Percutaneous Femoral Derotation Osteotomy - Description of a Novel Technique Using Computer Navigation, Intramedullary Saw and Cephalomedullary Nail
Abstract
Developmental Dysplasia of the Hip (DDH) is known to cause Excessive Proximal Femoral Torsion (EPFT). EPFT can be treated with a Proximal Femoral Derotation Osteotomy (PFDRO) with good success, which is usually performed via closed versus open osteotomy and intramedullary nailing. The technique to measure the degree of correction involves referencing wires or pins placed in the proximal and distal segments prior to the osteotomy, respectively. A goniometer is then used to measure the change in angle between the two wires following osteotomy. Computer navigation has been used to improve iatrogenic malrotations during closed intramedullary nailing in femoral shaft fractures; however, this technology has not yet been applied to correcting idiopathic EPFT via PFDRO. We present the first case of EPFT treated with the combination of an intra-medullary osteotomy, computer navigation guided de-rotation and stabilization with a cephalomedullary device.
Keywords
Computer navigation, Proximal femoral derotation osteotomy
Introduction
Developmental Dysplasia of the Hip (DDH) is known to cause multiple anatomical deformities around the hip joint. One such morphological variation of residual DDH in an adult is Excessive Proximal Femoral Torsion (EPFT). EPFT can be treated with a Proximal Femoral Derotation Osteotomy (PFDRO) with good success [1]. Of note, this condition is commonly associated with degeneration of the hip joint which is oftentimes addressed with procedures ranging from hip arthroscopy to acetabular osteotomy [2,3]. The surgical technique most widely performed for PFDRO involves a closed versus open osteotomy and intramedullary nailing [1,4,5]. The technique to measure the degree of correction involves referencing wires or pins placed in the proximal and distal segments prior to the osteotomy, respectively. A goniometer is then used to measure the change in angle between the two wires following osteotomy [1,3].
