Transfibular Approach to Hindfoot Arthrodesis Using an Acetabular Reamer: A Technique Tip
Abstract
The transfibular approach is commonly used for hindfoot arthrodesis. Fibula osteotomy with a saw blade and subsequent bone graft preparation can be time-consuming and prolong tourniquet time as well as prevent training opportunities. We describe a simple and reproducible technique to perform fibula osteotomy using an acetabular reamer. Advantages of this technique include reduction in operative time and use of the reamed bone as an autograft in the tibiotalar and talocalcaneal joints to bridge any voids and increase healing capacity.
Keywords
Transfibular approach, Ankle arthrodesis, Fibula osteotomy, Acetabular reamer, Technical tip
Introduction
The transfibular approach has become one of the workhorse surgical approaches to hindfoot and subtalar arthrodesis for end-stage arthritis. One of the first documented descriptions of this approach was by Adams in 1948 [1]. The approach utilises a lateral incision and distal fibula osteotomy in order to gain access to the tibiotalar and subtalar joints. This has numerous advantages including adequate exposure for joint surface preparation and fusion, it is extensile to allow access to the subtalar joint and the resected bone can be used as bone graft to augment the arthrodesis [2]. Multiple studies have demonstrated the transfibular approach to be a reproducible and reliable way to perform hindfoot arthrodesis procedures with minimal complications [2-5]. When performing the distal fibula osteotomy, the commonly described technique is to use a saw blade in order to transect the fibula in a proximal-lateral to distal-medial direction [5]. Differing levels at which this should be carried out have been described, ranging from 5 to 8cm proximal to the tip of the fibula [2,5]. This resected fibula can then