Fastest Recovery Time in Pediatric Tibial Tubercle Avulsion Fracture Repair Using SpeedBridge Double-Row Technique: A Case Report
Introduction
Tibial Tuberosity Avulsion Fractures (TTAF) are rare, accounting for less than 1% of pediatric fractures [1]. They typically occur in adolescent males by avulsion of the bony insertion of the patellar tendon, due to a sudden contraction of the quadriceps muscles [2]. This often occurs with jumping. To ensure the stability of the knee joint and good range of motion with minimal to no laxity, surgical reduction of the fracture is necessary [3]. Several techniques have been described and utilized to reduce tibial spine avulsion fractures. Most of these techniques require internal fixation with a screw, leaving the patient out of sports and activity for, at minimum, 3 months. Traditionally used in rotator cuff tear repair, we describe a method not previously reported in literature to treat TTAF using an all-suture, double-row knotless repair technique to reduce the fractured tibial spine with no need for screws, plates, or metal. This surgical method allows the patient to proceed postoperatively without casting, with early range of motion, immediate therapy and fastest return to sports.
Case Presentation
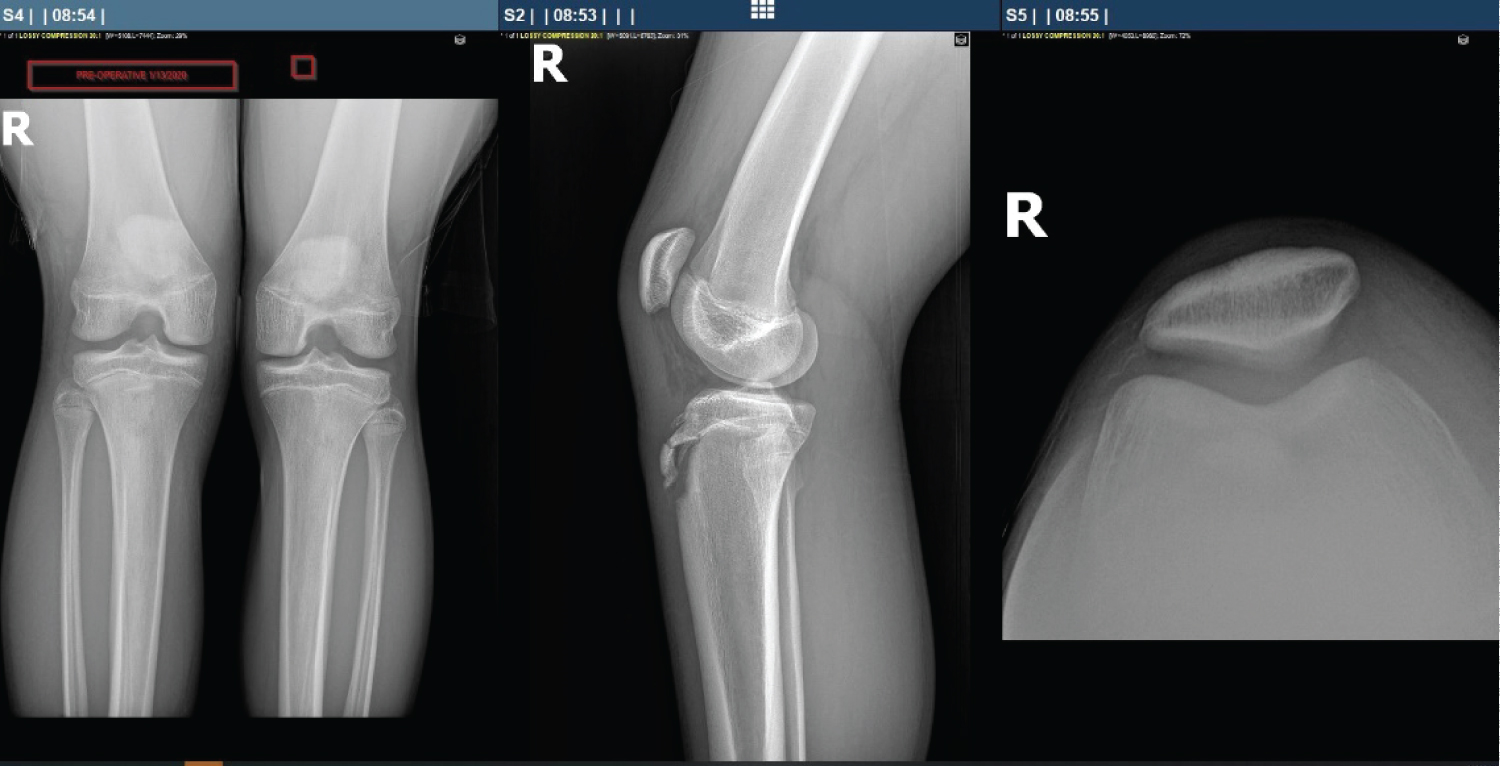
A 13-year-old boy presented with right knee pain and severe swelling following an injury during a basketball game a week prior. The injury was described by the patient as "knee to knee" contact with another player and he was immediately taken out of the game, unable to walk. Upon examination, diffuse tenderness and swelling were present, and the patient was unable to weight bear or extend his right leg. Anteroposterior and lateral radio graphs confirmed right knee displaced avulsion fracture of the tibial tubercle (Figure 1).
