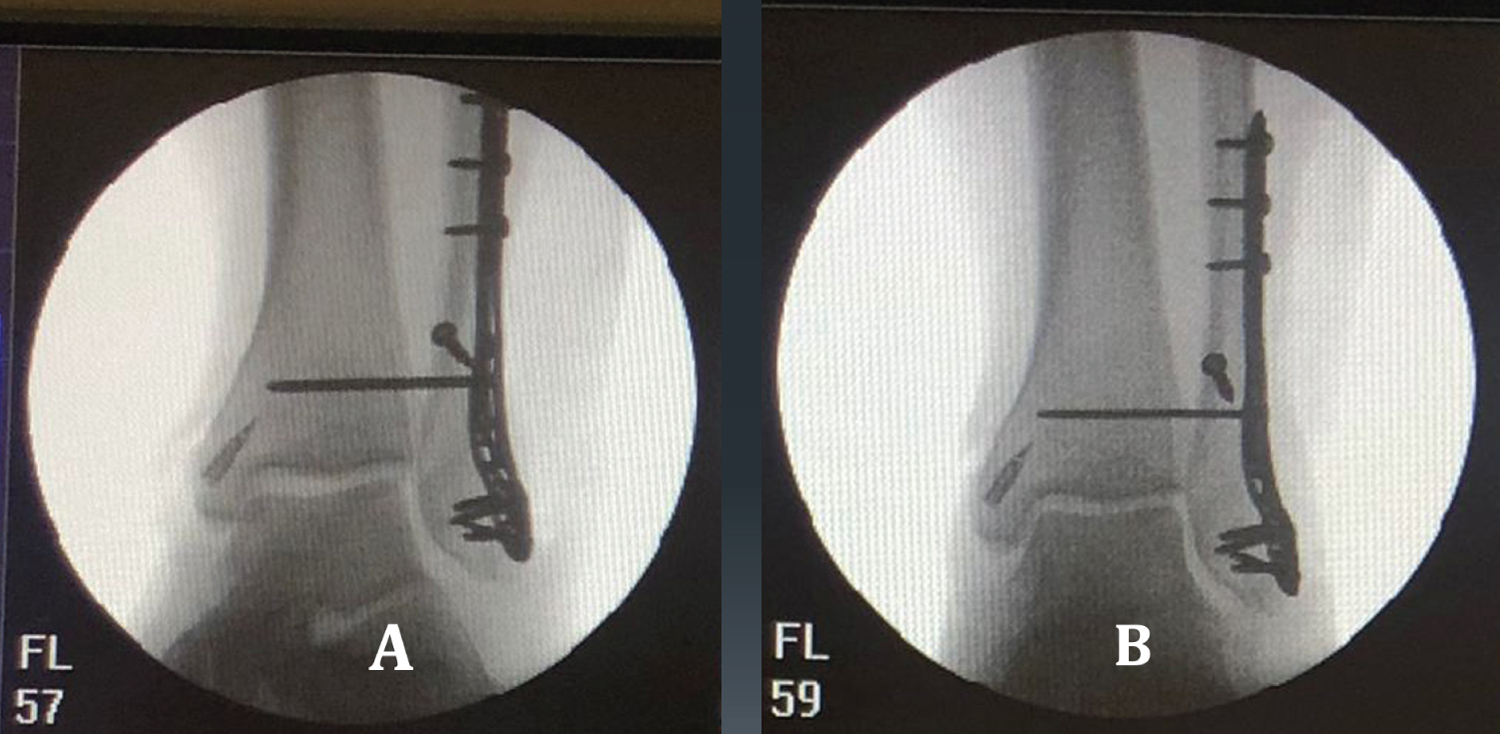
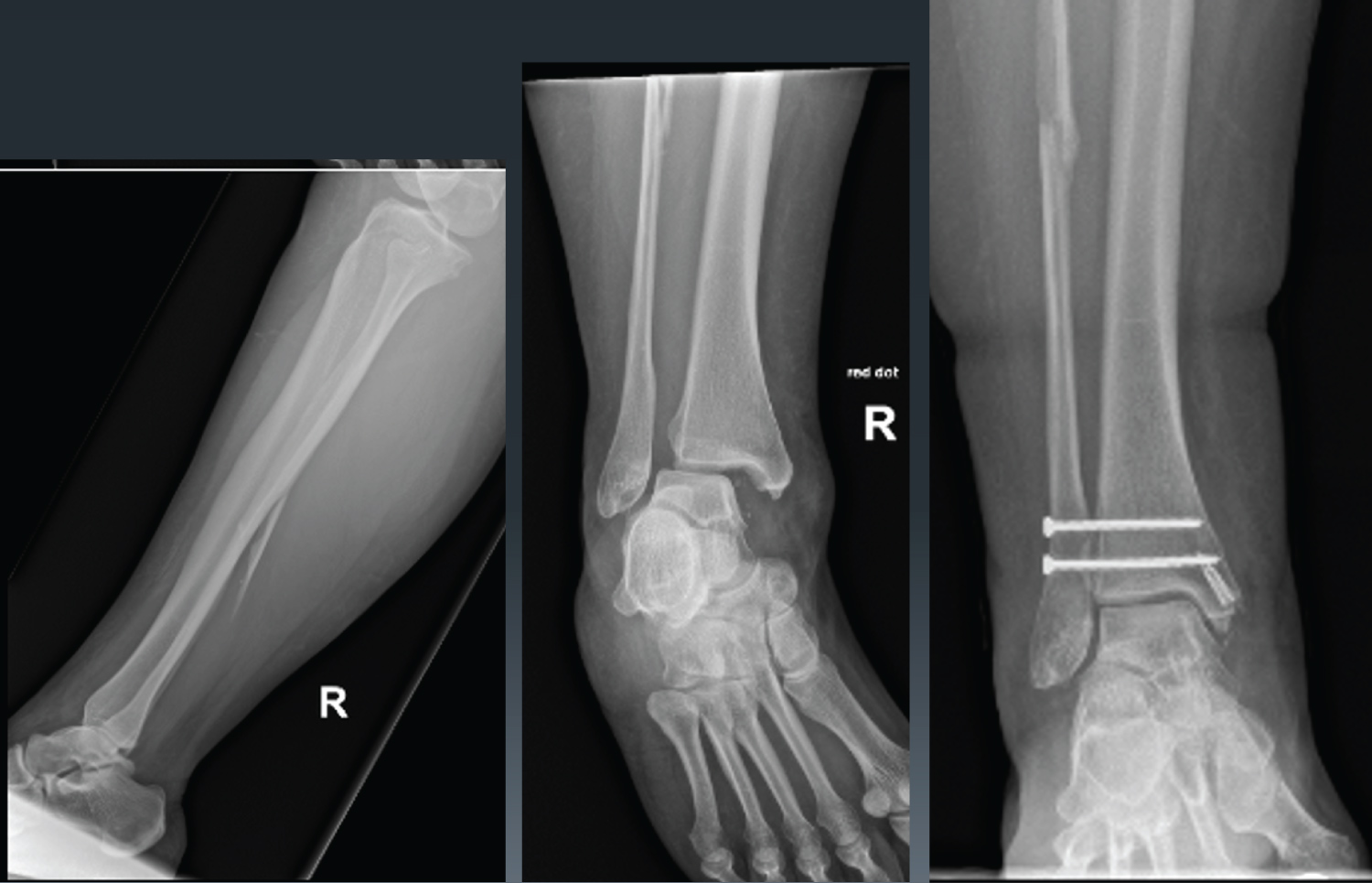
In some cases, we found on per-operative imaging, that before tying and tightening the medial repair stiches, the medial space and ankle mortise was not congruently reducing or stabilising in spite of lateral side fixation. The congruence and stability of the medial clear space and ankle mortise was always restored on tying and tightening the deltoid repair sutures (Figure 13). This for us, highlighted the importance of deltoid ligament repair for adequate reduction of the ankle mortise. Also, these patients were found to maintain their congruent reduction in post-operative weight bearing radiographs (Figure 14).
Conclusion
The current described technique affords improved access to the medial ligamentous and bony structures making possible a precise and strong anatomic repair of the superficial and deep deltoid ligament. Such a repair permits the congruent reduction of the talus in the ankle mortise, which in turn should permit full and predictable recovery of ankle function.
References
- Hintermann B, Knupp M, Pagenstert GI (2006) Deltoid ligament injuries: Diagnosis and management. Foot Ankle Clin 11: 625-637.
- Tornetta P 3rd (2000) Competence of the deltoid ligament in bimalleolar ankle fractures after medial malleolar fixation. J Bone Joint Surg Am 82: 843-848.
