Decompression of Thoracic Ossified Ligamentum Flavum with Floating Technique, Intraoperative Neurophysiological Monitoring and 3D Fluoroscopic Navigation
Abstract
Ossification of ligamentum flavum (OLF) is a rare condition. A 62-year-old gentleman, with cord compression by thoracic OLF, was treated with laminectomy. In this paper, an unusual case of thoracic OLF treated by laminectomy with floating ossification, with the incorporation of intraoperative neurophysiological monitoring (IONM) and 3D fluoroscopic navigation, is presented and a review of the literature is described.
Keywords
Floating, Intraoperative neurophysiological monitoring, Laminectomy, Navigation, Ossification of ligamentum Flavum
Introduction
Ossification of ligamentum flavum is an uncommon cause of thoracic myelopathy. Surgical treatment with laminectomy with ossified ligament excision has been shown to be associated with complications such as dural tear and cerebrospinal fluid (CSF) leaks [1]. Decompression of OLF with floating technique has been rarely reported in the current English literature [2-4]. Concomitant applications of IONM and 3D fluoroscopic navigation in the procedure have never been discussed. We report a case of T10-T12 OLF with cord compression treated by laminectomy with floating ossification, under the assistance of IONM and navigation guidance.
Case Report
A 62-year-old gentleman, with history of L2-S1 posterior spinal fusion for lumbar spondylosis years ago, presented with progressive bilateral lower limb numbness and weakness for 3 months. Patient reported poor mobility and become wheelchair bound after symptom onset. Preoperative