For immediate therapy, a knee immobilizer was applied to the right knee and an NSAID and Tylenol with Codeine were prescribed. We scheduled the patient for an open reduction and internal fixation of the right tibial tubercle on the following day.
Surgical Technique
A longitudinal incision was made over the lateral aspect of the tibial tubercle. A combination of sharp, hot, and blunt dissection was carried down to the level of the patellar tendon and tibial tubercle. Small free bony fragments were removed and this area was irrigated. The avulsed tibia tubercle fragment was then provisionally pinned and confirmed to be appropriately reduced radio graphically to access an atomic location. This fracture positioning was then noted and the provisional pinning was removed, allowing for visualization of the proper foot print of the avulsion.
Two proximal 4.75 anchors were positioned in the tibia, at the location of the avulsion bed after drilling, tapping. Sutures were then passed through the bony structure and tendinous insertion of the avulsed tibia tubercle aligning with the anchor placement.
The two distal anchors locations were then drilled and tapped positioned medial and lateral to the tibial tubercle, just distal to the distal end of the avulsed tibia tubercle fragment.
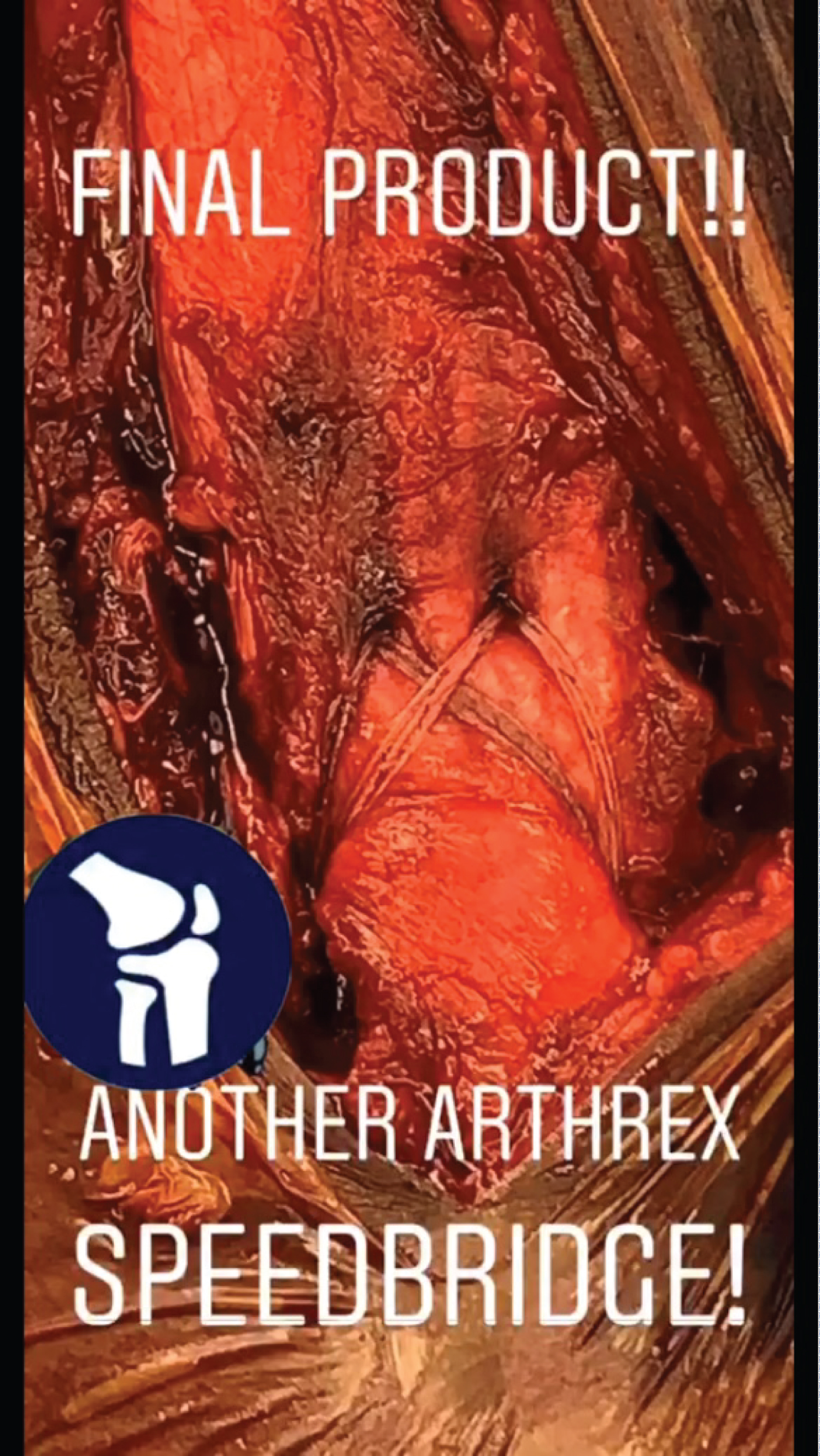
The proximal sutures were then secured to distal anchors in a classic Speed Bridge configuration, tightened and the anchors were then set, securing the patellar tendon, with the avulsed tibia tubercle fragment to the tibia. The intraoperative photo below displays the final product of the surgical repair (Figure 2).