be prepared into bone chips using a bone nibbler or equivalent for use as a graft between the articular surfaces being fused. In the author's experience, preparation of the fibula for bone graft can be time consuming, either for the surgeon or assistant. In this paper, we present a novel way to carry out the distal fibula osteotomy and immediate bone graft preparation using an acetabular reamer.
Technique
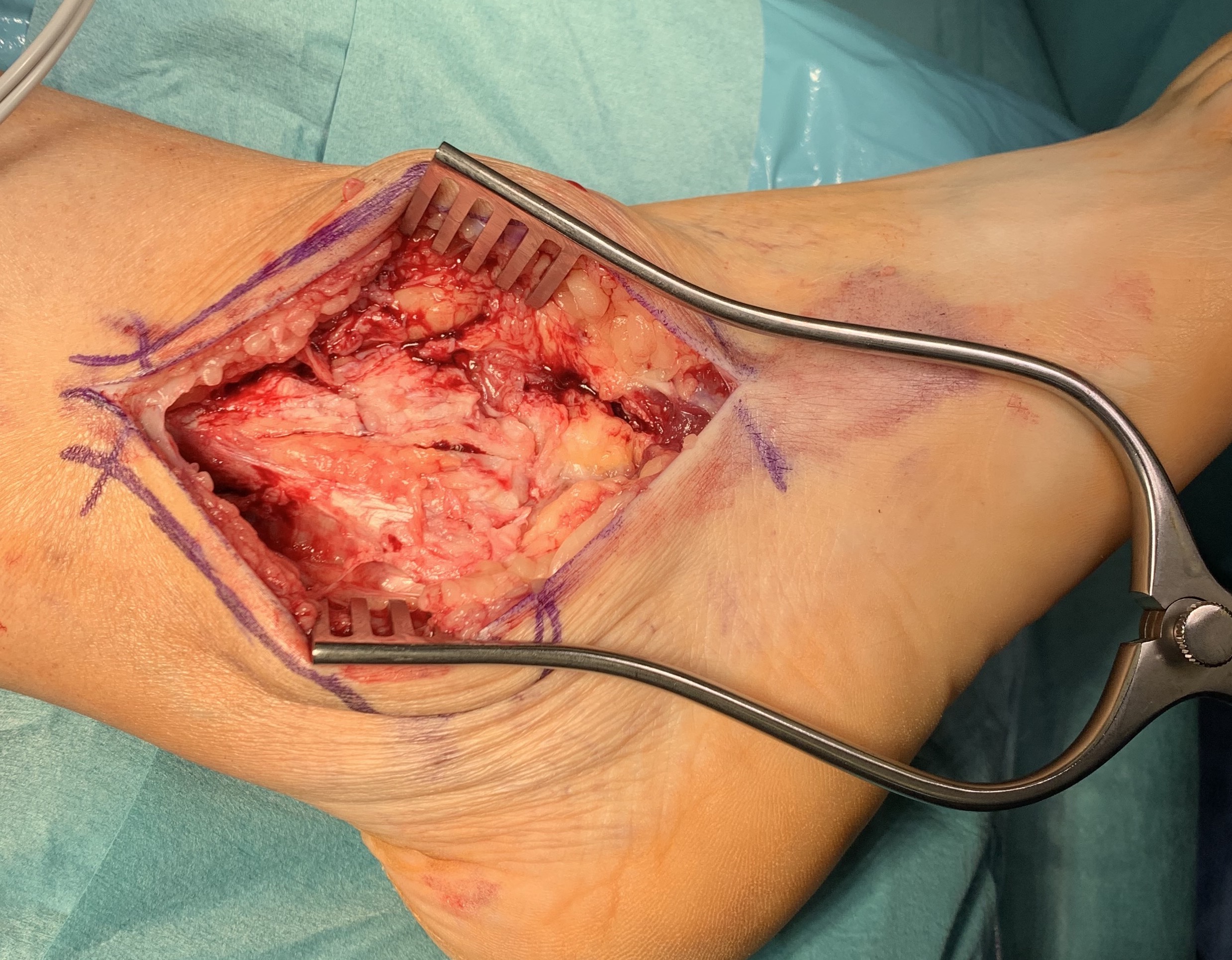
The transfibular approach is performed in a standard fashion. The patient is secured in a “floppy lateral” position. A thigh tourniquet is used to prevent blood loss during the procedure. A lateral longitudinal incision (usually 10-15 cm) is made over the fibula shaft just in front of the peroneal tendons extending distally along the sinus tarsi and curving anteriorly towards the base of the fourth metatarsal (Figure 1). Dissection is performed to expose the underlying fibula (Figure 2).
