Assessment of Clinical and Functional Outcomes of Treating Clinically Diagnosed Plica Syndrome in a Pediatric Population
Abstract
Introduction: Knee pain is one of the most common complaints in pediatric clinics, accounting for nearly one third of visits. Plica syndrome is one cause of pediatric knee pain that typically results from a traumatic event or due to overuse. Synovial plicae are normal anatomic findings thought to be embryologic remnants from the three compartments that develop into the knee. Plicae are associated with knee pain caused by trauma or repetitive movements that lead to inflammation; most commonly the medial plica. The purpose of this study is to retrospectively review plica syndrome treated operatively at a single institution by multiple surgeons.
Methods: A retrospective study of pediatric patients treated operatively for symptomatic plica syndrome at a tertiary care center between 2004 and 2020 was conducted. Patients were included if less than 18 years of age and underwent plica excision for the diagnosis of symptomatic plica syndrome. Patients were excluded if also treated for a concurrent injury (ie. ACL tear) or previous knee surgery. Medical records were reviewed for age, gender, clinical presentation, surgical findings, length of follow up, need for additional surgeries, complications, and outcomes.
Results: Eighty-four patients were included in the study. Twenty-four (29%) were male and 60 (71%) were female. Average age at surgery was 14.7 years. Patients had an average length of follow-up of 5.8 months. Fifty-one (60%) patients reported a specific event when their knee pain began. No patients required reoperation for plica syndrome specifically. Three (4%) patients required reoperation on the same knee for OCD lesion (2) and for a hypertrophic scar. Seventy-nine (94%) patients were able to return to play, while 5 (6%) patients had continued pain.
Conclusion: Plica syndrome is a relatively common cause of pediatric knee pain. After failure of conservative treatment, operative treatment should be considered. The results show that operative treatment of plica syndrome provides significant relief in over 94% of patients.
Keywords
Plica syndrome, Pediatrics plica, Operative management, Knee pain
Introduction
Knee pain in the adolescent population is one of the most common chief complaints in office visits; research studies performed in 1995, 2004, and 2017 found that the prevalence of knee pain in their adolescent research populations were 18.5%, 33.6%, and 34.7%, respectively [1-3]. In the adult population, knee pain prevalence has increased by nearly 65% over the past two decades, with one out of every four adults suffering from some degree of knee pain. This translates to almost four million knee pain attributed primary care visits per year [4]. The prevalence of knee pain in adults age 50 years and older doubles to 50% [3].
While the prevalence of knee pain is lower in the pediatric population compared to the adult population, it is an important health issue to address as it can serve as a precursor to debilitating chronic knee pain later in life if not properly treated and managed [5]. In addition to concerns over health care costs, knee-pain in pediatric populations can create both short-term and long-term health concerns if pain levels prevent children and adolescents from engaging in exercise. The CDC reports an 18.5% prevalence of obesity in children and adolescents age 2-19 years [6]. With this broader perspective of the implications of knee pain in the adolescent population and its potential impact in predisposing these patients at an early-age to other detrimental co-morbidities, it is imperative for current research studies to examine the effectiveness of treatment for pediatric knee pain.
There are numerous mechanisms by which chronic knee pain can arise in pediatric populations including congenital predispositions, developmental disorders, or traumatic injuries. A common under lying cause of chronic knee pain in adolescents, particularly with young athletes, are overuse injuries [7]. The stress on a knee joint as a result of overuse can cause a variety of different disorders associated with chronic knee pain, one of which is called plica syndrome. Plica syndrome is characterized by chronic medial or anterior knee pain that becomes worse with exercise or prolonged sitting. The clinical diagnosis of plica syndrome is made upon clinical features such as a palpable, tender plica, clicking or popping sensation, and exclusion of other causes of knee pain [8].
