A Simple Intraoperative Technique to Help Prevent Malreduction of the Syndesmosis during Ankle Fracture Fixation
Keywords
Syndesmosis, K-wire, Ankle, Fracture, Malreduction
Introduction
Malreduction of the syndesmosis during fixation of ankle fractures is often missed on radiographs, and is reported in over 50% of cases when confirmed with CT scans [1]. Malreduction may be caused by misplacement of reduction clamps and screws [2] and is associated with pain, instability and poorer functional outcomes, as well as the need for re-operation [3]. We report a simple intraoperative technique to help prevent syndesmosis malreduction. This technique is especially useful in comminuted 'Weber C' patterns of fracture.
Technique
The patient is positioned supine on a radiolucent table, and image intensifier is used throughout the procedure, obtaining AP and lateral views to check the adequacy of reduction. It is the authors preference to place a sandbag beneath the ipsilateral buttock, the lower leg elevated on a foam block, and an above knee tourniquet is used.
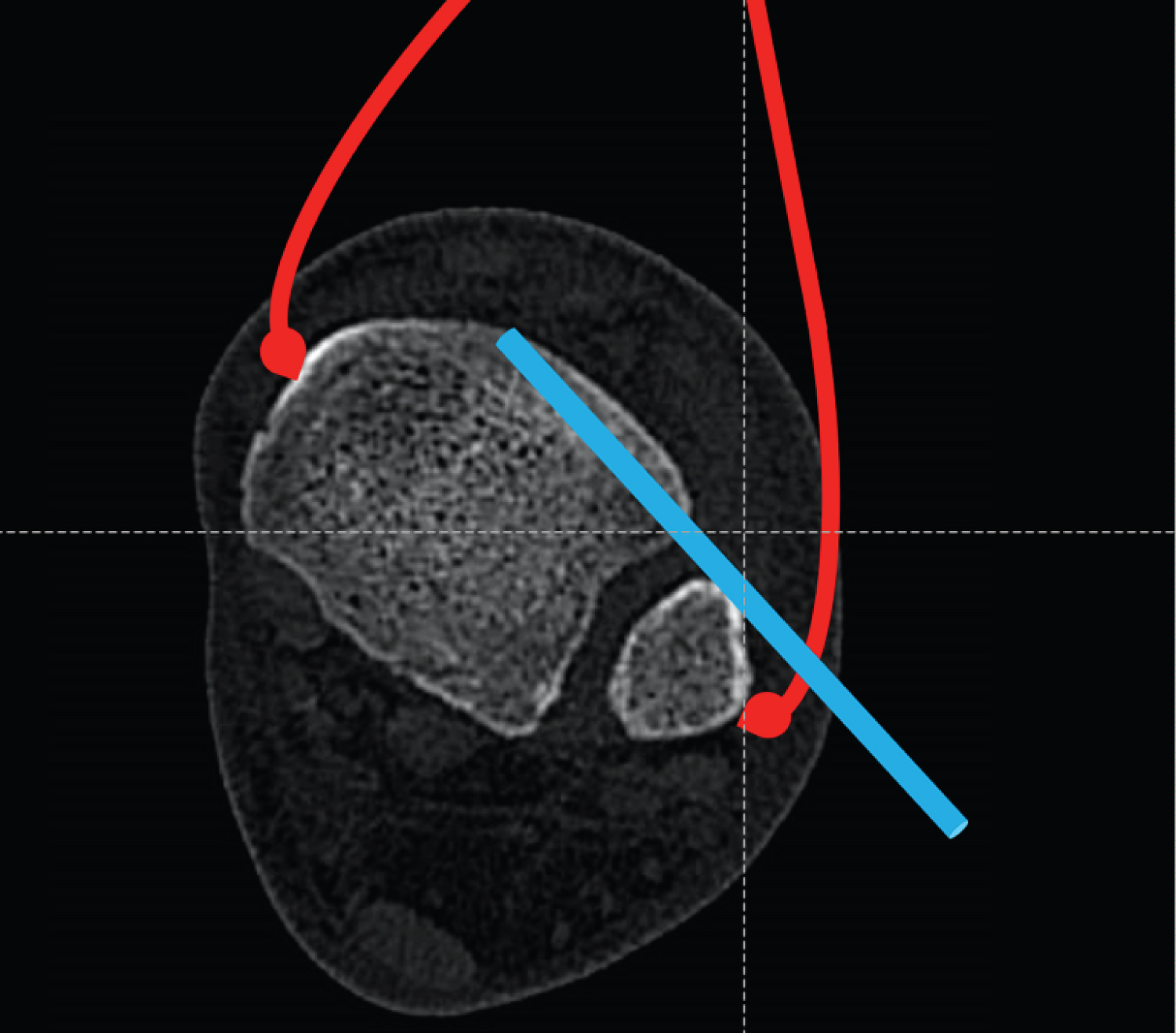
After restoration of fibular anatomy ensuring correction of length and rotation, and near anatomical fixation of other malleoli as necessary, the distal lateral incision is extended anteriorly. The anterior inferior tibiofibular ligament (AITFL), which is usually torn is identified and the incisura cleared of interposing soft tissue. The anterior ridge of the incisura is felt, over the anterior border of the fibula. A 2.0 mm k-wire is passed through the anterior ridge, parallel to the ankle joint from lateral to medial, and in the same plane as the anterior tibia. A pointed reduction clamp (e.g. Synthes® periarticular reduction forceps) is used to reduce the fibula within the incisura with the ankle in dorsiflexion. The k-wire provides a buttress to reduce the fibula into the incisura (Figure 1). Fibular length can be restored by traction on the lateral malleolus in cases of high fibular fractures with shortening (Figure 2). Fixation is then performed using the surgeon's preferred method, after which the clamp and k-wire are removed. It is our preference to use a 3.5 mm cortical screw through three cortices to stabilise the syndesmosis.
Expected Outcomes
This simple technique using a k-wire as an anterior block can help prevent malreduction of the fibula within the incisuradue to over-compression when fixing an ankle fracture with syndesmosis injury. This step may prevent the complications and need for re-operation reported in the literature.
Complications
This approach extends the most commonly used lateral incision for ankle fracture fixation. Injury to the superficial peroneal nerve can be prevented by identification and avoidance of overzealous retraction. The k-wire could break and require additional dissection for removal during the procedure. If a screw is used to stabilise the syndesmosis then fatigue failure may occur when the patient mobilises. However, this is unrelated to the intraoperative technique to prevent malreduction.
Conflicts of Interest
No conflicts of interest to declare.
References
- Gardner MJ, Demetrakopoulos D, Briggs SM, et al. (2006) Malreduction of the tibiofibular syndesmosis in ankle fractures. Foot Ankle Int 27: 788-792.
- Miller AN, Barei DP, Iaquinto JM, et al. (2013) Iatrogenic syndesmosis malreduction via clamp and screw placement. J Orthop Trauma 27: 100-106.
- Sagi HC, Shah AR, Sanders RW (2012) The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-Up. J Orthop Trauma 26: 439-443.
Corresponding Author
Rory Morrison, FRCS, Department of Trauma and Orthopaedics, Northumbria Healthcare NHS Foundation Trust, Rake Lane, North Shields, NE29 8NH, USA
Copyright
© 2022 Morrison R, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.