physical examination showed diffusely diminished light touch and pin prick sensation. The proximal and distal power of both lower limbs were grade 3/5 and 4/5. Hypertonicity and hyperreflexia were demonstrated. He reported no sphincter disturbance with per rectal examination showing preserved anal tone and grip. Overall, he had Frankel Grade C spastic paraparesis and the underlying cause of cord compression had to be sought.
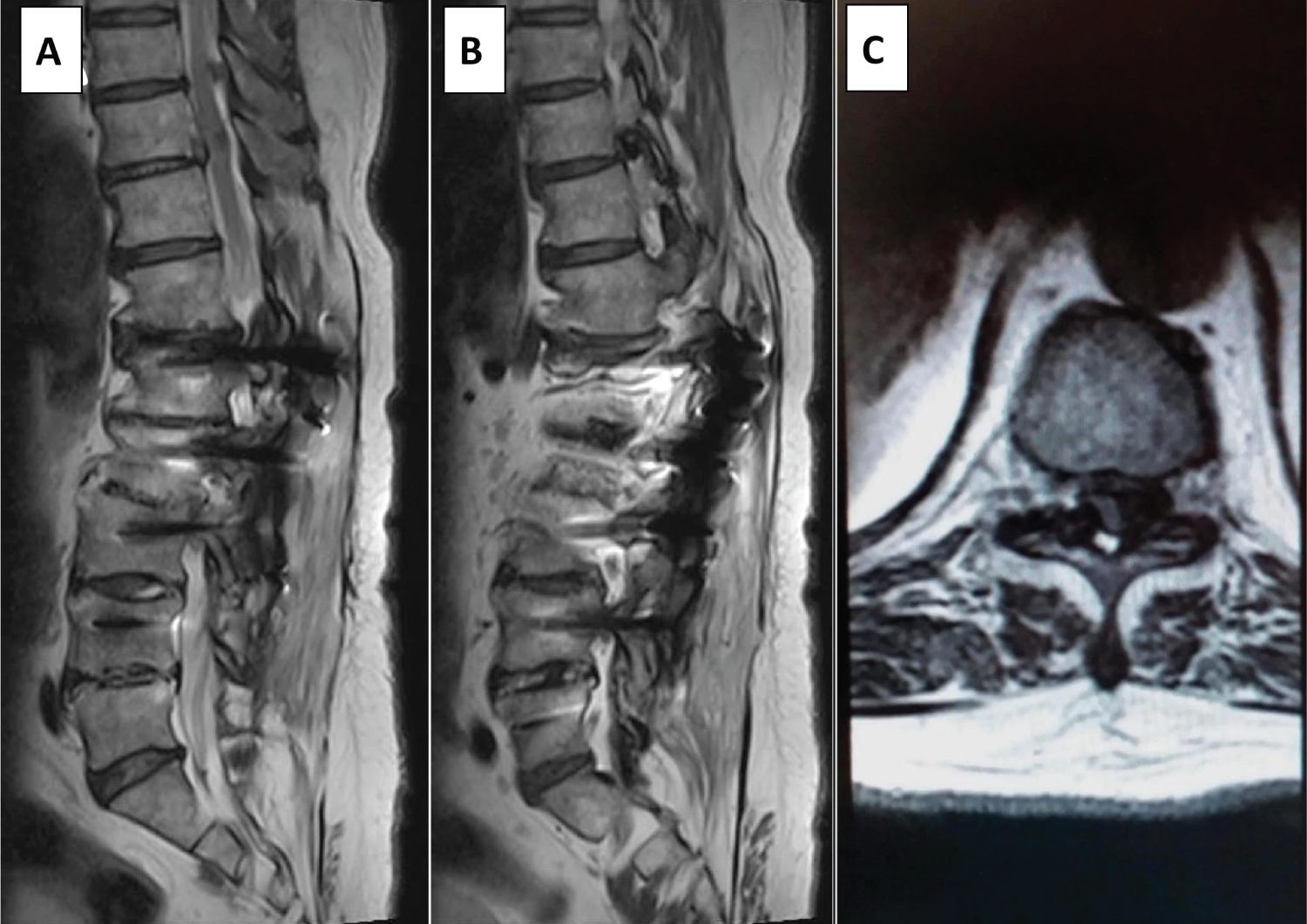
T2W (weighted) MRI of the T and LS spine showed ligamentum flavum hypertrophy at both T10/11 and T11/12 levels, with significant cord compression at T11/12 level. Bilateral lateral recess and neuroforamen were narrowed at the same level (Figure 1). Prior operated levels at L2-S1 only showed mild degenerative changes with no nerve root or cauda equina compression. Extent of ossification was also shown on preoperative CT scan (Figure 2).
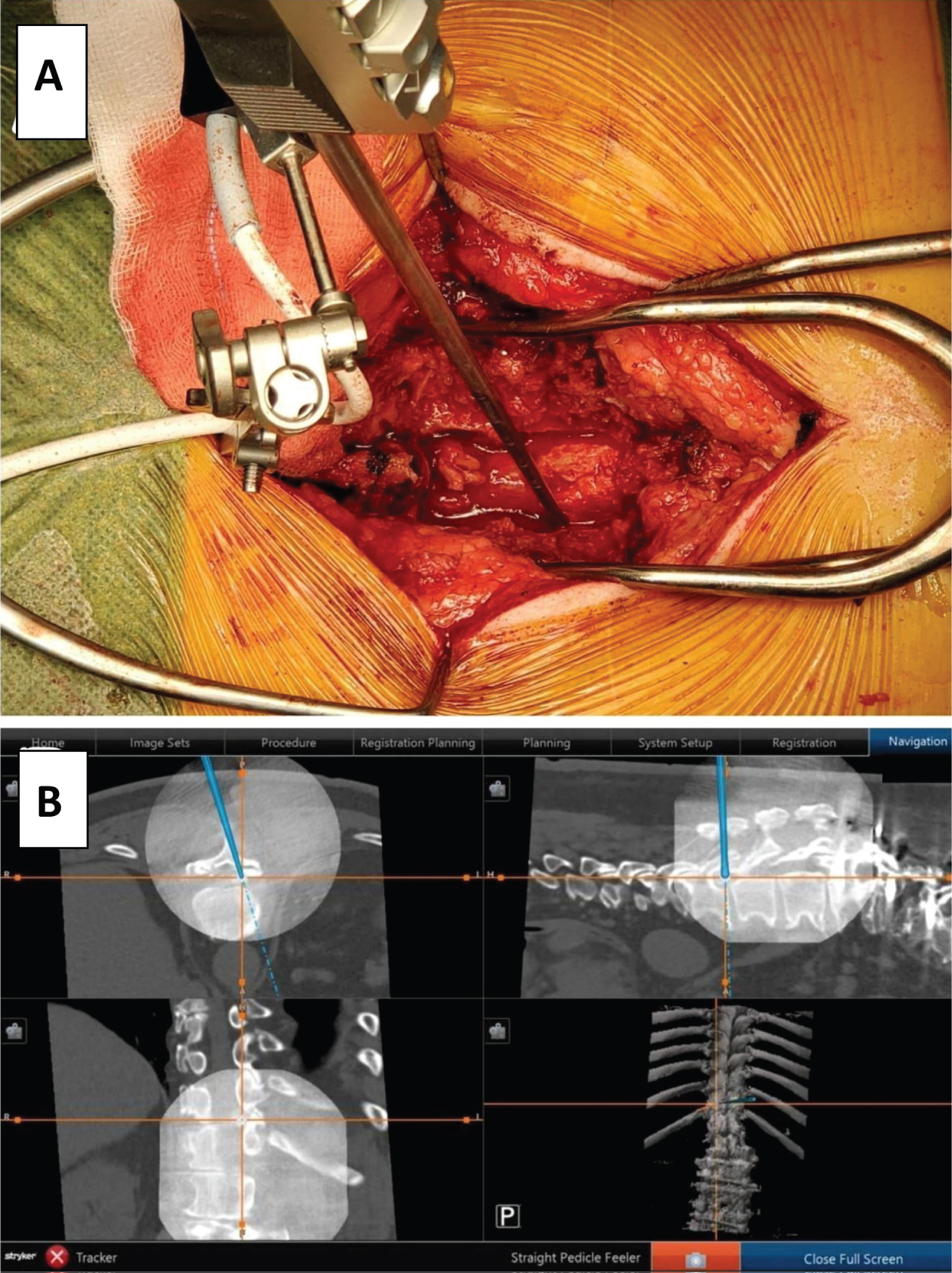
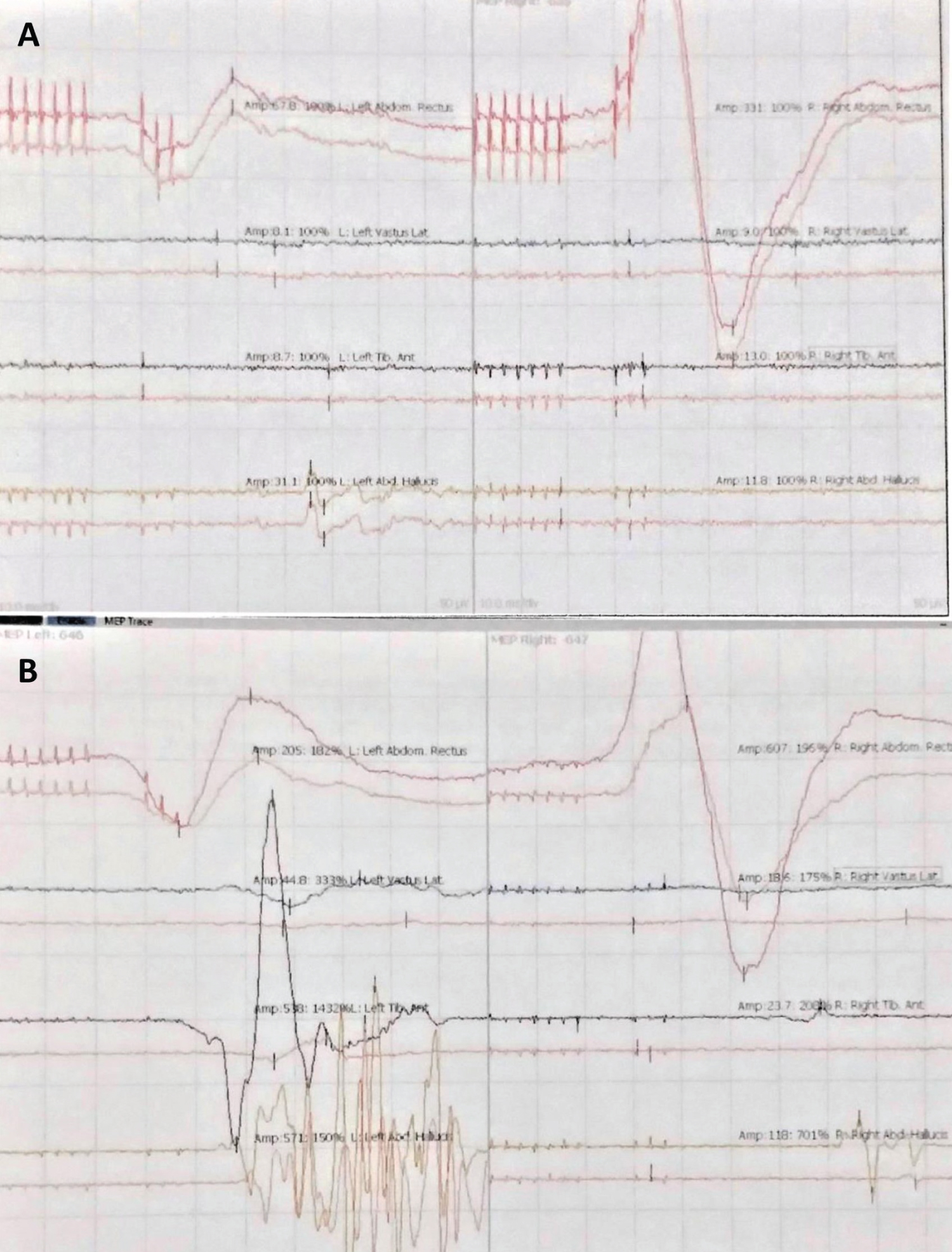
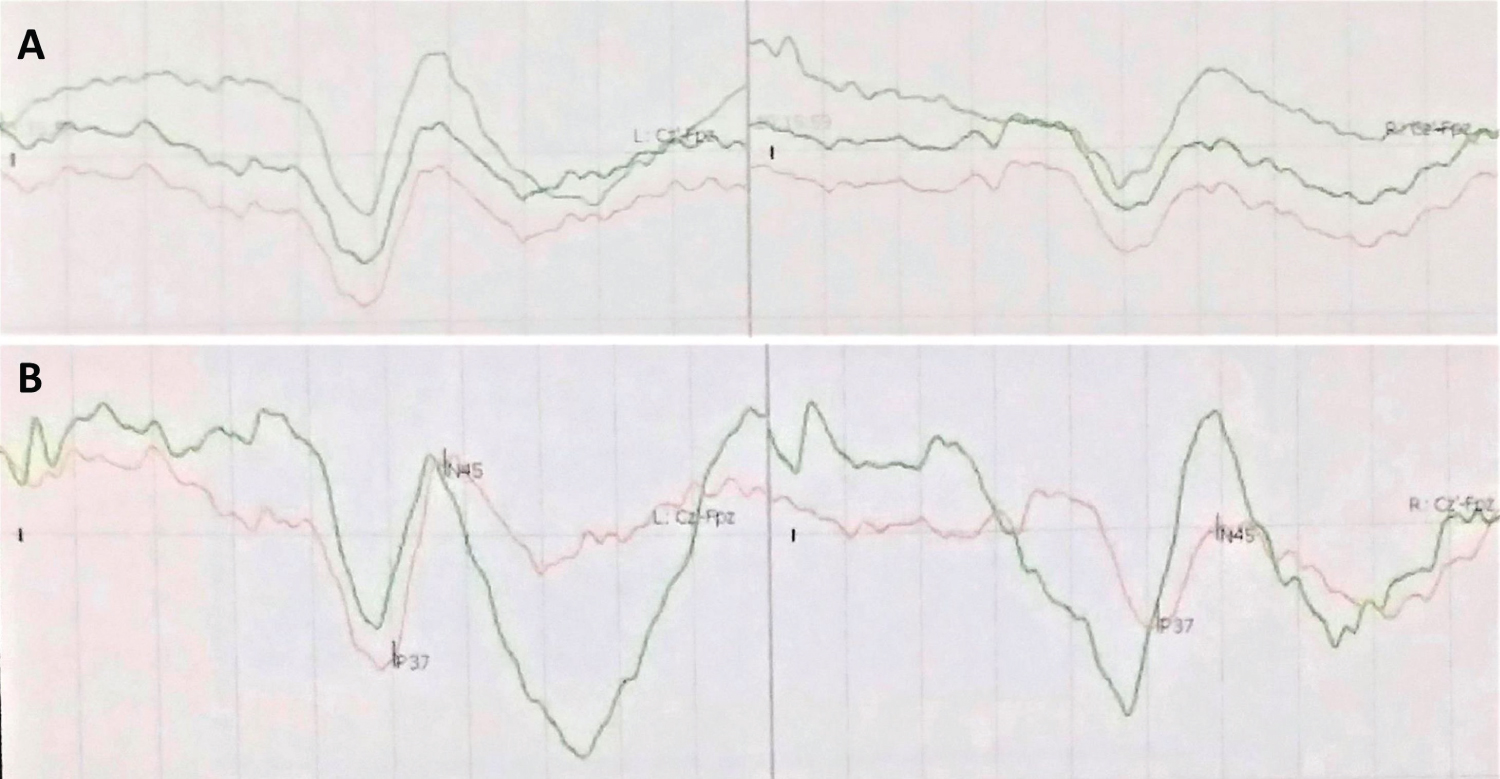
Laminectomy from T10 to T12 was performed. Intraoperatively, there was dense adhesion of OLF to the dorsal lateral dura at both levels. Decompression and thinning of OLF with floating technique using Kerrison rongeur and ultrasonic aspirator were performed. Surrounding bony attachment was also resected. The operation was performed under 3D fluoroscopic navigation system (Stryker NAV3i platform and integrated instrumentation), with matching of preoperative CT images (Figure 3). Upon the completion of decompression, pulsation was observed over the floated OLF. Throughout the operation, IONM was