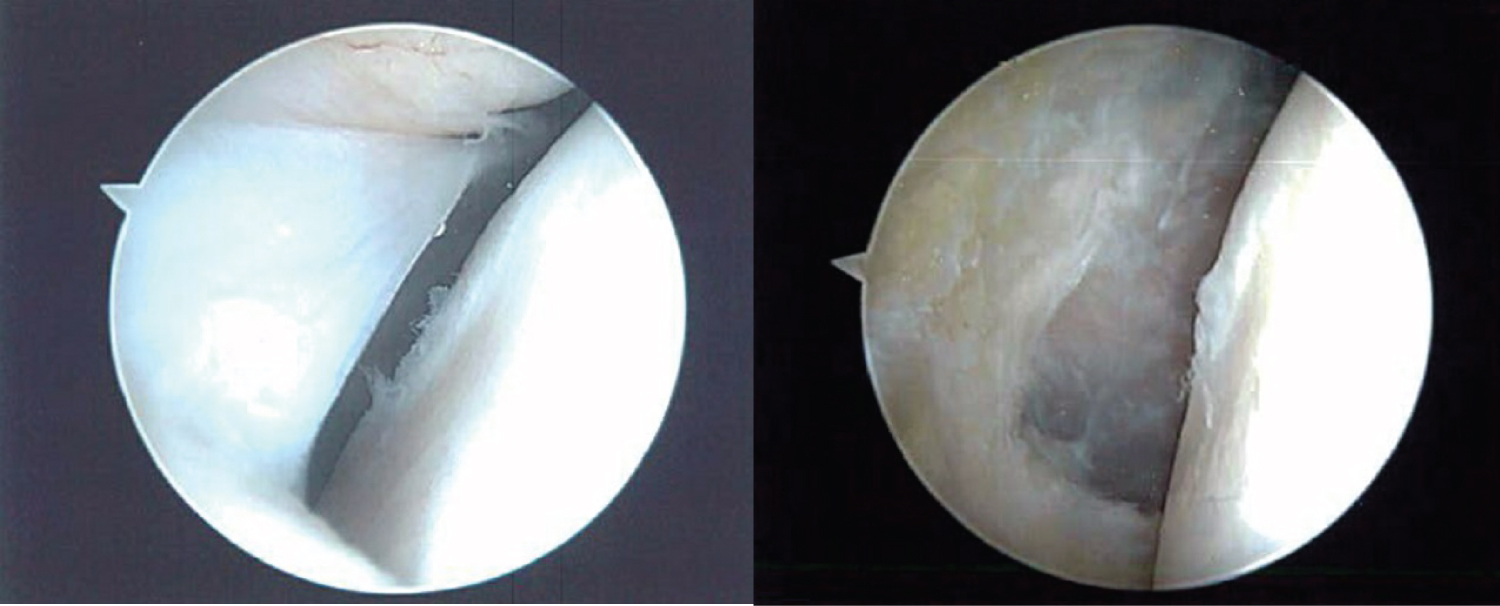
During embryological development of the knee, mesenchymal condensations and cavities within the inter zone tissue begin to form during weeks seven through ten; beyond this point, a single cavity with synovial lining comprises the knee joint with mesenchymal tissue found in the four distinct regions of the knee joint: Suprapatellar, medial, infrapatellar, and lateral [8,9]. There are synovial septa that resorb over the following 2 weeks. When these septa fail to resorb and are large enough, they are considered plicae (Figure 1). With direct trauma or overuse of the knee joint, plicae can become compressed, undergo fibrosis, and become inflamed [10]. In addition, any knee condition that causes synovit is can lead to the development of a pathological plica [8].
The presence of synovial plica has been reported as high as 70% in the population and the prevalence of symptomatic plica syndrome is reported as approximately 10% [8,10]. However, this number may be an underestimate as the diagnosis is typically made clinically and the symptoms of plica syndrome are similar to those of other etiological conditions [11,12].