The knee was taken through range of motion, through which excellent compression of the attachment of the patellar tendon was maintained. Radiographs confirmed anatomic reduction and compression of the fracture fragment. The patient was placed in a knee immobilizer postoperatively.
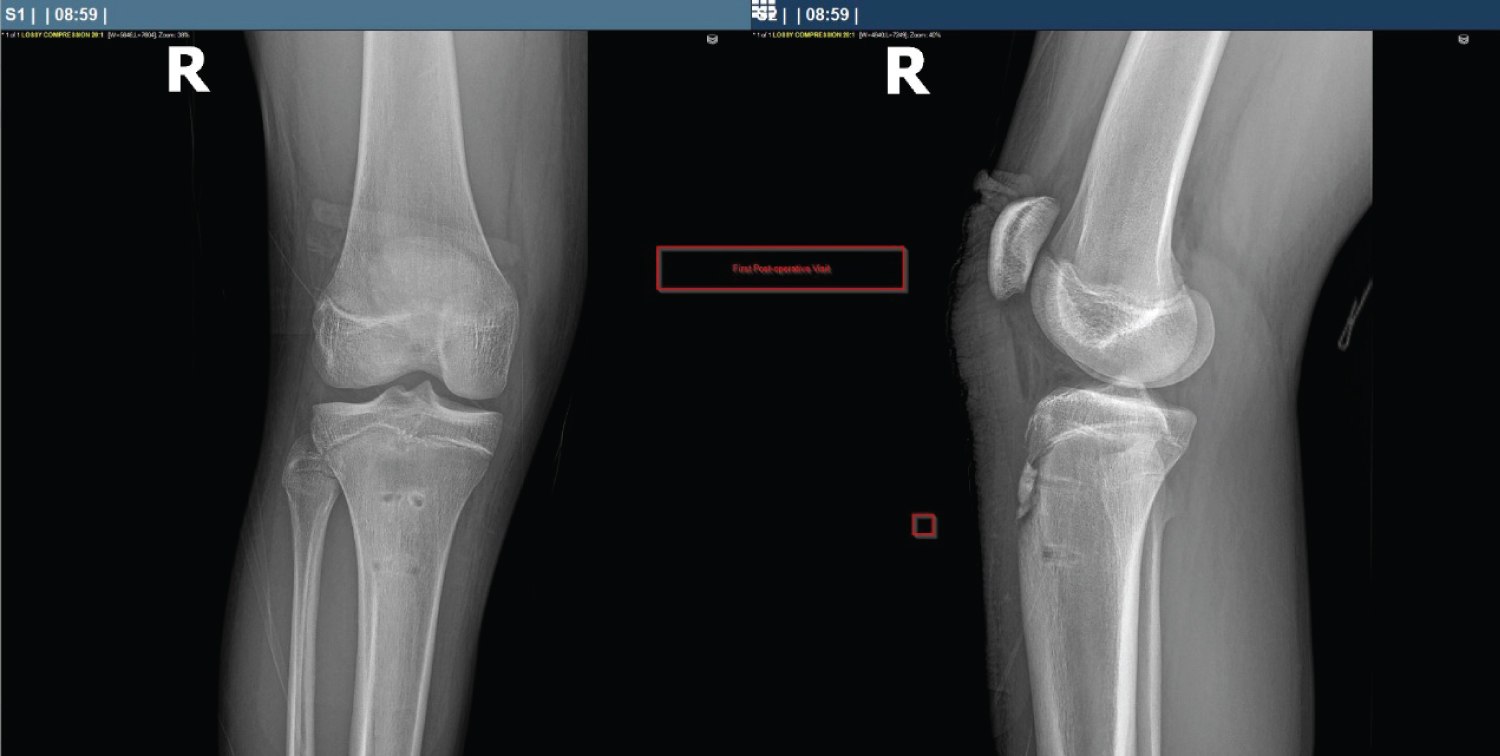
In-clinic radiographs were obtained 8 days postoperatively. These radiographs (anteroposterior and lateral) confirmed stable anatomic reduction and compression of the fracture fragment with healing (Figure 3).
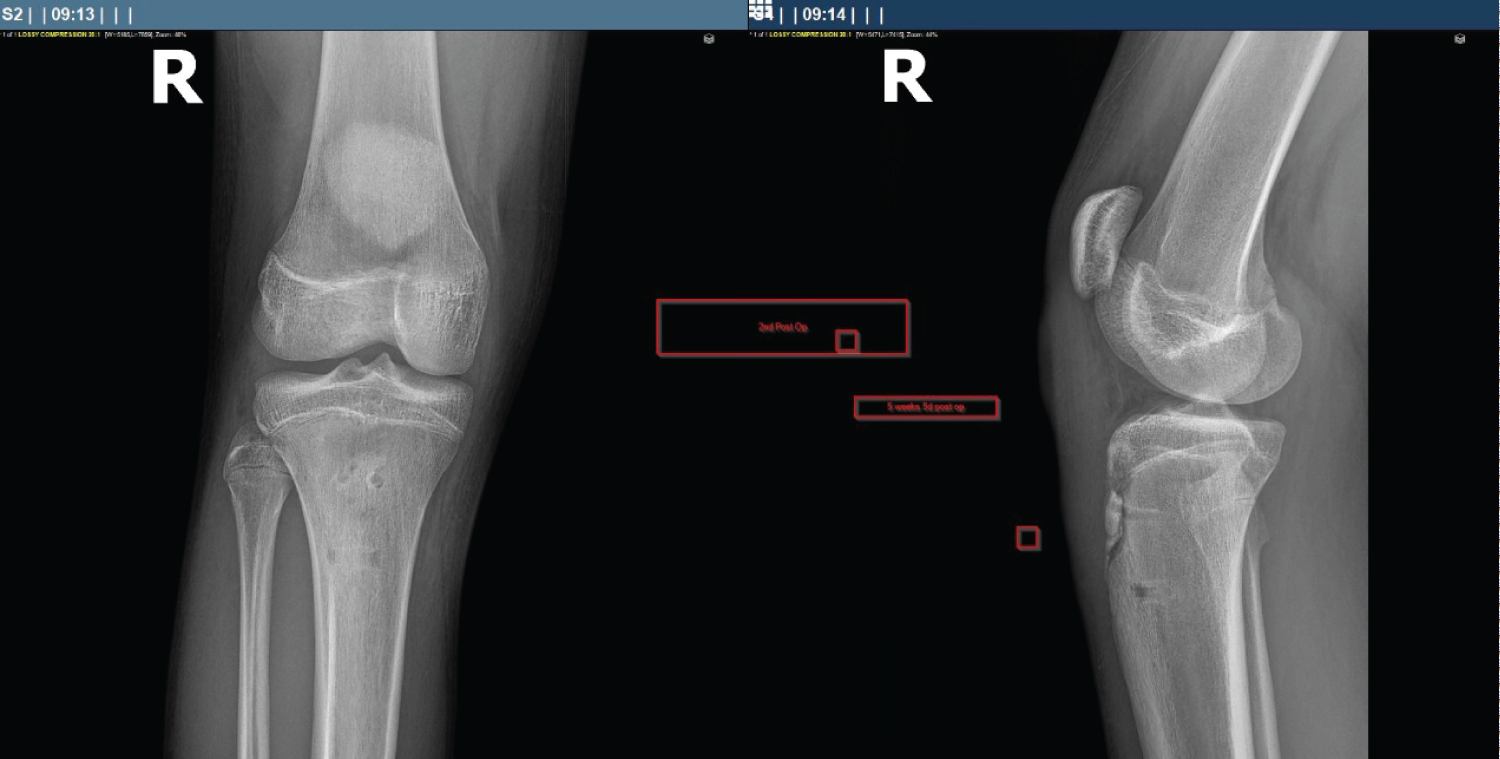
In-clinic X-rays were again obtained 5 weeks and 5 days postoperatively, which again confirmed stable anatomic reduction and compression of the fracture fragment with healing (Figure 4).