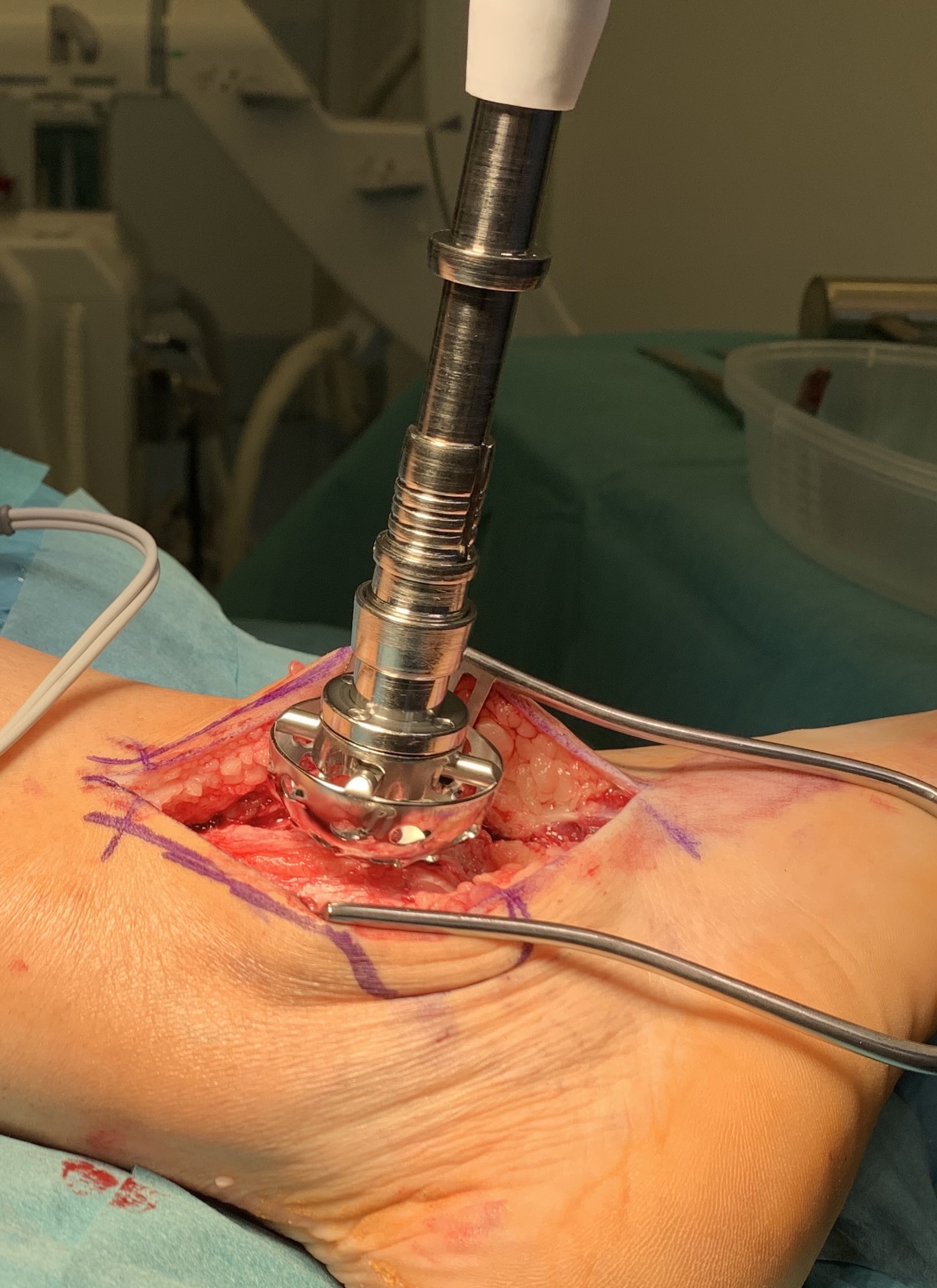
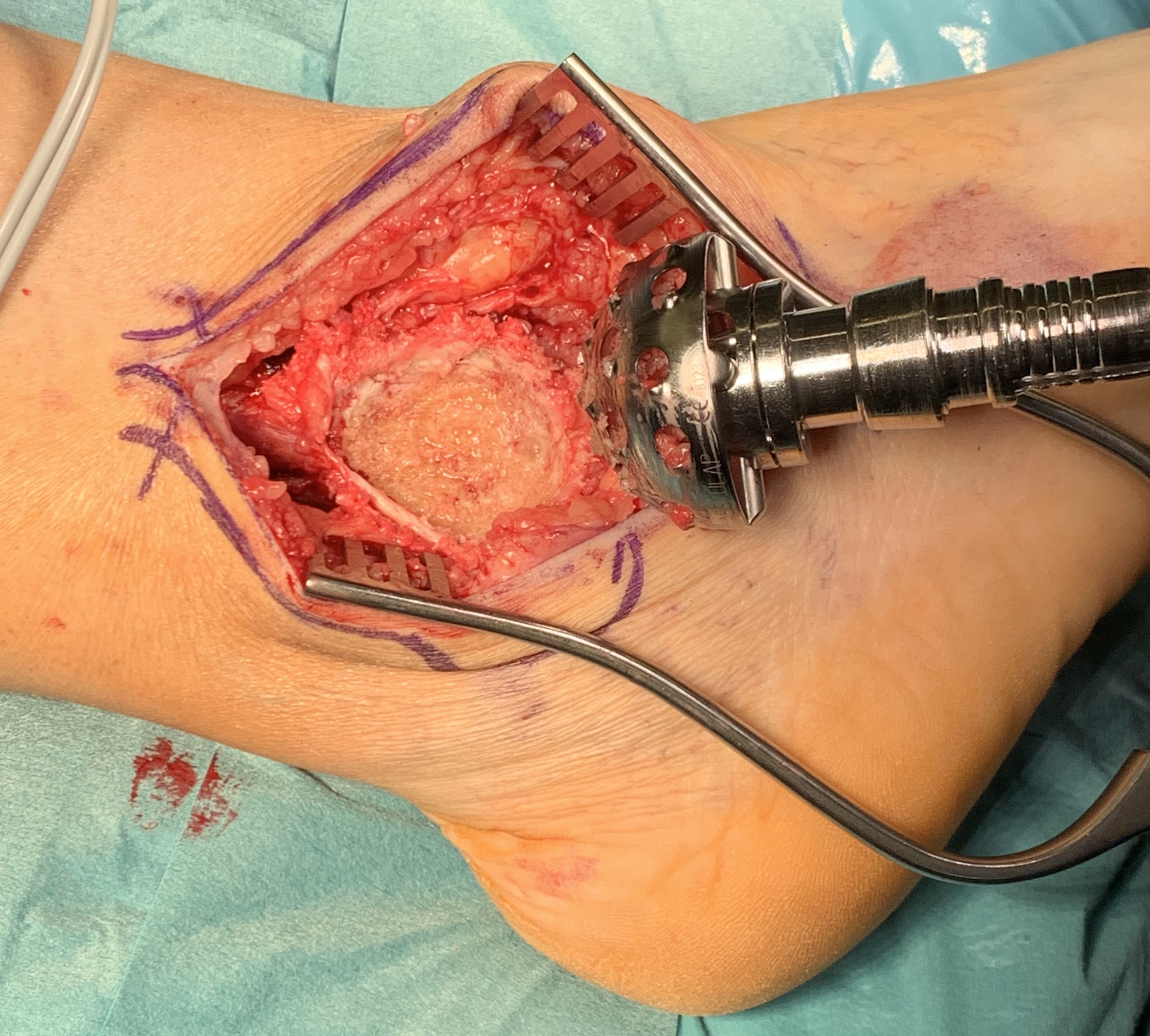
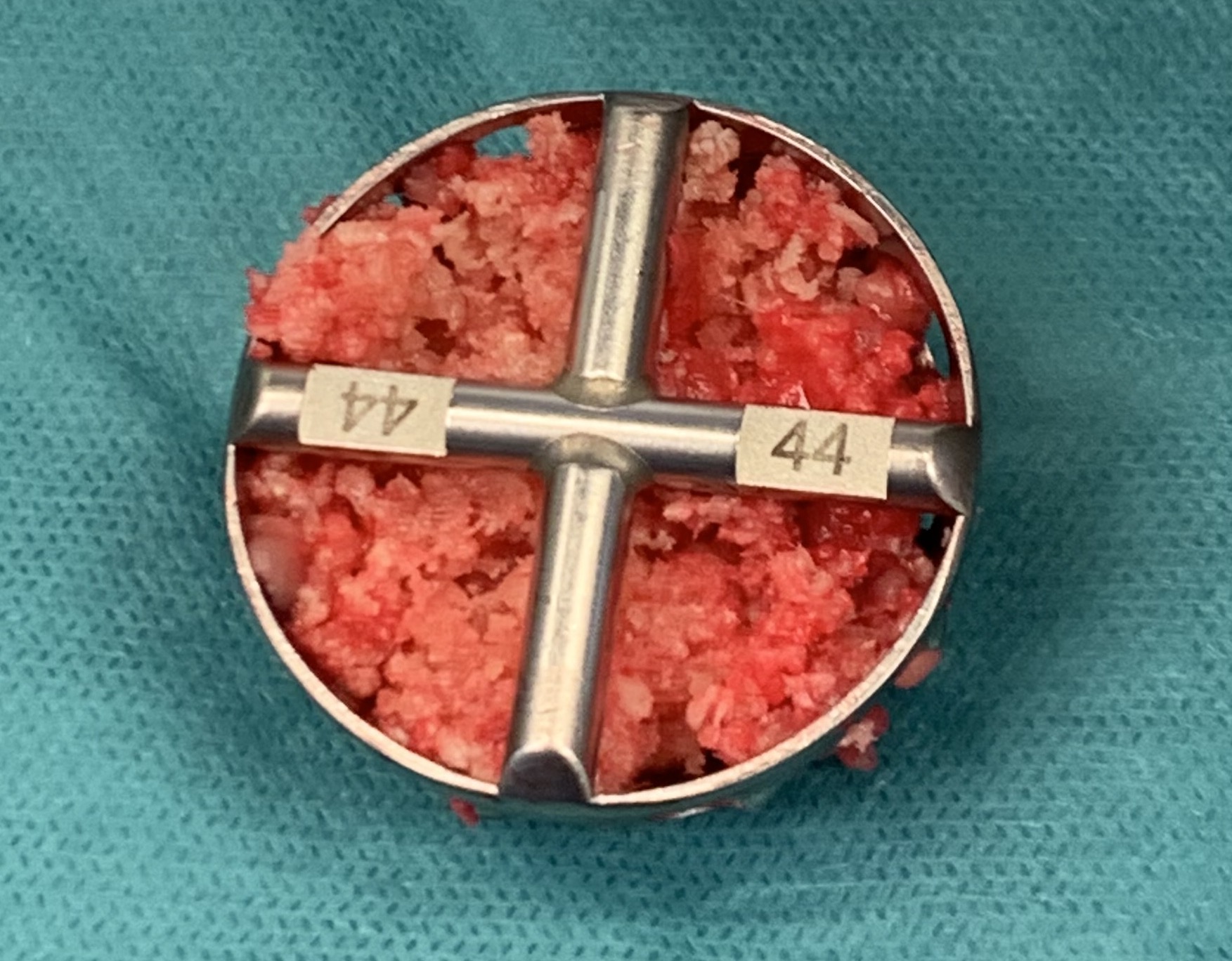
At this stage, surrounding soft tissue structures including the nerves, blood vessels, tendons and skin must be protected using either self-retaining or Hohmann retractors and the distal fibula resection can be performed. An entry acetabular reamer (for example 44 mm) is used directly over the distal fibula in order to resect the bone (Figure 3). This is checked at regular intervals to visualise the depth of the reaming (Figure 4). Reaming can be stopped once the lateral surface of the tibia and talus has been reached (Figure 5). The very distal end of the lateral malleolus can be subsequently dissected from its soft tissue attachments and excised. The edges of the remaining fibula are smoothened with a bone nibbler. The bone graft formed in the acetabular reamer is then collected (Figure 6).