The treatment for plica syndrome generally recommends an acute and recovering phase as part of a conservative, non-operational approach. The acute phase includes reduction of physical activity, nonsteroidal anti-inflammatory drugs, ice application, and potentially corticosteroid injections to help reduce swelling and pain. When pain levels subside, treatment begins to target stretching and strengthening the surrounding muscle groups crossing the knee joint such as the quadriceps, hamstrings, gastrocnemius, as well as hip adductors [8]. However, for patients with severe symptoms, or when conservative treatment fails, surgical resection of the pathological plica is recommended and shows positive results in significantly reducing pain levels [10,13].
Despite current evidence-based research demonstrating the effectiveness of surgical intervention to reduce pain levels in patients suffering from plica syndrome, there is still limited data demonstrating functional outcomes of surgical intervention in the pediatric population outside of a recent 2016 research study published in the Journal of Children's Orthopedics. The 2016 study showed promising results; however, a large majority of their surgical results involved plica excision with a lateral retinacular release [10]. Thus, more research is needed to be conducted on the clinical and functional outcomes of treating plica syndrome in a pediatric population through arthroscopic resection of pathological plica. We hypothesize that arthroscopic resection of pathological plica will yield positive results in enabling patients to return to their respective physical activities of choice.
Methods
This study was approved by the health system Institutional Review Board (IRB). A retrospective review was performed for pediatric patients aged less than 18 years treated operatively for symptomatic plica syndrome between 2004 and 2020 at a single institution. Operative treatment consisted of surgical resection of the pathological plica. Patients were identified by and aggregated from the institution's electronic health record, EPIC, and using a password protected query program and database, called Webi.
CPT code for knee arthroscopic synovectomy was used to identify 539 patients. Patient medical records were retrospectively reviewed to identify patients treated with a primary diagnosis of pathological plica. Exclusion criteria were patients 18 years or older, treated for a concurrent injury (ie. ACL tear) and previous ipsilateral knee surgery.
Eighty-four patients were included in the study. Patient medical records were reviewed, including pre-surgical clinic notes, operative notes, and post-surgery clinic notes. Data collection included age, gender, clinical presentation, surgical findings, length of follow-up, need for additional surgeries, complications, and return to play.
Results
Eighty-four patients met the inclusion criteria for this study. Sixty (71%) patients were female, 24 (29%) patients were male, and the average patient age was 14.7 years (range 10-17). Fifty-one (61%) patients had an associated traumatic event that correlates with the start of their knee pain and 33 (39%) patients had a more insidious onset. All patients failed at least 6 months of conservative treatment and had evidence of plica on physical exam and/or MRI. The average length of follow up was three visits (range 1-10) and 5.8 months (range 1-58.7).
Seventy-nine (94%) patients experienced improved symptoms and were able to return to play within the time of their follow up. Five (6%) patients continued to have pain and were unable to return to play. One patient was noncompliant with post-operative instructions and injured their knee while running stairs. No patients underwent additional surgery for re-operation specifically for plica. Two patients went on to have additional surgery for OCD lesions and one patient required surgical removal of hypertrophic scar tissue.
Five (6%) patients had an associated OCD lesion that was addressed during surgery. Five (6%) patients had meniscal tears and one patient had evidence of a healed meniscal tear. Three (4%) patients experienced minor complications from surgery, including a hemarthrosis that required aspiration, uncontrolled pain and need for emergency room visit, and emergency room visit for skin discoloration and numbness. All issues resolved within one week. No major complications were noted.
Discussion
This study reports on a pediatric population treated operatively for symptomatic plica syndrome. The average age at surgery was 14.7 years. In total, 71% of patients were female, which is likely due to the higher rate of anterior knee pain in females. Sixty-one percent of patients reported a specific traumatic event triggering the onset of symptoms. This finding is similar to a 2013 meta-analysis on plica syndrome in which 57% of cases had a known traumatic onset of injury [12]. The average length of follow-up was 5.7 months. We found no patients required reoperation for plica syndrome; however, three patients required an additional operation on the same knee for other pathologies. Seventy-nine (94%) patients reported improved symptoms and were able to return to play, and only four patients continued to report knee pain that prevented them from returning to play.