Recently, computer navigation has been used to improve iatrogenic malrotations during closed intramedullary nailing in femoral shaft fractures as it allows for measurement of femoral neck anteversion using intra-operative fluoroscopy referenced off the posterior femoral condylar axis. To our knowledge, this technology has not yet been applied to correcting idiopathic EPFT via PFDRO. We present the first case of EPFT treated with the combination of an intra-medullary osteotomy, computer navigation guided de-rotation and stabilization with a cephalomedullary device. These three techniques have been previously described and used separately, but never together in the same procedure.
Case Report
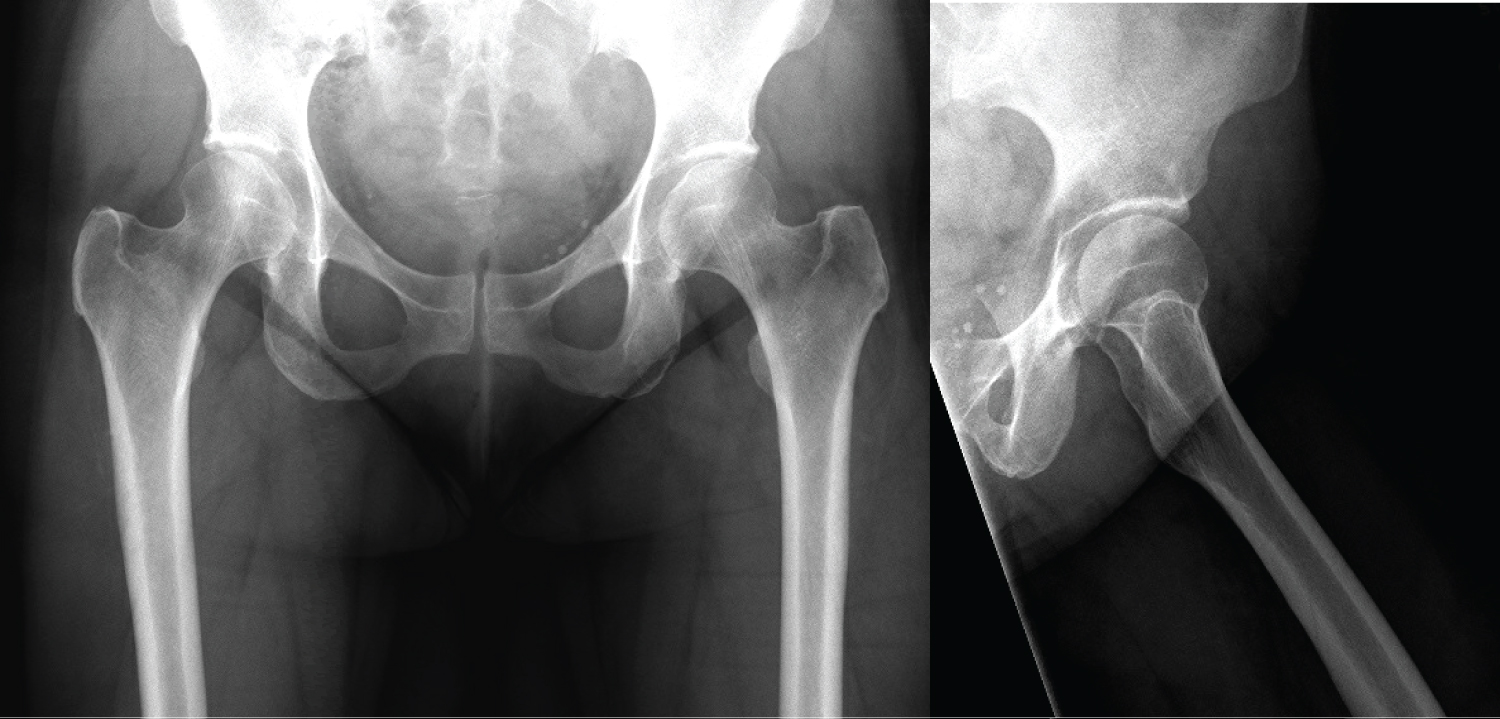
A 47-year-old woman was referred to our tertiary hospital with severe left hip pain without discernable osteoarthritis in her hip and no evidence of referred pain from elsewhere. She was known to have DDH as a child and was treated then with a spica cast and pavlik harness. At the time of the initial visit the patient complained of pain located in her lateral and anterior thigh, with occasional pain radiating to her groin and buttocks. She also had a bothersome in-toeing gait on the left side. Her musculoskeletal exam demonstrated that she was able to flex her hip to about 120 degrees bilaterally, abduct 50 degrees on the right, and 40 degrees on the left. She had external rotation to 45 degrees on the right and 40 degrees on the left. Her internal rotation was 30 degrees on the right and 20 degrees on the left. She had intact neurologic function and no evidence of vascular deficiency.
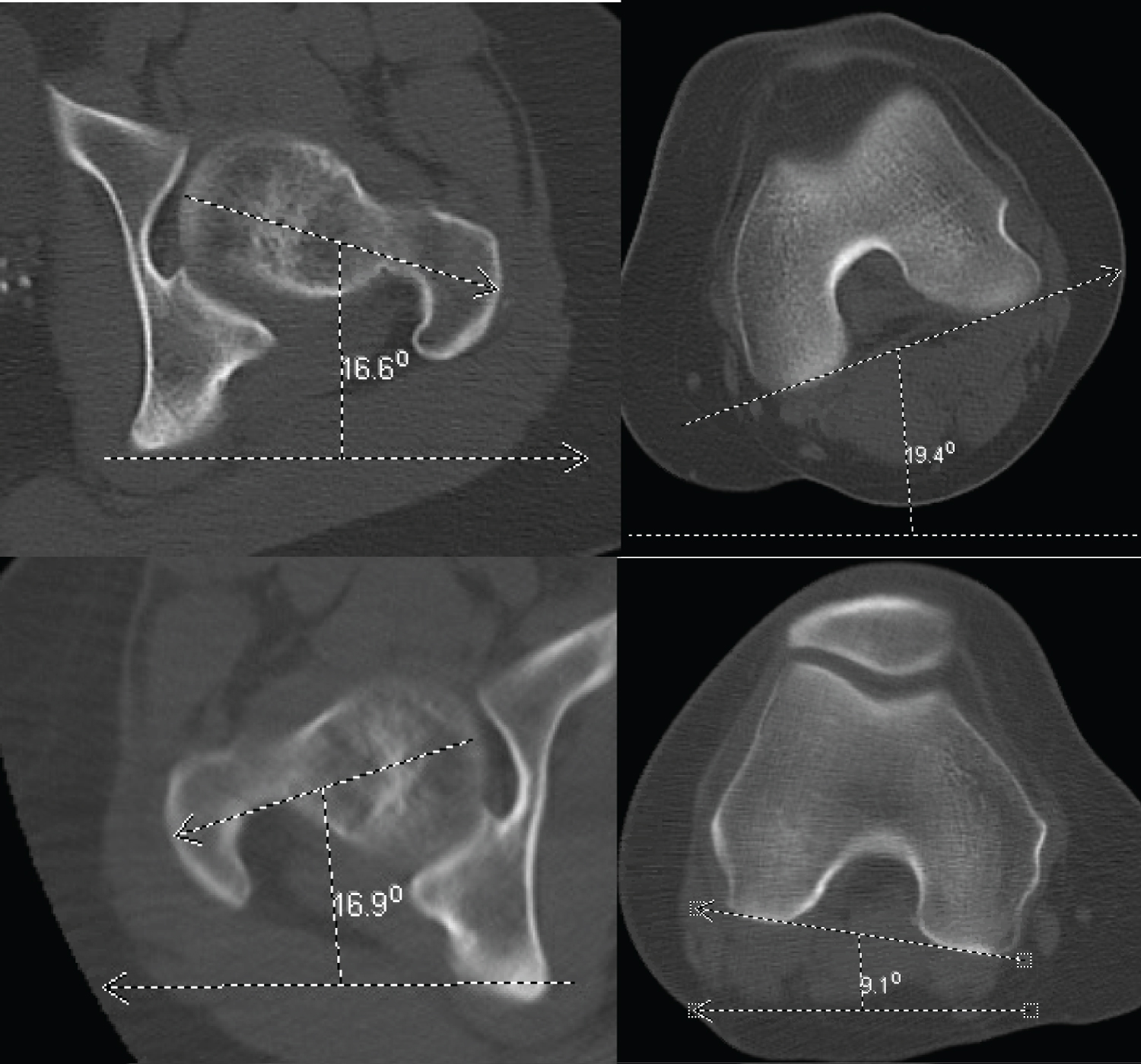
