Different Methods of Treatment of Distal Radius Fracture Including External Fixator with Kirschner Wires Augmentation and Internal Fixation
Abstract
Introduction: Distal radius fractures represent approximately one-sixth of all fractures presenting in the emergency room. Different fixation options have been described. This study compared two methods for displaced intra-articular distal radius fracture fixation, namely closed reduction and Kirschner wire augmented external fixation versus open reduction and internal fixation (ORIF) with a locked volar plate.
Aim: To compare functional and radiological outcomes following treatment of distal radius fracture by ORIF using volar plate versus external fixation with Kirschner wire augmentation.
Patients and methods: 40 patients with intra articular distal radius fracture were treated operatively, between December 2018 and June 2020. Twenty patients were treated by ORIF and 20 patients by external fixation with K-wire augmentation. All cases were evaluated clinically and radiologically at 2, 4, 6, 12 weeks and thereafter at 6, 12, 18 months. The Cooney modification of the Green and O'Brien score for functional assessment and the Sarmiento score for radiological assessment were used at 18 months to directly compare between the two methods of treatment.
Results: ORIF had better functional outcomes in Green and O'Brien compared to external fixation. 90% of the ORIF had accepted functional outcomes (70% excellent, 20% good) 75% external fixation had accepted functional outcomes (70% excellent, 5% good). The radiographic results in ORIF were more favorable than in EF. 95% of ORIF had acceptable radiological parameters (95% got excellent in Sarmiento score). 85 % in external fixation (70% got excellent & 15% got good in Sarmiento score).
Conclusion: Functional and radiological outcomes were better in ORIF with fewer complications as compared to K-wire augmented external fixation.
Keywords
Distal, External, Radius, Volar, ORIF
Introduction
Distal radius fractures represent approximately one-sixth of all fractures presenting in the emergency room. They are considered the most common fracture of the upper extremity [1,2].
Different fixation options for the various subtypes of distal radius fractures have been described, yet in specific situations the ideal management remains controversial [3,4].
The past 70 years have witnessed the evolvement of 15 different classification systems, though only 8 are commonly used whereas the other 7 lack sufficient reproducibility and reliability [5]. In this study, the AO/OTA classification system was used due to its inert comprehensiveness, its proven reliability, reproducibility and its widespread use in research. Furthermore, it provides a solid foundation for treatment and allows for retrospective outcome assessment.
This study compared two methods of treatment for displaced intra-articular distal radius fracture fixation, namely closed reduction and Kirschner wire augmented external fixation versus open reduction and internal fixation (ORIF) with a locked volar plate.
Patients and methods
In the period between December 2018 and June 2020, 40 patients with intra-articular distal radius fractures (AO/OTA 23-B and 23-C) were included in this randomized prospective study which was previously approved by the pertinent Ethical Review Board. Open fractures of distal radius and associated head injury were excluded from the study. Forty consecutive patients who presented to the emergency room of our tertiary trauma facility received a detailed informed consent and were randomized per Research Randomizer, an online free randomization software [6].
20 patients were managed by open reduction and internal fixation with a locked plate (ORIF-group) while 20 cases were managed by a K-wire augmented external fixator (EF-group). All surgical procedures were performed by a single surgeon at a single institute.
Patients aged 18-60 years with recent intra-articular fracture of the distal radius with no medical contraindications for anesthesia were included in the study.Patients with extra-articular fractures, fractures older than 14 days, active infection or severe radiocarpal arthritis were excluded from this study. The minimum intended follow-up was set to 18 months and averaged 25 months (range 19 to 28 months). In each group 17 patients (85%) were males. The average age in the EF-group was 36.4 ± 8.7 years while in the ORIF-group was 43.1 ± 15.4 years. The most common mode of trauma in both groups was falling down from a standing height with 16 patients (80.0%) and 13 patients (65.0%) for the ORIF and EF-group, respectively (Table 1).
Standard biplanar X-rays of the wrist were used to classify the fracture per the AO/OTA classification system [7] and preoperative demographic data and relevant history were appraised. In five cases a computer tomography with 3D reconstruction was required to further delineate the fracture geometry.