While the results showed good return to play outcomes, conservative treatment remains first line. Previous studies have reported a 60% success rate for non-operative treatment, although these are adult study populations. While other studies have proven conservative treatment as effective, these protocols typically work best for patients with early or mild disease [8]. For patients with more severe disease or who have failed conservative protocols, surgery has been shown to be effective in both reducing pain levels and allowing patients to return to physical activity [8,12]. In a similar study, Kosaka, et al. reported the clinical outcomes of 10 athletes with an average age of 19 years with symptomatic lateral plicae who underwent arthroscopic resection. They reported that pain and range of motion were improved in all cases with no complications [14]. Although evidence suggests arthroscopic resection is a good option for symptomatic synovial plicae unresponsive to conservative treatment, there is a lack of research reporting outcomes of surgical plica excision in pediatric populations, which highlights the importance of this study.
A strong aspect of this study was the young age of patients as many prior studies evaluated older age groups. Limitations of the study include its retrospective nature at a single institution, short term follow up, limited pre and postoperative functional data, and small study population. Further research into the long-term outcome of pediatric patients operated on for plica syndrome is needed.
In conclusion, this study demonstrates arthroscopic plica excision is an effective means of treating plica syndrome in the pediatric population with a relatively low risk for complications and a high rate of return to play. Further prospective research in long-term outcomes of patients treated for plica syndrome compared to non-operative treatment should be carried out. Given the results of this study, we recommend surgical intervention be considered as an effective treatment option for pediatric patients diagnosed with plica syndrome who do not improve with non operative treatment.
References
- Vahasarja V (1995) Prevalence of chronic knee pain in children and adolescents in northern Finland. Acta Pædiatrica 84: 803-805.
- Spahn G, Schiele R, Langlotz A, et al. (2004) Prevalence of functional pain of the back, the hip and the knee in adolescents: Results of a cross-sectional study. Dtsch Medizinische Wochenschrift 129: 2285-2290.
- Saes MO, Soares MCF (2017) Knee pain in adolescents: Prevalence, risk factors, and functional impairment. Brazilian J Phys Ther 21: 7-14.
- Bunt CW, Jonas CE, Chang JG (2018) Knee pain in adults and adolescents: The initial evaluation. Am Fam Physician 98: 576-585.
- Lyu SR, Hsu CC (2006) Medial plicae and degeneration of the medial femoral condyle. Arthrosc - J Arthrosc Relat Surg 22: 17-26.
- Hales CM, Carroll MD, Fryar CD, et al. (2017) Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief 288: 1-8.
- Patel DR, Villalobos A (2017) Evaluation and management of knee pain in young athletes: Overuse injuries of the knee. Transl Pediatr 6: 190-198.
- Lee P, Nixion A, Chandratreya A, et al. (2017) synovial plica syndrome of the knee: A commonly overlooked cause of anterior knee pain. Surg J 3: e9-e16.
- Boles CA, Martin DF (2001) Synovial plicae in the knee. Am J Roentgenol 177: 221-227.
- Kramer DE, Kalish LA, Abola MV, et al. (2016) The effects of medial synovial plica excision with and without lateral retinacular release on adolescents with anterior knee pain. J Child Orthop 10: 155-162.
- Bellary SS, Lynch G, Housman B, et al. (2012) Medial plica syndrome: A review of the literature. Clin Anat 25: 423-428.
- Schindler OS (2014) "The Sneaky Plica" revisited: Morphology, pathophysiology and treatment of synovial plicae of the knee. Knee Surgery, Sport Traumatol Arthrosc 22: 247-262.
- Uysal M, Asik M, Akpinar S, et al. (2008) Arthroscopic treatment of symptomatic type D medial plica. Int Orthop 32: 799-804.
- Kosaka M, Nakase J, Kitaoka K, et al. (2019) Arthroscopic treatment of symptomatic lateral synovial plica of the knee. J Orthop Surg 27: 2309499019834496.
Corresponding Author
J Alex Holbert, MD, Geisinger Medical Center, Danville, 16 Woodbine Lane, PA17821, USA.
Copyright
© 2022 Holbert JA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.