Hybrid Fixation of Failed Internally Fixed Distal Femoral Fracture with an Extramedullary Locking Plate and an Intramedullary Cortical Strut Allograft Construct- A Case Report
Abstract
Introduction: Fractures in osteoporotic bones present a surgical challenge for fixation and are often associated with significant morbidity.
Case presentation: We present a case of failed internal fixation of fracture femoral shaft in a 74-year-old patient with osteoporosis. Fracture fixation was undertaken using an extra medullary locking plate and an intramedullary cortical strut graft, a hybrid fixation technique, a Locking Plate Allograft Construct.
Discussion: Bone grafts are often used to support the native bone. By using a hybrid technique, the locking plate allograft construct achieves an enhanced stability of fracture fixation compared to plate alone, thus improving the outcome of surgery in osteoporotic bone fractures.
Conclusion: Hybrid fixation using locking plate allograft constructs are relatively easy to perform and provide superior fixation to routine methods in osteoporotic bone fractures.
Keywords
Case report, Bone fracture, Locking plate allograft construct, Hybrid fixation
Introduction
Long bone fractures in patients with osteoporosis are a common source of morbidity and increasing mortality in the elderly population [1,2]. Osteoporotic bones are characterized by a decrease in bone mineralization, leading to reduced cortical thickness [2].
Fixation of fractures in osteoporotic bones can be a surgical challenge and they are often associated with delayed healing [3,4]. Poor quality of bone, pattern and configuration of the fracture, non-union of the fracture, rigidity of fixation and implant-bone construct fatigue may result in failure of fixation [1,2].
Various implant fixation techniques have been described to manage fractures in an osteoporotic bone, and systemic agents have also been used to expedite bone healing. We describe a hybrid fixation technique using a long extra medullary locking plate supplemented with an intramedullary cortical strut graft, creating a Locking Plate Allograft Construct (PAC).
Case Presentation
Patient information
A 74-year-old lady with osteoporosis underwent retrograde intramedullary nailing of the right distal femoral fracture. She presented 4 weeks later with catastrophic failure of fixation. Plain radiographs showed that the femoral nail cut-out distally, with posterior displacement of the distal segment (Figure 1a and Figure 1b). She was obese and had significant medical comorbidities.
Therapeutic intervention
This patient underwent revision surgery to stabilize the fracture. Revision procedure involved the removal of intramedullary nail and application of a hybrid fixation, with a combination of an extramedullary locking plate and an intramedullary cortical strut allograft construct (PAC).
Patient was positioned supine with a bolster under the right knee and a sand-bag under the ipsilateral buttock. Left lateral table supports were applied to the radiolucent operating table to enable tilting of the table.
Patient was given general anaesthesia and intravenous Augmentin was administered at induction. An incision incorporating the scar on the anterior aspect of the right knee was made and the femoral nail was removed after carefully removing the proximal locking screws, the distal locking screw and the spiral blade. Intra-operative findings included a comminuted femoral fracture, bone loss, a sleeve fracture of the trochlear cartilage, and soft bone.
Femoral fracture was approached laterally, reduced, and held with three Synthes cables (DePuy Synthes, Leeds, UK). Stability was further augmented by introducing a long cortical strut graft through the distal femoral entry point used for nailing, into the femoral intramedullary canal to achieve internal splintage of the fracture. Satisfactory alignment and stability were achieved with the inlay cortical strut graft and cables (Figure 2).