Preoperative imaging included plain radiographs (Figure 1) and a CT scan, which demonstrated 36 degrees of femoral anteversion on the left and 26 degrees on the right (Figure 2). She was consequently diagnosed with EPFT and offered a PFRDO. She also had a recent prior MRI of the pelvis which did not demonstrate any abnormalities involving the hip joint. Digital pre-operative templating was performed with Trauma-CAD (Voyant Health, Columbia, MD, USA) to determine the level of osteotomy in relation to the Cephalomedullary nail, so that there was at least two cortical widths between the osteotomy and the distal locking screw of the nail [6]. The procedure was rehearsed two weeks prior on synthentic bones (Sawbones™, Vashon, Washington, USA).
Intraoperatively, she was positioned supine on a Pro-FX table (Mizuho OSI, Union City, CA, USA) with her non-operative leg abducted, flexed and externally rotated in a Lloyd Davis stirrup and with a calf pump for thromboprohylaxis. The left foot was placed in a boot and attached to the spar of the Pro-FX table such that the leg was extended at the hip and knee. She was positioned in a 'banana' position, convexity to the left, to aid instrumenting the femur.
Scout films with a C-arm fluoroscope were taken to make sure that there were no impediments to image acquisition.
Step 1: Distal femoral condyles rotated to horizontal
The lateral view of the distal femur was taken with the C-arm in a horizontal position. The limb was rotated until the posterior femoral condyles overlapped perfectly and the spar was locked in this position until the osteotomy. The left lower extremity was then prepped and draped in standard sterile fashion.
Step 2: Reaming and insertion of cephalomedulalry nail in intact femur
A 3.5 mm straight pin was placed percutaneously to the tip of the greater trochanter, which was opened with a cannulated bone awl passed over the wire. A ball-tipped guide wire was then inserted into the femur which was sequentially reamed to 13.5 mm up to its diaphysis. The proximal femur was reamed to 17 mm. A short (180 mm) cephalomedullary nail (Gamma Nail, Stryker, Mawah, NJ, USA) with a 130-degree neck angle was inserted into the canal.