Discussion
The avulsion fracture of the tibial tuberosity occurs primarily in adolescent males. Typically, it is seen in jumping sports, most prominently of which, basketball [4]. The exact mechanism involves sudden violent contraction of the quadricep muscle, causing a strong tensile force on the skeletally immature tibia [1]. When the tensile forces of the quadriceps complex against the patellar tendon insertion overcome the cohesive forces within the apophyseal cartilage, an avulsion fracture of the tibial tubercle may occur [5]. The tibial tubercle avulsion fracture is regarded as a substantial injury to the extensor mechanism as the patellar tendon is attached to the tibial tuberosity [6]. As such, an anatomical reduction and stable fixation is required to ensure it heals anatomically. There are three main goals in treating the fracture: To restore the extensor mechanism, to restore a congruent knee joint, and to prevent refracture at the site of injury.
Traditional techniques to repair TTAF necessitate long leg casting for, at minimum, 4-6 weeks following surgical repair. Range of motion is typically not achieved until 4 weeks post-operatively [4]. This leaves the adolescent patient out of sports and regular activity for, on average, 3.9 months [4]. This has a profoundly negative impact on the quality of life of these patients, as the vast majority of them are young, active athletes. Such a length of time without physical activity or sports often culminates in physical, psychological, even emotional harm in these pediatric patients. The all-suture repair technique we describe in this case requires no casting, yields early range of motion, and immediate therapy. Our 13-year-old male patient achieved full extension of his right leg 8 days postoperatively, in stark contrast to traditional methods which yield full range of motion 4 weeks postoperatively [4]. In addition, he was cleared to initiate physical therapy 8 days postoperatively. He was able to return to basketball and other jumping sports with no restrictions just 10 weeks postoperatively. In comparison to traditional methods to repair TTAF, which can necessitate up to 6.5 months of inactivity following surgical repair [4], the method we describe in this case offers a convincing alternative when considering all aspects of the human condition.
References
- Zaizi A, El Yaacoubi T, Chafry B, et al. (2019) Tibial tubercle avulsion fractures in school sports injury: A case report. Int J Surg Case Rep 58: 30-32.
- Nanninga AJ, Josaputra HA (1987) Tibial tuberosity fracture in adolescents - report of a case and review of the literature. Neth J Surg 39: 144-146.
- Joseph T Gamboa, Broc A Durrant, Neil P Pathare, et al. (2017) Arthroscopic reduction of tibial spine avulsion: Suture lever reduction technique. Arthroscopy Techniques 6: e121-e126.
- Frey S, Hosalkar H, Cameron DB, et al. (2008) Tibial tuberosity fractures in adolescents. J Child Orthop 2: 469-474.
- Stevens MA, El Khoury GY, Kathol MH, et al. (1999) Imaging features of avulsion injuries. Radiographics 19: 655-672.
- J Schiller, S DeFroda, T Blood (2017) Lower extremity avulsion fractures in the pediatric and adolescent athlete. The Journal of the American Academy of Orthopaedic Surgeons 25: 251-259.
Corresponding Author
Noah Embry, TCU and UNTHSC School of Medicine, 3500 Camp Bowie Blvd, Fort Worth, 76107, USA
Copyright
© 2020 Embry N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.