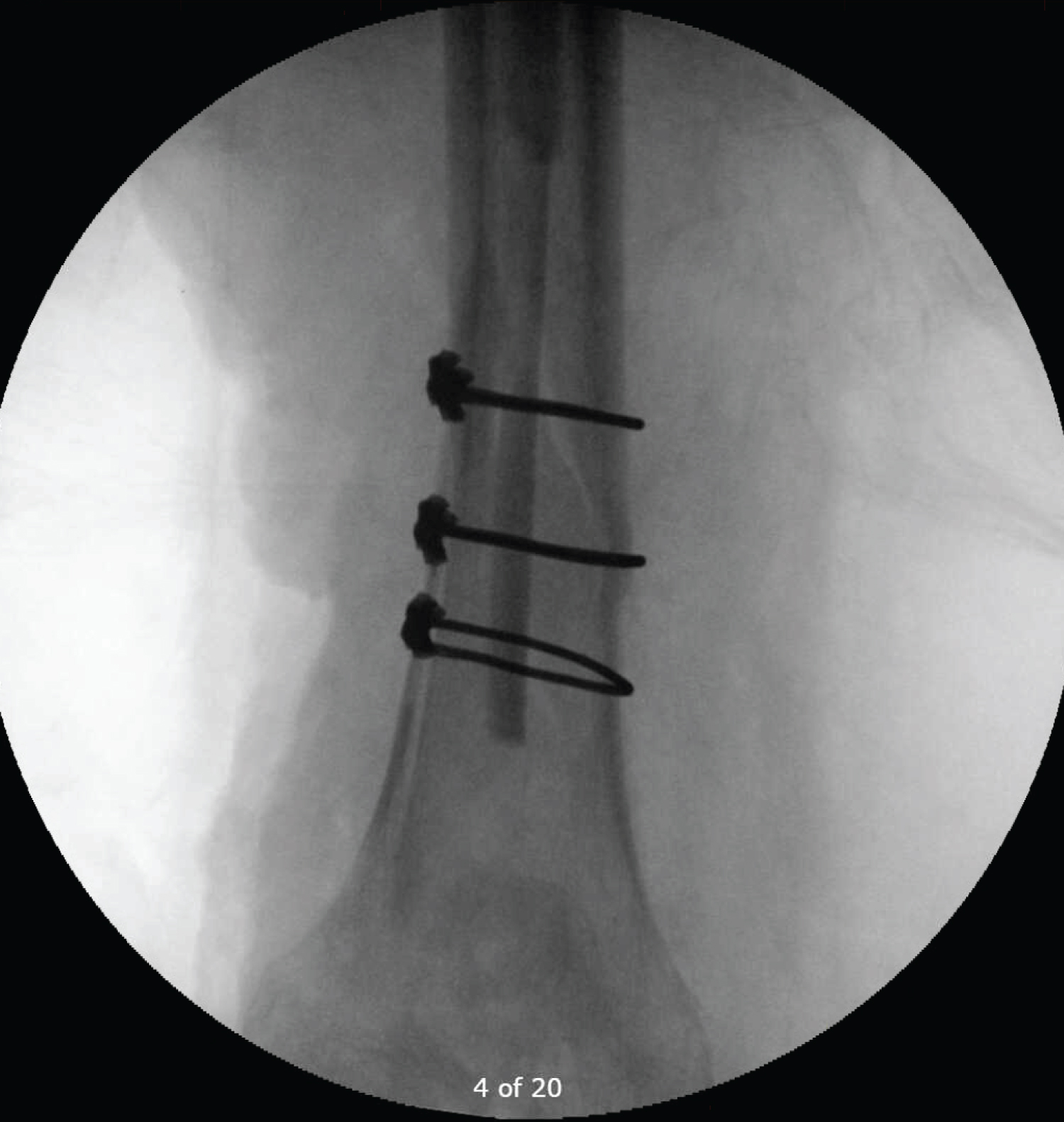
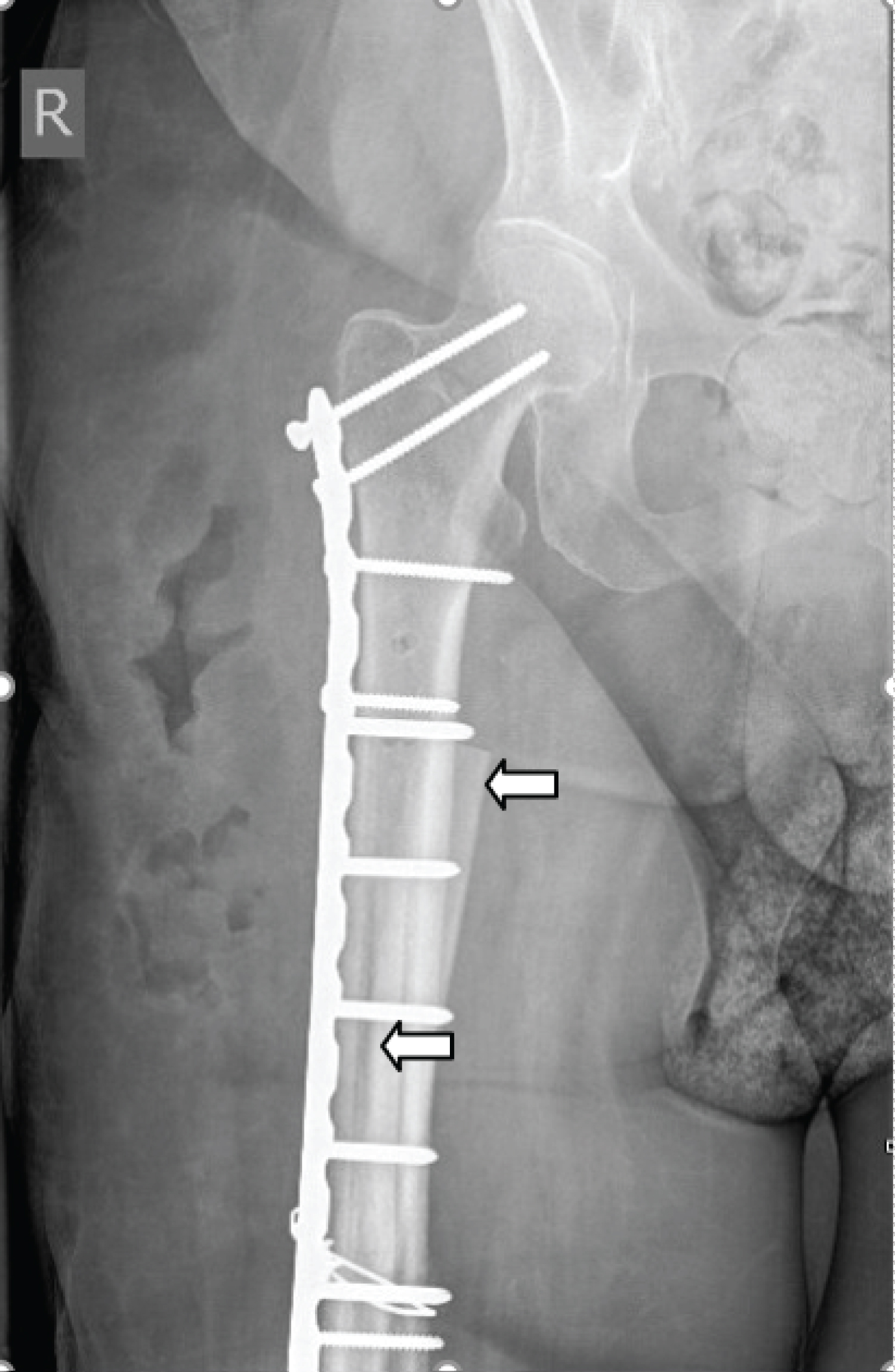
Secondary stability was achieved with a percutaneously and submuscularly applied extramedullary 18-hole Synthes variable angle locking plate (DePuy Synthes, Leeds, UK), spanning the full length of the femur. A combination of locking screws, cortical screws and cables were used (Figure 3). At least four cortical screws were inserted to transfix the intramedullary strut graft to the plate, achieving a tetra-cortical purchase for each of the screws (Figure 4). Two cortical screws were placed in the right proximal femoral head and neck, stabilizing the entire length of the femur. A second onlay strut allograft was placed anteriorly and proximally to provide additional torsional stability (Figure 5). This strut graft was stabilized and locked to the plate and the native femur with two locking Synthes cables (DePuy Synthes, Leeds, UK), making it a monolithic construct.
After confirming satisfactory alignment and stability, clinically and with intraoperative radiographs, wounds were washed with five litres of chlorhexidine. Closure was achieved with loop PDS for the fascia, absorbable Vicryl sutures for the subcutaneous layer and absorbable Monocryl suture for skin. A Mepilex dressing with wool and crepe bandaging was applied. Full weight bearing was allowed post-operatively.
Discussion
Fracture fixation in an osteoporotic bone can be a surgical challenge. Failure of fixation and delayed fracture healing are recognized complications [2,5]. Bone allografts and bone supplements have been used with excellent results in hip and knee revision arthroplasty procedures, peri-prosthetic fractures, avascular necrosis, tumour surgery, non-union of fractures and in spine surgery [6-12]. However, the use of strut grafts for a hybrid plate/structural allograft construct (PAC) for primary or failed internal fixation of long bone fractures in elderly patients with osteoporosis hasn’t really been explored.
Elbarbary, et al. showed that intramedullary nailing in femoral shaft fractures in osteoporotic bones has a good outcome with no major complications [13]. This was the first line of treatment offered to our patient when she initially presented with a fracture of her distal femoral shaft.