Step 3: Insertion of Navigation trackers to femur
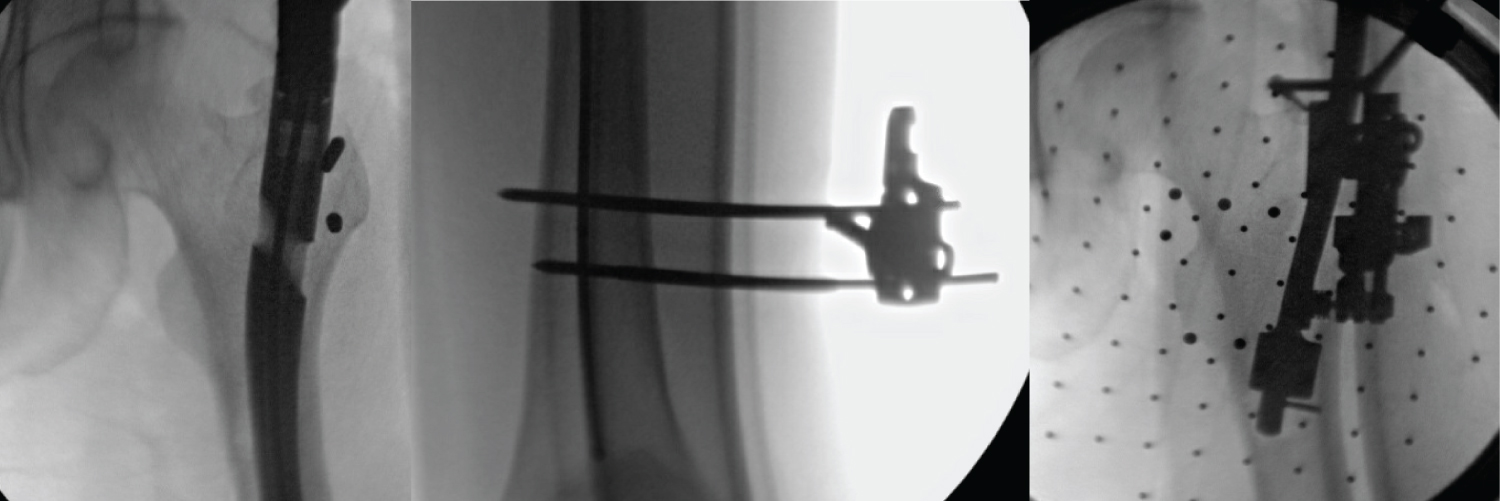
Two threaded pins (3 mm) were then inserted into the greater trochanter lateral to the Gamma nail to which the proximal navigation tracker was attached. These were inserted after the cephalomedullary nail in order to ensure they did not impede the trajectory of the nail. Two (4 mm) navigation pins were inserted in the distal femur bi-cortically (Figure 3).
Step 4: Fluoroscopic registration of the femur
The Brain lab Navigation system (Munich, Germany) was used for this operation. A C-arm tracker was attached to the receiver end of the machine. The nail was then removed, and five fluoroscopic radiographs were then taken: AP and lateral of the proximal femur, AP and lateral of the proposed osteotomy site, and a true lateral of the distal femur with overlapping condyles. These images were used to aid the identification and selection of the femoral head center, the posterior condylar axis, and the axis of the proximal and distal “virtual” fragments. Her intraoperative rotational alignment was recorded with computer navigation as being 33 deg. Of note, pre-operative CT scan had measured the anteversion as being 36 deg).
Step 5: Intramedullary osteotomy
A 13 mm Cam with a 16 mm saw was attached to the intramedullary saw (Biomet, Warsaw, IN, USA) which was then inserted into the proximal femur to the pre-designated level. This gave a maximum cutting diameter of 39 mm (13 mm diameter of the CAM + 16 mm length of saw). A circumferential horizontal intramedullary osteotomy was then preformed. The completeness of the osteotomy was confirmed with both fluoroscopic images and with two 5 mm Steinman pins inserted into the proximal and distal fragments, respectively, which upon completion of the osteotomy, became independently mobile.
Step 6: Re-insertion of the nail and de-rotation under navigation
The Gamma nail was re-inserted to its pre-determined depth, and the proximal cephalad screw inserted using the 'One shot' device (Stryker, Marwah, NJ, USA) along with a set screw to lock the cephalad screw in place. Next, rotational correction was made in real-time using the computer navigation, changing the femoral anteversion from 33 degrees to 15 degrees, by externally rotating the foot on the Pro-FX spar. A distal locking screw was then inserted using the attached external jig. Finally, the correction was crosschecked under fluoroscopic guidance by first acquiring a true lateral of the distal femoral condyles. The degree of C-arm rollover was then noted at this position. A lateral of the femoral neck was then subsequently obtained. The difference in necessary C-arm rollover to obtain this image represents the version, which was confirmed to be 15 degrees of anteversion.