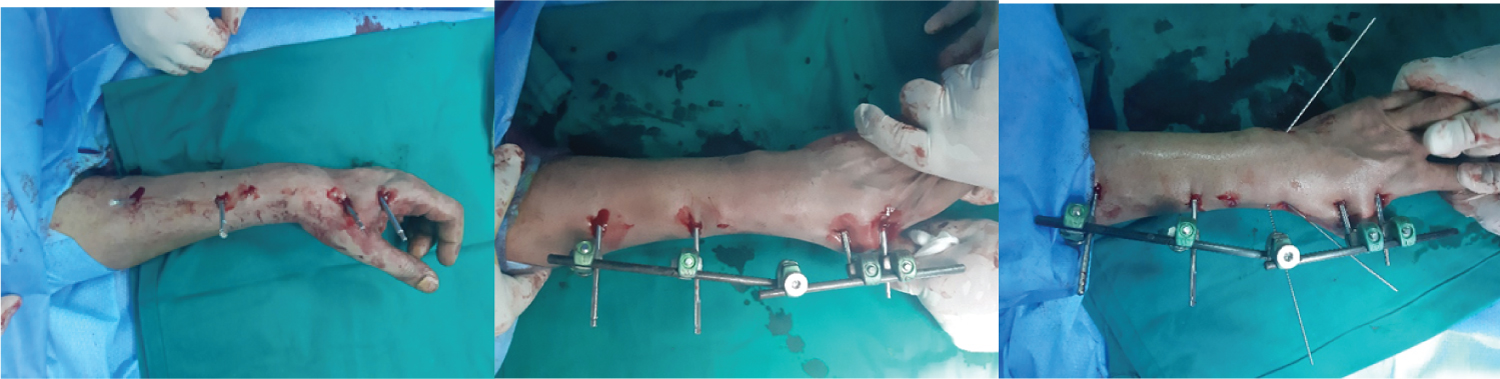
A K-wire augmented Orthofix Galaxy external fixator (Orthofix Srl, Verona, Italy) was used to maintain reduction in the EF-group. General anesthesia was applied in 9 cases (45%) and regional nerve block (axillary brachial plexus block) in 11 cases (55%). Two small incisions for the 2 proximal fixator 4 mm pins were made on the dorso-radial aspect of the radial shaft about 5 cm apart. The superficial branch of the radial nerve is susceptible during this step, so the pins were placed in the interval between the extensor carpi radialis brevis and longus. Through a skin incision near the base of second metacarpal dorso-radially two distal Schanz pins of 2.5-3 mm 40-60° in reference to the horizontal plane were applied.
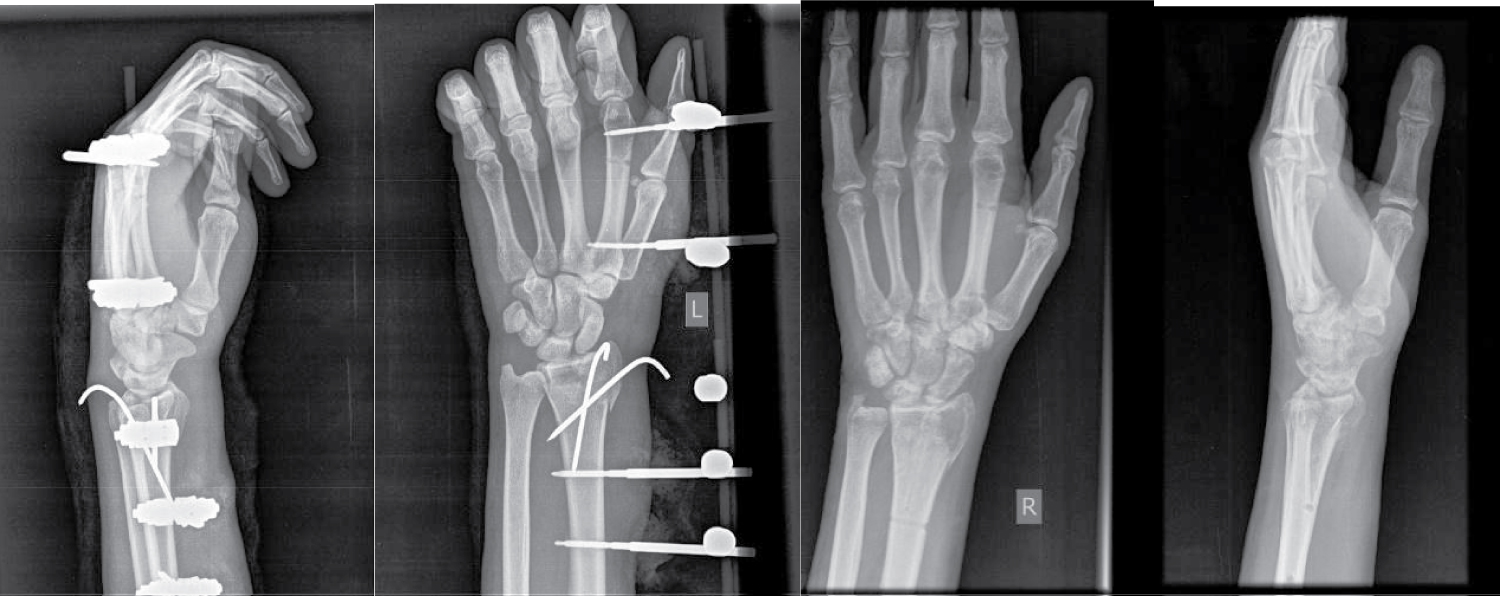
This was followed by controlled traction and reduction of the distal segment. To avoid overzealous traction and prospective joint stiffness, the intercarpal distance equaled the radiocarpal distance on the image intensifier. Once the desired reduction was achieved the assistant tightened the other clamp to maintain this position. One or two percutaneous 1.6 mm K-wires were inserted from the radial styloid directed proximally toward the opposite intact cortex. Another 1.6 mm wire was added from the dorso-ulnar aspect of the distal radius and was directed towards the volar aspect to engage the opposite intact cortex. Another horizontal 1.6 mm wire was added to maintain distal radioulnar joint (DRUJ) only in case of associated distal radioulnar joint dislocation. The patients were encouraged to use their affected hand immediately postoperative and to move their fingers to the maximum attainable range of motion. The external fixator device and K-wires were removed at 6 to 8 weeks according to union (Figure 1).
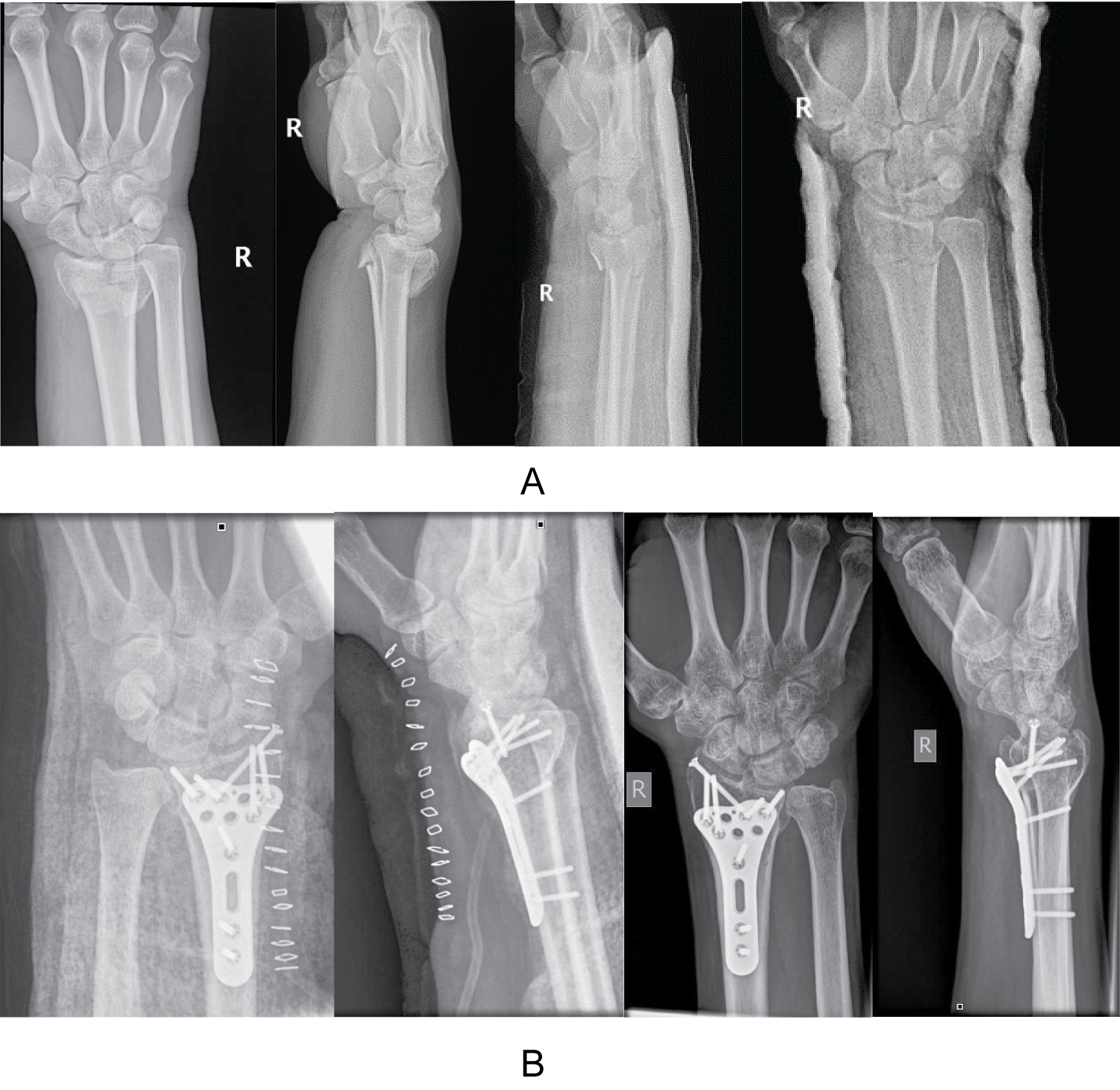