applied and modalities of somatosensory evoked potentials (SSEP) and motor evoked potentials (MEP) were adopted. Both signals showed improvement after the procedure when compared to the preoperative baseline level, and drastic increases in MEP signals over left side predetermined muscles, namely rectus abdominis, vastus lateralis, tibialis anterior and abductor hallucis, were observed (Figure 4 and Figure 5). There was no intraoperative dural tear and CSF leakage.
Postoperatively, the operation wound healed well. Rehabilitation with walking exercises was started since post operation day 5. He reported much improved numbness and was able to walk with frame under supervision at the time of discharge.
Discussion
This is a case report of T10/11, T11/12 OLF treated with decompression with floating technique, with the applications of IONM and navigation guidance, in a middle-aged gentleman. To the best of our knowledge, there is no report of managing OLF with such combination of technologies in the English literature.
OLF is an uncommon cause of thoracic myelopathy with majority of cases found in East Asian, especially in Japan. The condition was found in less than 5% of outpatient X-ray taken in Japanese population [5]. The exact etiology is still uncertain. It usually has an insidious and chronic progression, with presentations ranging from local thoracic pain and stiffness to slowly progressive myelopathy. T2W MRI is the most instrumental imaging modality for diagnosis, while CT is useful in differentiating hypertrophy and ossification of ligamentum Flavum [5]. In our patient, preoperative CT also played an additional role of navigation planning, which would be further discussed in the later paragraph. Conservative treatment has limited use and surgical decompression is vital for effective management of the condition.