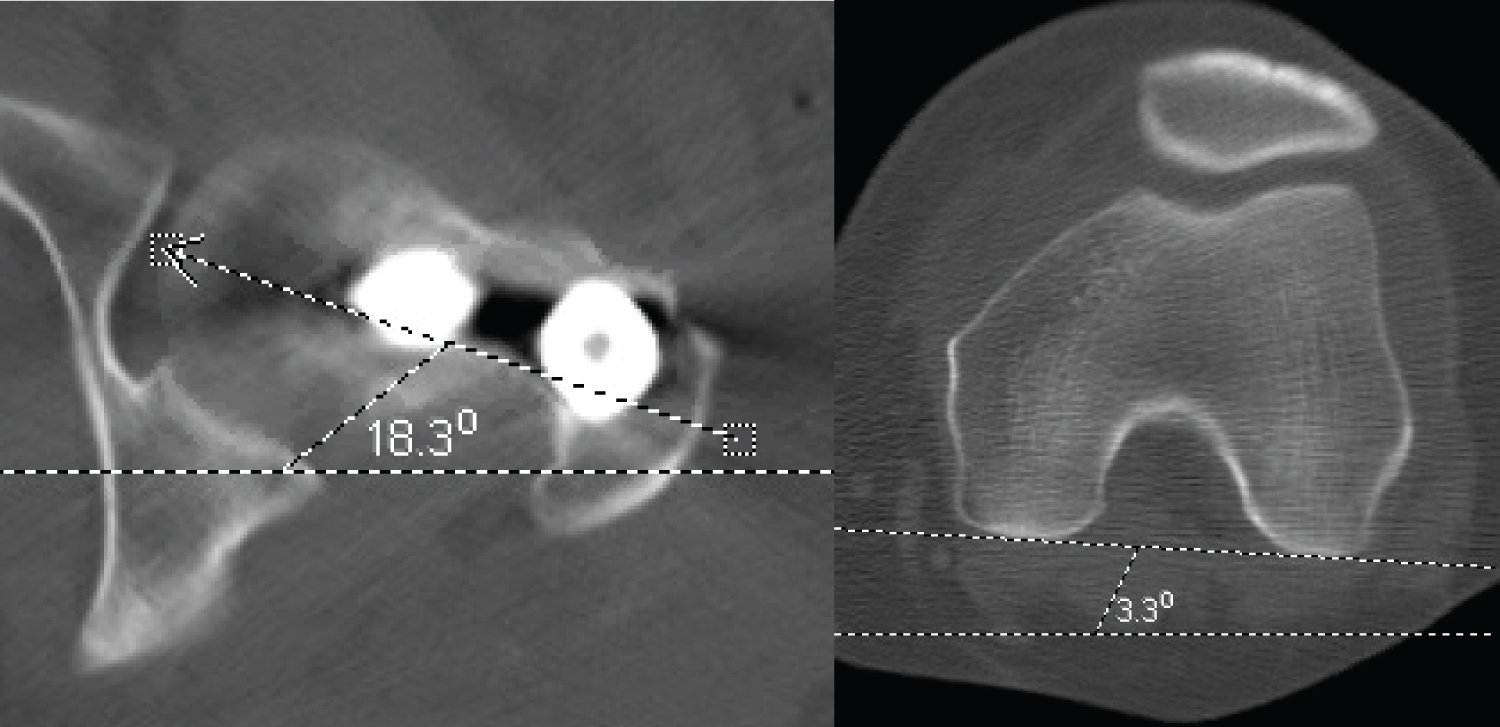
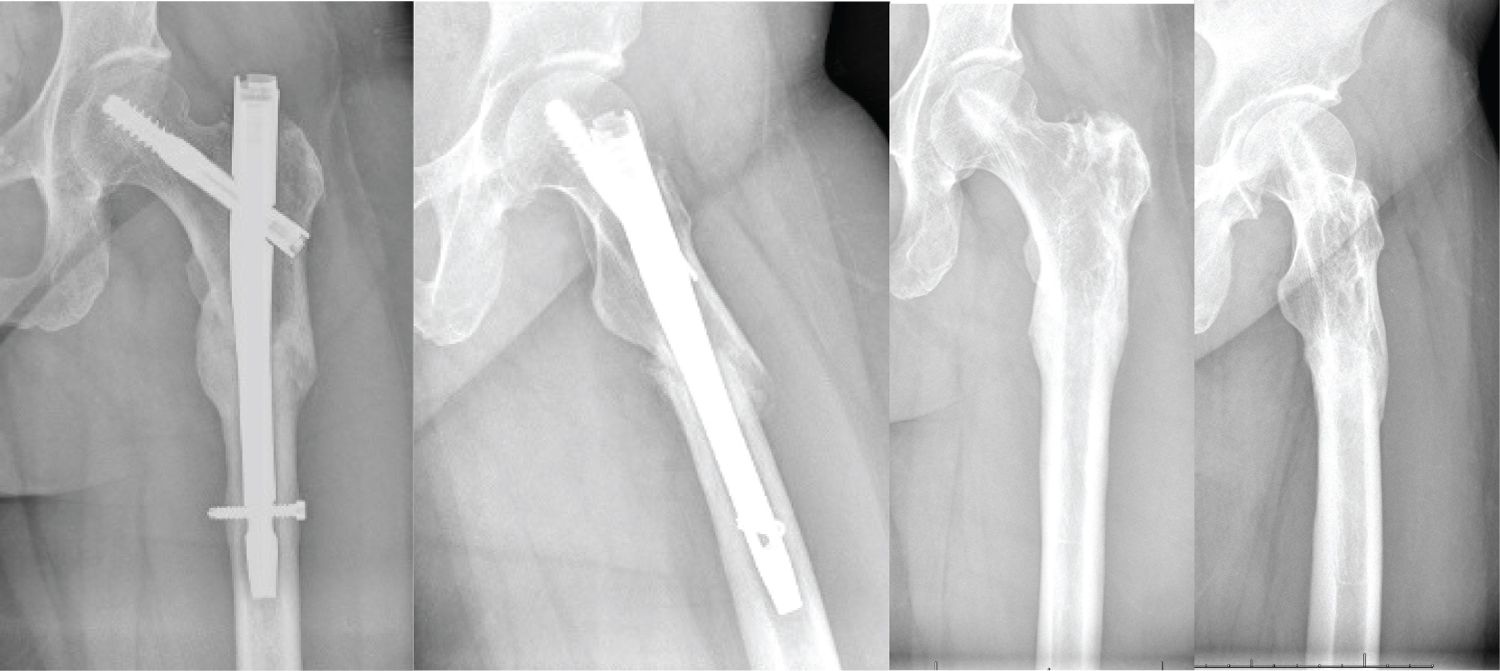
In addition, a postoperative CT scan was obtained, which also confirmed the new anteversion to be 15 degrees (Figure 4). Post-operatively, the patient was permitted to weight bear as tolerated. Her subsequent hospital stay was uneventful, and she was discharged to home on post-operative day two. Her osteotomy site had radio graphically healed by her three-month post-operative appointment (Figure 5). At that point, she had resumed full activity without limitations. The nail was removed percutaneously eight months after the index surgery due to lateral hip pain over the region of the greater trochanter, a well described and relatively common issue following the use of a cephalomedullary device [7]. This resulted in complete resolution of her pain. At her one-year follow-up, she reported no pain and an ability to run for the first time since she was a teenager. At final follow-up 27 months post-operatively, she remained pain free without limitations in her activity level.
Discussion
The commonly described technique for PFDROs involves an open approach and using Kirschner wires in the proximal and distal fragments to assess the rotational correction [3]. The open technique has many disadvantages including larger area of soft tissue dissection with more periosteal stripping, disruption of the osteotomy-site hematoma, and increased risk for wound complications, infection, delayed union, and nonunion [8-10]. The usual method of measuring the correction also allows for an element of human error in evaluating the angles. Additionally, in our experience, soft tissue tension on the Kirschner wires can often-times result in bending of the wires, producing a less reliable measurement. Finally, the rotation of the proximal fragment is likely to happen at the femoral head in the hip joint rather than along the anatomic axis of the proximal femur. These factors can result in an unreliable correction.