Discussion
Bone graft preparation following traditional fibula osteotomy with a saw blade can be a time-consuming endeavour. Hindfoot/subtalar arthrodesis is commonly performed under a tourniquet and therefore it is important to perform the procedure in a timely fashion in order to prevent complications from prolonged tourniquet time [6]. Furthermore, if this bone preparation is left to the assistant (often a surgical resident or equivalent) they will no longer be able to actively participate in the procedure, which can leave the primary surgeon without assistance and preclude training opportunities for the assistant now focussed on preparing bone graft. Use of an acetabular reamer during hindfoot arthrodesis has been described previously in the context of preparing the joints by reaming the distal tibia and remaining talus/calcaneum to create a concave surface into which a femoral head allograft is subsequently inserted [7,8]. However, to the authors' knowledge, this is the first described use of an acetabular reamer to ream the distal fibula and use the reamed bone as an autograft.
Our technique using an acetabular reamer provides a fast, simple, and reproducible alternative to the traditional fibula osteotomy. The bone collected in the acetabular reamer allows for immediate use as bone autograft following articular surface preparation without the need to manually break up the bone. Furthermore, the finer bone graft produced, when compared to manually created bone chips, allows for more to be packed into the joint and bridge any voids, therefore aiding bony union. The curvature of the reamer maintains the normal proximal-lateral to distal-medial obliquity at the distal end of the resected fibula.
Conclusion
We describe a simple and reproducible technique for the transfibular approach using an acetabular reamer to reduce surgical time and provide immediate bone autograft.
Funding
No funding was received for this study.
Conflicts of Interest
The authors have no financial disclosures or conflicts of interest.
References
- Adams JC (1948) Arthrodesis of the ankle joint; experiences with the transfibular approach. J Bone Joint Surg Br 30: 506-511.
- Sripanich Y, Steadman J, Valderrabano V, et al. (2020) Open ankle arthrodesis: Transfibular approach 19: 26-36.
- Akra GA, Middleton A, Adedapo AO, et al. (2010) Outcome of ankle arthrodesis using a transfibular approach. J Foot Ankle Surg 49: 508-512.
- Balaji SM, Selvaraj V, Devadoss S, et al. (2017) Transfibular ankle arthrodesis: A novel method for ankle fusion - A short term retrospective study. Indian J Orthop 51: 75-80.
- Houng BE, Thompson JM, Mendicino RW (2021) Transfibular approach to ankle arthrodesis: Surgical technique guide and tips. Foot & Ankle Surgery: Techniques, Reports & Cases 1: 100038.
- Gangadharan R, Roslee C, Kelsall N, et al. (2021) Retrospective review of complications following long tourniquet time in foot and ankle surgery. J Clin Orthop Trauma 16: 189-194.
- Cuttica DJ, Hyer CF (2011) femoral head allograft for tibiotalocalcaneal fusion using a cup and cone reamer technique. J Foot Ankle Surg 50: 126-129.
- Rigby RB, Cottom JM (2013) Lateral simultaneous reaming technique with femoral head allograft implantation for tibiocalcaneal arthrodesis: A case report. Foot Ankle Spec 6: 45-49.
Corresponding Author
Sandeep Nayar, Department of Trauma and Orthopaedic Surgery, Queen's Hospital, Rom Valley Way, Romford, RM7 0AG, UK, Tel: +447-535-247-125.
Copyright
© 2022 Nayar SK, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.