The flexor carpi radialis [FCR] approach as described by orbay and Fernandez [8] was utilized for volar plating. Eight patients (40%) received general anesthesia, while regional nerve block (axillary brachial plexus block) was used in 12 cases (60%). The application of locked anatomical volar distal radius plates (Variax distal radius locking plate system of Stryker) necessitated image intensification which involved posteroanterior, lateral, oblique views (supination and pronation oblique views), inclination views (inclined lateral view with 23° tilt and inclined posteroanterior view with 11° tilt) to ensure restoration of normal radiological parameters and proper screw length and position. Stability of the distal radio-ulnar joint was assessed clinically and in case of instability, a transverse 1.6 mm K-wire from the distal ulna to the distal radius was applied and its position verified by image intensification. This K-wire was again routinely removed at 6 weeks (Figure 2).
All cases were evaluated clinically for pain, activities, range of motion and grip strength and radiologically (by X-rays with P-A & lateral views). Radiological parameters included radial height, palmar tilt, radial inclination, ulnar variance, anteroposterior distance, position of the DRUJ, fracture healing and position of hardware.
This was assessed immediately postoperatively and at 2, 4, 6, 12 weeks and thereafter at 6, 12, 18 months. The Cooney modification of the Green and O'Brien score [9] for functional assessment and the Sarmiento score [10] for radiological assessment were used at 18 months to directly compare between the ORIF-group and EF-group (Figure 3 and Figure 4).
The statistical evaluation conducted by SPSS (IBM, Newark, USA) included the Chi-square test which was used for comparison of qualitative categorical variables while the Student's t test was used for comparison of quantitive data in the form of mean and slandered deviation. P value was checked at 5% level of significance (P ≤ 0.05). The Spearman rho correlation was used to evaluate association in the final grading (excellent, good, fair, and poor) between different outcome instruments.
Results