Computer navigation is used most frequently in hip and knee arthroplasty to accurately position components. It has also been used in deformity correction surgery as it allows for precise measurement of long bone axial and rotational alignment. The most common application for the latter indication is improvement of iatrogenic rotational malunions following closed femoral shaft intramedullary nailing [11].
The use of an intra-medullary saw is attractive as it avoids the surgical exposure of the bone and preserves the 'fracture' hematoma which is useful for bone healing. These saws have been most commonly used for rotational malunions of the femur and shortening osteotomies [3,10,12]. The use of an intramedullary nail was able to allow her to fully weight bear as tolerated immediately which helped shorten her rehabilitation period.
The most notable challenge of this case was placing the navigation pins into the proximal femur with the nail in-situ. With limited options, the most readily available bone is in the greater trochanter. Caution must be taken during the procedure to avoid placing excess stress on these pins in order to prevent an iatrogenic fracture of the greater trochanter.
This case also reinforces the importance of pre-operative planning. The amount of desired correction, position of the osteotomy site in relation to the nail, and the size of the cutting diameter of the intra-medullary saw were determined pre-operatively. Rehearsing the technique on Sawbones proved to be invaluable in ensuring the operative was carried out safely and efficiently.
This is the first reported case of a minimal access PFDRO using an intramedullary saw, cephalomedullary nail and computer navigation for precise correction of femoral version. We are extremely enthusiastic about the results and plan to use it in the future on appropriately indicated patients.
Conflict of Interest
None.
Study Description
Case Presentation, level V evidence.
Disclosures
No funding or other sources of support were used to aid this work. The Authors declare that they have no potential or perceived conflicts of interest.
References
- Buly RL, Sosa BR, Poultsides LA, et al. (2018) Femoral derotation osteotomy in adults for version abnormalities. J Am AcadOrthop Surg 26: e416-e425.
- Waisbrod G, Schiebel F, Beck M (2017) Abnormal femoral antetorsion-a subtrochanteric deformity. J Hip Preserv Surg 4: 153-158.
- Hartigan DE, Perets I, Walsh JP, et al. (2017) Femoral derotation osteotomy technique for excessive femoral anteversion. Arthrosc Tech 6: e1405-e1410.
- Chapman ME, Duwelius PJ, Bray TJ, et al. (1993) Closed intramedullary femoral osteotomy: Shortening and derotation procedures. Clin Orthop Relat Res 287: 245-251.
- Winquist RA (1986) Closed intramedullary osteotomies of the femur. Clin Orthop Relat Res 212: 155-164.
- Antekeier SB, Burden RL, Voor MJ, Roberts CS (2005) Mechanical Study of the Safe Distance Between Distal Femoral Fracture Site and Distal Locking Screws in Antegrade Intramedullary Nailing. J Orthop Trauma 19: 693-697.
- Rosen M, Kasik C, Swords M (2020) Management of Lateral Thigh Pain following Cephalomedullary Nail: A Technical Note. Spartan Med Res J 5: 12931.
- Itoman M, Sekiguchi M, Yokoyama K, Minamisawa I (1996) Closed intramedullary osteotomy for rotational deformity after long bone fractures. Int Orthop 20: 346-349.
- Grosse D, Brinkert D, Kempf I (2002) Osteotomies of the femoral diaphysis by closed technique. In: Kempf I, Leung KS, Grosse A, et al., Practice of intramedullary locked nails: Advanced techniques and special applications recommended by “Association Internationale Pour l’Ostéosynth Èse Dynamique” (AIOD). Springer 2002: 73-81.
- Stahl JP, Alt V, Kraus R, et al. (2006) Derotation of post-traumatic femoral deformities by closed intramedullary sawing. Injury 37: 145-151.
- Keast Butler O, Lutz MJ, Angelini M, et al. (2012) Computer navigation in the reduction and fixation of femoral shaft fractures: A randomized control study. Injury 43: 749-756.
- Blair VP, Schoenecker PL, Sheridan JJ, et al. (1989) Closed shortening of the femur. J Bone Joint Surg Am 71: 1440-1447.
Corresponding Author
Wyatt Vander Voort, MD, Department of Orthopaedics, University of California, Davis 2315 Stockton Blvd Sacramento, CA 95817, USA, Tel: 719-641-4278
Copyright
© 2022 Voort WDV, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.