We describe a technique to achieve a stable monolithic construct for failed internal fixation of a fracture or even for primary fixation of a fracture in an osteoporotic bone. We augmented the extra medullary locking plate fixation with an inlay intramedullary and an onlay extramedullary strut graft. The intramedullary strut graft was transfixed to the plate and the native femur with four cortical screws and the extra medullary strut graft was anchored to the native bone and the plate with the help of locking cables. Excellent and stable hybrid construct was achieved, enabling the patient to fully weight bear immediately post-operatively. Hybrid fixation with a locking plate and a strut allograft construct (PAC) achieves an enhanced axial and torsional stability, much higher than what would be achieved with a locking plate alone [7,14,15].
Hybrid fixation with Plate Allograft Construct (PAC) is ideal for elderly patients with osteoporotic long bone fractures. This technique is simple and can be performed with relative ease, with no significant addition to the surgical time.
Conclusion
With the growing elderly population, surgical techniques that can achieve a reliable fracture fixation in osteoporotic bones and allow early full weight bearing are welcome. Whilst locking plate and an intramedullary nail are good implants to treat these complex fractures, protected weight bearing or even partial weight bearing may still be required. There is the added risk of failure of fixation. Hybrid fixation with a Plate Allograft Construct (PAC) may provide a much more robust fixation with the added benefit of full weight bearing post operatively.
Author Contributions
Both authors have contributed to the writing of the article, revision and editing, and have participated in the case. Authors have read and approved the final manuscript for submission.
References
- Yaacobi E, Sanchez D, Maniar H, et al. (2017) Surgical treatment of osteoporotic fractures: An update on the principles of management. Injury 48: S34-S40.
- Gorter EA, Reinders CR, Krijnen P, et al. (2021) The effect of osteoporosis and its treatment on fracture healing a systematic review of animal and clinical studies. Bone Rep 15: 101117.
- Giannoudis P, Tzioupis C, Almalki T, et al. (2007) Fracture healing in osteoporotic fractures: Is it really different?: A basic science perspective. Injury 38: S90-S99.
- Nikolaou VS, Efstathopoulos N, Kontakis G, et al. (2009) The influence of osteoporo-sis in femoral fracture healing time. Injury 40: 663-668.
- Hak DJ (2018) The biology of fracture healing in osteoporosis and in the presence of anti-osteoporotic drugs. Injury 49: 1461-1465.
- Delloye C, Cornu O, Druez V, et al. (2007) Bone allografts: What they can offer and what they cannot. J Bone Joint Surg Br 89: 574-579.
- Rollo G, Bonura EM, Huri G, et al. (2020) Standard plating vs. cortical strut and plating for periprosthetic knee fractures: A multicentre experience. Med Glas (Zenica) 17: 170-177.
- Granger L, Bankes MJ, Sandiford NA. (2020) Cortical strut graft for enigmatic thigh pain in uncemented total hip replacement. Cureus 12: e8233.
- Jo YH, Lee SG, Kook I, et al. (2020) Intramedullary fibula strut bone allograft in a periprosthetic humeral shaft fracture with implant loosening after total elbow arthroplasty. Clin Shoulder Elbow 23: 152-155.
- Saltzman BM, Erickson BJ, Harris JD, et al. (2016) Fibular strut graft augmenta-tion for open reduction and internal fixation of proximal humerus fractures: A systematic review and the authors’ preferred surgical technique. Orthop J Sports Med 4: 232596711665682.
- Wang Y, Yin L, Lu Z, et al. (2009) Analysis of long-term outcomes of double-strut bone graft for os-teonecrosis of the femoral head. Orthop Surg 1: 22-27.
- Majoor BCJ, Peeters Boef MJM, van de Sande MAJ, et al. (2017) What is the role of allogeneic cortical strut grafts in the treatment of fibrous dysplasia of the proximal femur? Clin Orthop Relat Res 475: 786-795.
- Elbarbary AN, Hassen S, Badr IT (2021) Outcome of intramedullary nail for fixation of osteoporotic femoral shaft fractures in the elderly above 60. Injury 52: 602-605.
- Rollo G, Biserni M, Huri G, et al. (2020) Strut graft vs. traditional plating in the management of periprosthetic humeral fractures: A multicentric cohort study. Med Glas (Zenica) 17: 490-497.
- Peters CL, Bachus KN, Davitt JS (2003) Fixation of periprosthetic femur fractures: A biomechanical analysis comparing cortical strut allograft plates and conventional metal plates. Orthopedics 26: 695-699.
Corresponding Author
Vatsal Khetan, Senior Clinical Fellow, Trauma and Orthopaedics, Rotherham District General Hospital, The Rotherham NHS Foundation Trust, Moorgate Road, Rotherham S60 2UD, South Yorkshire, United Kingdom
Copyright
© 2022 Khetan V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.