20 patients were managed by ORIF and 20 patients were managed by EF, mean age of the EF group was 36.4 while that of the ORIF group was 43.1. The percentage of males was 85% in both groups. In the ORIF group 80% were Class C (2R3C) and 20% were class B (2R3B) while in the EF group 92% were Class C (2R3C) and 8% were class B (2R3B). Falling down was the most frequent cause of trauma in both groups, followed by fall from a height, while road traffic accident was the least common cause. Trauma was of the low energy type in 80% of patients in the ORIF group and in 65% in the EF group. The frequency or mode of trauma were not significantly different between the groups (p = 0.288).
The ORIF group showed better functional outcomes in Green & O'Brien compared to EF group. Ninety percent (90%) of the ORIF group had accepted functional outcomes (70% excellent, 20% good), while 75% of the EF group had accepted functional outcomes (70% excellent, 5% good).
The radiographic results in the ORIF group were more favorable than in the EF group, where 95% of the ORIF group had acceptable radiological parameters (95% got excellent in Sarmiento score), the percentage was 85% in the EF group (70% got excellent & 15% got good in Sarmiento score).
Regarding injury to treatment interval, 70% of patients in the ORIF group and 65% of patients in the EF group were subjected to surgical management one day after the injury. In all patients, the amount of blood loss was less than 500 cm3. The mean operation time was 45.5 minutes ± 10.75 in the ORIF group, in comparison to 23.25 minutes ± 5.68 in the EF group. Student's t test revealed a statistically significant difference between both groups regarding the operation time (p = 0.00).
According to Green and O'Brien score, 70% of the two groups achieved excellent outcome, with no significant difference between the two groups (p = 1.000) (Table 2). Ninety percent (90%) of the ORIF group had accepted functional outcomes (70% excellent and 20% good) as compared to 75% of the EF group (70% excellent & 5% good).