Various surgical options have been discussed. Most commonly performed procedure is en bloc laminectomy with excision of ossified ligament [1,5,6]. Other techniques include laminotomy and laminoplasty. Nevertheless, Osman, et al. [1] performed a meta-analysis which included 6 studies that involved patients with thoracic OLF treated with laminectomy and ossified ligament excision. Multiple complications were reported in all studies. Dural tear was the most prevalent with a pooled incidence of 18.4%. Other complications included CSF leak, surgical site infection and neurological deficit. Correlation between dural ossification and significant incidence of dural tear and CSF leak was postulated. Alternative surgical technique involving laminectomy and floating ossification have been discussed to minimize the above named complications. Miyashita, et al. [2] reported a case of thoracic OLF in an elderly patient, with neurological improvement after laminectomy with floating ossification. Yamada, et al. [3] also described a case of multilevel thoracic OLF in a young patient, treated successfully with a combination of resection and floating technique, depending on the presence of dural adhesion. No dural tear or CSF leak was found. However, strong data to support this surgical technique in the current literature is still lacking. In our patient treated with floating technique, neither dural tear nor CSF leak was observed.
On the other hand, to improve the safety and efficiency of spine surgery, computer assisted navigation (CAN) has become an essential adjunct in recent years. 2D (dimensional) and 3D navigation, which differ in the imaging modality used for reference, are available. These technologies have been widely implemented in pedicle screw insertion. Shin, et al. [7] performed a meta-analysis which analyzed 20 studies with over 8500 screws involved. Significant reduction in the risk of pedicle perforation for navigated screw insertion was found when compared to non-navigated insertion in all spinal regions. Navigation for tumor resection was also described and had showed satisfactory results with complete resection and absence of intraoperative complications related to navigation [8]. Nonetheless, current experience in treating OLF with navigation is limited. Wang, et al. [9] has demonstrated that O-arm computer navigation accurately located the boundary of OLF during the decompression surgery in a retrospective study. O-arm was also used when treating multilevel OLF patient [3]. The modality we use was CT-based 3D fluoroscopic navigation which involved a matching of preoperative CT and intraoperative 3D fluoroscopic images. Position, size, shape and boundary of OLF could be precisely identified under real time guidance. To the best of our knowledge, there is no report of application of this modality in OLF decompression surgery in the English literature. Our experience has illustrated CT-based 3D fluoroscopy could be a feasible option of navigation when treating patients of thoracic OLF with decompression and floating ossification.