- Schuberth JM, Collman DR, Rush SM, et al. (2004) Deltoid ligament integrity in lateral malleolar fractures: A comparative analysis of arthroscopic and radiographic assessments. J Foot Ankle Surg 43: 20-29.
- Panchani PN, Chappell TM, Moore GD, et al. (2014) Anatomic study of the deltoid ligament of the ankle. Foot Ankle Int 35: 916-921.
- Jones CR, Nunley JA (2015) Deltoid ligament repair versus syndesmotic fixation in bimalleolar equivalent ankle fractures. J Orthop Trauma 29: 245-249.
- Lee S, Johnny Lin, Hamid KS, et al. (2019) Deltoid ligament rupture in ankle fracture: Diagnosis and management. J Am Acad Orthop Surg 27: e648-e658.
- Milner CE, Soames RW (1998) Anatomy of the collateral ligaments of the human ankle joint. Foot Ankle Int 19: 757-760.
- Campbell KJ, Michalski MP, Wilson KJ, et al. (2014) The ligament anatomy of the deltoid complex of the ankle: A qualitative and quantitative anatomical study. J Bone Joint Surg Am 96: e62.
- Clarke HJ, Michelson JD, Cox QG, et al. (1991) Tibio-talar stability in bimalleolar ankle fractures: A dynamic in vitro contact area study. Foot Ankle 11: 222-227.
- Earll M, Wayne J, Brodrick C, et al. (1996) Contribution of the deltoid ligament to ankle joint contact characteristics: A cadaver study. Foot Ankle Int 17: 317-324.
- Rasmussen O, Kromann-Andersen C, Boe S (1983) Deltoid ligament. Functional analysis of the medial collateral ligamentous apparatus of the ankle joint. Acta Orthop Scand 54: 36-44.
- Lack W, Phisitkul P, Femino JE (2012) Anatomic deltoid ligament repair with anchor-to-post suture reinforcement: Technique tip. Iowa Orthop J 32: 227-230.
- Woo SH, Bae SY, Chung HJ (2018) Short-term results of a ruptured deltoid ligament repair during an acute ankle fracture fixation. Foot Ankle Int 39: 35-45.
- Zeegers AV, van der Werken C (1989) Rupture of the deltoid ligament in ankle fractures: Should it be repaired? Injury 20: 39-41.
- Strömsöe K, Höqevold HE, Skjeldal S, et al. (1995) The repair of a ruptured deltoid ligament is not necessary in ankle fractures. J Bone Joint Surg Br 77: 920-921.
- Johnson DP, Hill J (1988) Fracture-dislocation of the ankle with rupture of the deltoid ligament. Injury 19: 59-61.
- Zhao HM, Lu J, Zhang F, et al. (2017) Surgical treatment of ankle fracture with or without deltoid ligament repair: A comparative study. BMC Musculoskelet Disord 18: 543.
- Yu GR, Zhang M-Z, Aiyer A, et al. (2015) Repair of the acute deltoid ligament complex rupture associated with ankle fractures: A multicenter clinical study. J Foot Ankle Surg 54: 198-202.
- Butler BA, Hempen EC, Barbosa M, et al. (2020) Deltoid ligament repair reduces and stabilizes the talus in unstable ankle fractures. J Orthop 17: 87-90.
- Wu K, Lin J, Huang J, et al. (2018) Evaluation of transsyndesmotic fixation and primary deltoid ligament repair in ankle fractures with suspected combined deltoid ligament injury. J Foot Ankle Surg 57: 694-700.
- Boden SD, Labropoulos PA, McCowin P, et al. (1989) Mechanical considerations for the syndesmosis screw. A cadaver study. J Bone Joint Surg Am 71: 1548-1555.
- Harper MC (1987) Deltoid ligament: An anatomical evaluation of function. Foot Ankle 8: 19-22.
- Harper MC (1988) The deltoid ligament. An evaluation of need for surgical repair. Clin Orthop Relat Res 226: 156-168.
- Hardy MA, Connors JC, Zulauf EE, et al. (2020) Acute deltoid ligament repair in ankle fractures: Five-year follow-up. Clin Podiatr Med Surg 37: 295-304.
Corresponding Author
Shakir Hussain, FRCS, FCPS, MRCS, MBBS, Department of Trauma and Orthopaedic Surgery, Queen's Hospital, Rom Valley Way, Romford, RM7 0AG, United Kingdom, Tel: +447-831-578-392
Copyright
© 2023 Hussain S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.