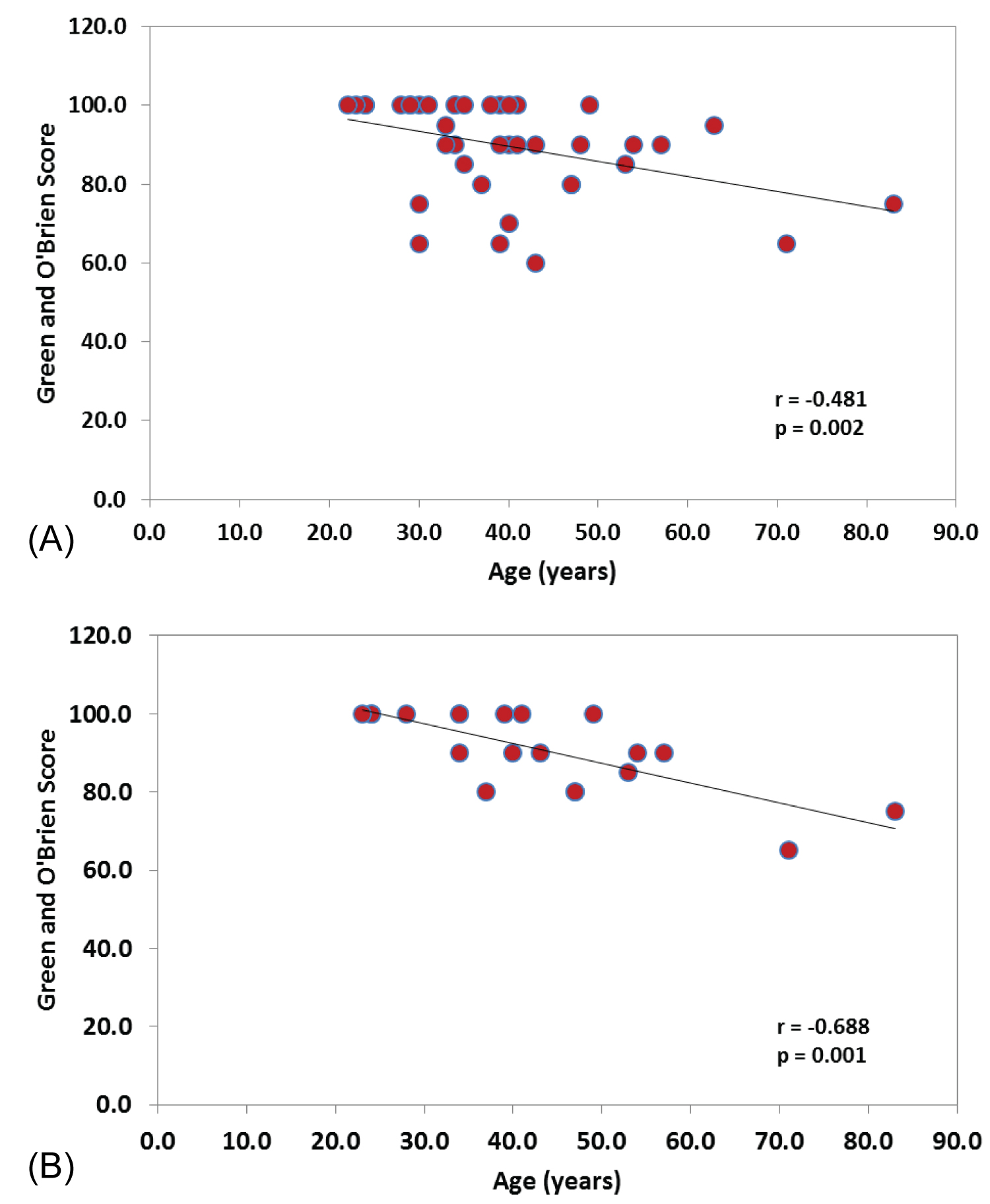
Spearman's test revealed that the Green and O'Brien score had negative correlation with age and interval between trauma & surgery in the whole group (n = 40). This correlation was statistically significant (p = 0.002, p = 0.033 for age and interval to surgery respectively) (Figure 5). This negative correlation was statistically significant (p = 0.001, p = 0.014 for age and interval to surgery respectively) in the ORIF group, but did not reach the level of statistical significance in the EF group (p = 0.093, p = 0.451 for age and interval to surgery respectively). The two groups were comparable in palmar tilt (p = 0.798), radial height (p = 0.478), and radial inclination (p = 0242) (Table 3).