Another technique employed in our case was intraoperative neurophysiological monitoring (IONM). There is an increasing trend in its utilization in recent years to provide real time detection of perioperative neurological injury during spine surgery. Various modalities are available. The most commonly utilized techniques include somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs) and electromyography (EMG). Nevertheless, each modality has its own strength and weakness [10]. To achieve a comprehensive monitoring, Charalampidis, et al. [10] performed a meta-analysis and suggested that multimodal IONM (MIONM) had the advantage of compensating the limitations of each individual modality and was effective and accurate in detecting perioperative neurological injury in spine surgery. In our patient, SSEP and MEP were used. Gradual improvements in both sensory and motor signals upon the completion of the surgery suggested a favorable surgical outcome. In current literature, only Li, et al. [6] applied single modality, i.e. SSEP, when they managed 85 patients with thoracic OLF with decompressive laminectomy, but no MIONM used when managing thoracic OLF patient.
Conclusion
OLF is a rare cause of thoracic myelopathy that has poor response to conservative management. Decompression laminectomy with floating ossification is a feasible surgical option in case of dural adhesion. Applications of intraoperative 3D fluoroscopic navigation and IONM are instrumental in minimizing intraoperative complications.
Conflict of Interests Statement
The authors declare that they have no financial or non-financial conflicts of interest related to the subject matter or materials discussed in the manuscript.
References
- Osman NS, Cheung ZB, Hussain AK, et al. (2018) Outcomes and complications following laminectomy alone for thoracic myelopathy due to ossified ligamentum flavum: A systematic review and meta-analysis. Spine (Phila Pa 1976) 43: E842-E848.
- Miyashita T, Ataka H, Tanno T (2013) Spontaneous reduction of a floated ossification of the ligamentum flavum after posterior thoracic decompression (floating method); report of a case (abridged translation of a primary publication). Spine J 13: e7-e9.
- Yamada T, Torigoe I, Sakai K, et al. (2019) Contiguous multilevel thoracic ossification of ligamentum flavum in a young adult spine. Case Rep Orthop 2019: 1640485.
- Sun J, Zhang C, Ning G, et al. (2014) Surgical strategies for ossified ligamentum flavum associated with dural ossification in thoracic spinal stenosis. J Clin Neurosci 21: 2102-2106.
- Hirabayashi S (2017) Ossification of the ligamentum flavum. Spine Surg Relat Res 1: 158-163.
- Li Z, Ren D, Zhao Y, et al. (2016) Clinical characteristics and surgical outcome of thoracic myelopathy caused by ossification of the ligamentum flavum: A retrospective analysis of 85 cases. Spinal Cord 54: 188-196.
- Shin BJ, James AR, Njoku IU, et al. (2012) Pedicle screw navigation: A systematic review and meta-analysis of perforation risk for computer-navigated versus freehand insertion. J Neurosurg Spine 17: 113-122.
- Rawicki N, Dowdell JE, Sandhu HS (2021) Current state of navigation in spine surgery. Ann Transl Med 9: 85.
- Wang ZW, Wang Z, Fan XW, et al. (2020) Precise surgical treatment of thoracic ossification of ligamentum flavum assisted by o-arm computer navigation: A retrospective study. World Neurosurg 143: e409-e418.
- Charalampidis A, Jiang F, Wilson JRF, et al. (2020) The use of intraoperative neurophysiological monitoring in spine surgery. Global Spine J 10: 104S-114S.
Corresponding Author
Hoi Tung Lam, Department of Orthopaedics and Traumatology, 1/F, Main block, Tseung Kwan O Hospital, 2 Po Ning Lane, Hang Hau, Tseung Kwan O, Hong Kong SAR, 999077, China, Tel: +852-6253-0300, Fax: +852-2274-4051.
Copyright
© 2022 Lam HT, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.