According to Sarmiento radiological score, 95% of the patients in the ORIF group achieved excellent outcome, in comparison to 70% of the patients in the EF group. Chi-square test revealed that this difference was statistically significant (p = 0.047) (Table 3). The percentage of patients with acceptable radiological parameters in the ORIF group was 95% (95% got excellent in Sarmiento score), while in the external fixator group it was 85% (70% got excellent & 15% got good in Sarmiento score).
Regarding the frequency of postoperative complications in the two groups; there were no cases of tendon injury in the two groups. Generally, 20% of patients in the ORIF group developed complications, in comparison to 25% in the EF group. Chi square test revealed no significant difference between the two groups in the total number of patients who developed postoperative complications (p = 0.980) (Table 4).
Discussion
Fractures of the distal radius are commonly encountered injuries. They usually occur as a cause of high-energy trauma in young individuals and low-energy trauma in elderly. As a warrant for a good outcome, restitution of the radio-carpal and radioulnar articular surfaces in particular and gross anatomical features of the distal radius as radial length, inclination and volar tilt in general have been identified [11].
In this study, variables such as age, gender, the dominant hand, standard radiographic values, grip power and range of motion were evaluated. In addition, radiological Sarmiento and functional Green and O'Brien Scoring scores were appraised, to compare between the ORIF-group and the EF-group.
The radiographic results in the ORIF group were more favorable than in the external fixator group. The percentage of patients with acceptable volar tilt, radial length and radial inclination in the ORIF group was 95%, while in the external fixator group it was 85% (70% received excellent and 15% a good result per Sarmiento score). This is mostly because of plating which allows direct visualization and manipulation of the fracture and therefore provides better restoration of radial height, radial inclination, volar tilt and articular congruity.
Most of the prior studies support these radiological results [12-19].
Other studies showed that there is no significant difference in radiological results between ORIF group and external fixation group, which is in contradiction to the current study results, as in Wei, et al. [20]. There were no significant differences in radial inclination, volar tilt, ulnar variance, radial length, and step-offs with gaps between the two methods of fixation in the studies done by Kreder, et al. [21] and Drobetz, et al. [22].
In this study, the ORIF group patients had better functional outcomes as per Green and O'Brien score when compared to the EF group patients; 90% of the ORIF group patients have accepted functional outcome (70% excellent and 20% good) as compared to 75% of external fixation group patients (70% excellent & 5% good). Most of the prior studies are in agreement with these results as in Williksen, et al. [23], Antonio Abramo, et al. [24], Rozental, et al. [25], Wei, et al. [20] and Egol, et al. [26].
In the study by Mellstrand, et al. [12], in which they compared between ORIF (69 patients) and external fixation (65 patients), the range of motion was equal in both groups except for radial deviation, which was better in the volar locking plate group at 1-year follow-up.
On the other hand, some studies showed results different from the results of the current study as in Grewal, et al. [27] study, in which 53 patients were randomized to be treated with ORIF (27 patients) and augmented external fixation (26 patients). The ORIF group had higher levels of pain at 1 year when compared with the external fixator group; however, this equalized after hardware removal. The external fixation group showed an average grip strength of 97% compared with the normal side and 86% in the dorsal plate group.
In the current study, ORIF had an overall decreased incidence of complications compared with external fixation, Complex regional pain syndrome was observed in three patients (15%) in the EF group but was not encountered in the ORIF group. This may be related to the severity of injury or excessive distraction and reduction maneuvers associated with external fixation. This can be avoided by early wrist rehabilitation, avoidance of over distraction during external fixator application and postoperative vitamin C supplementation. Stiffness was observed in two patients (10%) of the ORIF group, in comparison to three patients (15%) in the EF group.
In the ORIF group, the strength and stability of the construct allows early wrist motion, and this has been shown to decrease the incidence of stiffness and enhance hand and finger function. Infection was observed only in one patient (5%) of the external fixator group (pin tract infection) but was absent in ORIF group. Mal-union was observed in three patients (15%) of the external fixation group compared to only one patient (5%) in the ORIF group. In this study, ORIF restored volar tilt and radial inclination better than external fixation.
These results are in concordance with most of the prior studies, which have tended to show less complications in patients treated with ORIF [20,21,23-25,28-33].
Conversely, some studies showed higher incidence of complications in ORIF patients than external fixation patients, which is different than the results of the current study, as in Mellstrand, et al. [12], Egol, et al. [26] and Kapoor, et al. [14].
Finally we found that both ORIF and external fixation represent treatment choices for distal radius fractures. ORIF had better functional and radiological outcomes according to Green & O'Brien and Sarmiento scoring systems when compared to external fixation. ORIF had less incidence of complications compared with external fixation. ORIF allows better anatomical reduction of the fracture fragments and more stable construct, this allows early postoperative range of motion exercises as compared to external fixation. The grip strength was better in the ORIF group; however, it improved gradually in external fixation group after frame removal and physiotherapy, thus became comparable to the ORIF group. External fixation is a rapid, minimally-invasive, and low cost technique with comparable functional outcome with other methods of fixation.
Our study was a randomized prospective comparative study which added to its strength while the limitations were the relative small sample size, and the short follow up period. Further studies with larger sample size and longer follow up periods are needed to identify factors that predict outcomes and to explore different management strategies to achieve the best outcome.
We also recommend some tips and pitfalls
In the EX FIX group.
• The superficial branch of the radial nerve is susceptible during insertion of distal pins, so the pins were placed in the interval between the extensor carpi radialis brevis and longus.
• To avoid overzealous traction and prospective joint stiffness the intercarpal distance equaled the radiocarpal distance on the image intensifier
• The patients were encouraged to use their affected hand immediately postoperative and to move their fingers to the maximum attainable range of motion.
In the ORIF group
• Avoid placing the plate above watershed area which can result in frictional irritation with flexor tendons and subsequent rupture, also repair of the L-shaped incision of the pronator quadratus muscle by interrupted sutures to cover the plate is essential to avoid frictional irritation with the flexor tendons passing volar to the pronator quadratus muscle.
• Image intensification which involved posteroanterior, lateral, oblique views (supination and pronation oblique views), inclination views (inclined lateral view with 23° tilt and inclined posteroanterior view with 11° tilt) to ensure restoration of normal radiological parameters and proper screw length and position.
• Postoperatively, engourge the patients Active full range of movements started for fingers since immediate postoperatively, and for the wrist after 2 weeks for simple fractures, and after 6 weeks for comminuted fractures.
Conclusion
Both ORIF by a volar locked plate and K-wire augmented external fixation represent valid treatment options for distal radius fractures. Functional and radiological outcomes were better in ORIF with fewer complications. In addition, early postoperative mobilization and an early improved grip strength lead us to whenever applicable to prefer open reduction and internal fixation with plating for treatment of intraarticular fracture distal radius over external fixation.
References
- Asif Ilyas M, Jesse Jupiter B (2007) Distal radius fractures-classification of treatment and indications for surgery. Orthop Clin N Am 38: 167-173.
- Kenneth Koval J, John Harrast J, Jeffrey Anglen O, et al. (2008) Fractures of the distal part of the radius. The evolution of practice over time. Where's the evidence? J Bone Joint Surg Am 90: 1855-1861.
- Knox J, Ambrose H, McCallister W, et al. (2007) Percutaneous pins versus volar plates for unstable distal radius fractures: A biomechanic study using a cadaver model. J Hand Surg Am 32: 813-817.
- Gouk C, Ng SK, Knight M, et al. (2019) Long term outcomes of open reduction internal fixation versus external fixation of distal radius fractures: A meta-analysis. Orthop Rev (Pavia) 11: 7809.
- Shehovych A, Salar O, Meyer C, et al. (2016) Adult distal radius fractures classification systems: Essential clinical knowledge or abstract memory testing? Ann R Coll Surg Engl 98: 525-531.
- Urbaniak GC, Plous S (2013) Research Randomizer (Version 4.0).
- Muller ME, Nazarian S, Koch P (1987) Classification AO des fractures. Paris, Springer Verlag.
- Khatri K, Sharma V, Farooque K, et al. (2016) Surgical treatment of unstable distal radius fractures with a volar variable-angle locking plate: Clinical and radiological outcomes. Arch Trauma Res 5: e25174.
- Cooney WP, Bussey R, Dobyns JH, et al. (1987) Difficult wrist fractures perilunate fracture-dislocations of the wrist. Clin Orthop Relat Res 214: 136-147.
- Sarmiento A, Pratt G, Berry N, et al. (1975) Colles' fractures. Functional bracing in supination. J Bone Joint Surg Am 57: 311-317.
- Cowie J, Anakwe R, McQueen M (2015) Factors associated with one-year outcome after distal radial fracture treatment. J Orthop Surg 23: 24-28.
- Mellstrand Navarro C, Ahrengart L, Törnqvist H, et al. (2016) Volar locking plate or external fixation with optional addition of K-wires for dorsally displaced distal radius fractures: A randomized controlled study. J Orthop Trauma, 30: 217-224.
- Zamzuri Z, Yusof M, Hyzan MY (2004) External fixation versus internal fixation for closed unstable intra-articular fracture of the distal radius. Early results from a prospective study. Med J Malaysia 59: 15-9.
- Kapoor H, Agarwal A, Dhaon BK (2000) Displaced intra-articular fractures of distal radius: A comparative evaluation of results following closed reduction, external fixation and open reduction with internal fixation. Injury 31: 75-79.
- Jeudy J, Steiger V, Boyer P, et al. (2012) Treatment of complex fractures of the distal radius: A prospective randomized comparison of external fixation 'versus' locked volar plating. Injury 43: 174-179.
- Gereli A, Nalbantoglu U, Kocaoglu B, et al. (2014) Comparative study of the closed reduction percutaneous cannulated screw fixation and open reduction palmar locking plate fixation in the treatment of AO type A2 distal radius fractures. Arch Orthopaed Trauma Surg 134: 121-129.
- Zhang PX, Xue F, Dang Y, et al. (2012) Clinical effect of distal radius fracture treated with open reduction and internal plate fixation. Chin Med J (Engl) 125: 140-143.
- Neander GU, Chien SH (2009) Volar plating or external fixation of dorsally displaced fractures of distal radius. JBJS.
- Kiliç A, Kabukçuoglu Y, Ozkaya U, et al. (2009) Volar locking plate fixation of unstable distal radius fractures. Acta Orthop Traumatol Turc 43: 303-308.
- Wei DH, Raizman NM, Bottino CJ, et al. (2009) Unstable distal radial fractures treated with external fixation, a radial column plate, or a volar plate. A prospective randomized trial. J Bone Joint Surg Am 91: 1568-1577.
- Kreder HJ, Hanel DP, Agel J, et al. (2005) Indirect reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular fractures of the distal radius: A randomised, controlled trial. J Bone Joint Surg Br 87: 829-836.
- Drobetz HE, Mackay base hospital (2010) Volar locking plate versus external fixation/cast fixation for the treatment of distal radius fractures. JBJS.
- Williksen JH, Frihagen F, Hellund JC, et al. (2013) Volar locking plates versus external fixation and adjuvant pin fixation in unstable distal radius fractures: A randomized, controlled study. J Hand Surg Am 38: 1469-1476.
- Abramo, Kopylov P, Geijer M, et al. (2009) Open reduction and internal fixation compared to closed reduction and external fixation in distal radial fractures: A randomized study of 50 patients. Acta Orthop 80: 478-485.
- Rozental TD, Blazar PE (2006) Functional outcome and complications after volar plating for dorsally displaced unstable fractures of the distal radius. J Hand Surg 31: 359-365.
- Egol K, Walsh M, Tejwani N, et al. (2008) Paksima Bridging external fixation and supplementary Kirschner-wire fixation versus volar locked plating for unstable fractures of the distal radius: A randomised, prospective trial. J Bone Joint Surg Br 90: 1214-1221.
- Grewal R, Mac Dermid JC, King GJ, et al. (2011) Open reduction internal fixation versus percutaneous pinning with external fixation of distal radius fractures: A prospective, randomized clinical trial. J Hand Surg Am 36: 1899-1906.
- Karantana A, Downing ND, Forward DP, et al. (2013) Surgical treatment of distal radial fractures with a volar locking plate versus conventional percutaneous methods: A randomized controlled trial. J Bone Joint Surg Am 95: 1737-1744.
- Wilcke MK, Abbaszadegan H, Adolphson PY (2011) Wrist function recovers more rapidly after volar locked plating than after external fixation but the outcomes are similar after 1 year. Acta Orthop 82: 76-81.
- Xu GG, Chan SP, Puhaindran ME, et al. (2009) Prospective randomised study of intra-articular fractures of the distal radius: Comparison between external fixation and plate fixation. Ann Acad Med Singapore 38: 600-606.
- Leung F, Tu YK, Chew WY, et al. (2008) Comparison of external and percutaneous pin fixation with plate fixation for intra-articular distal radial fractures. A randomized study. J Bone Joint Surg Am 90: 16-22.
- Grewal R, Perey B, Wilmink M, et al. (2005) Randomized prospective study on the treatment of intra-articular distal radius fractures: Open reduction and internal fixation with dorsal plating versus mini open reduction, percutaneous fixation, and external fixation. J Hand Surg Am 30: 764-772.
- McQueen MM, MacLaren A, Chalmers J (1996) The value of re-manipulating Colles fractures. J Bone Joint Surg Br 68: 232-233.
Corresponding Author
Ahmed Hamdi, Department of Orthopaedic Surgery, Cairo University, Egypt, Tel: 00201146131132.
Copyright
© 2021 Barakat AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.