Salvage Procedure Salvaged by External Fixation: A Case Report
Abstract
Background
The one-bone forearm is a salvage procedure that can be used in chronic distal radio-ulnar joint instability, therefore sacrificing pronation-supination in order to reduce pain. Failed consolidation is a common complication and associated with several risk factors. Many authors insist on the need for rigid fixation, combining bone grafting, internal fixation and external fixation together when faced with complicated upper-limb reconstruction.
Case presentation
A 56-year-old woman presents chronic right-forearm pain following serious trauma to the distal radio-ulnar joint. Multiple surgical interventions were performed, including a Darrach procedure, extensive resection of the distal ulna, and latero-lateral arthrodesis. Several years later in 2017, considering the persistence of symptoms and the limited amount of alternative solutions, reconstruction using the one-bone forearm salvage procedure was performed. However, consolidation was not successfully achieved until the third retake, when an external fixator was used instead of an above-elbow plaster cast to immobilize the forearm after surgery.
Conclusion
Our hypothesis is that the new biomechanical constraints created in a one-bone forearm can be so high that they exceed the stabilizing capacities of an internal plate and traditional plaster cast, resulting in repeated non-union. Systematic use of an external fixator would therefore ensure optimal consolidation and avoid such complications.
Keywords
One-bone forearm, Distal radio-ulnar joint, External fixation, Forearm non-union, Darrach failure
List of Abreviations
DRUJ: Distal Radio-Ulnar Joint; OBF: One-Bone Forearm
Background
Initially used to treat complicated post-traumatic forearm injuries, the one-bone forearm (OBF) is an unconventional yet effective solution to a variety of complicated situations involving chronic pain and instability of the forearm. Despite acceptable functional and esthetical results [1-3], it remains a salvage technique that should not be the first line of treatment for the simple reason that it eliminates forearm pronation/supination.
This loss of supination/pronation, though seemingly radical at first, is a small sacrifice that restores forearm stability and use of the hand, ultimately improving one’s quality of life. Patients are also able to adapt by using the shoulder joint in order to partially compensate this loss of range of motion [4]. The exact fusion angle is chosen based on the patient’s lifestyle and personal preferences, and cannot be determined by a surgical team alone, despite various recommendations [4].
Failed consolidation of the OBF is a common complication. Peterson, et al. [4] found a primary non-union rate of 32% in 19 patients having undergone either an OBF procedure or radio-ulnar fusion. They were able to identify several factors associated with poor results (including non-union): Traumatic primary pathology, ≥ 2 previous major reconstructive procedures, severe nerve injury, and previous infection. Jacoby, et al. [5] report a similar non-union rate of 37.5% in 8 patients after an OBF procedure, with an average of 4.2 previous procedures for patients with non-union compared to 3.4 for patients with union. They equally suggest that smoking and the type of osteotomy (transverse vs. oblique) could play a role in bone union.
Though several authors emphasize the importance of bone grafting [4], the most important factor for any bone union is correct osteosynthesis. When considering the OBF, Jacoby, et al. [5] conclude that “it is difficult to recommend one form of internal fixation over another because of reports based on small case series, heterogeneous patient populations, and differences in outcome assessment tools”. Our case shows that internal osteosynthesis a lone, even when combined with an above-elbow plaster cast, is not sufficient.
Bessy, et al. [1] insist on the need for rigid fixation with bone grafting, and use an external fixator in combination with internal osteosynthesis techniques in two cases of complex upper member reconstruction. Dell and Sheppard recognize the potential importance of such external fixation, stating that “an external fixator is essential to supplement the recognized marginal internal fixation” [6].
Case Presentation
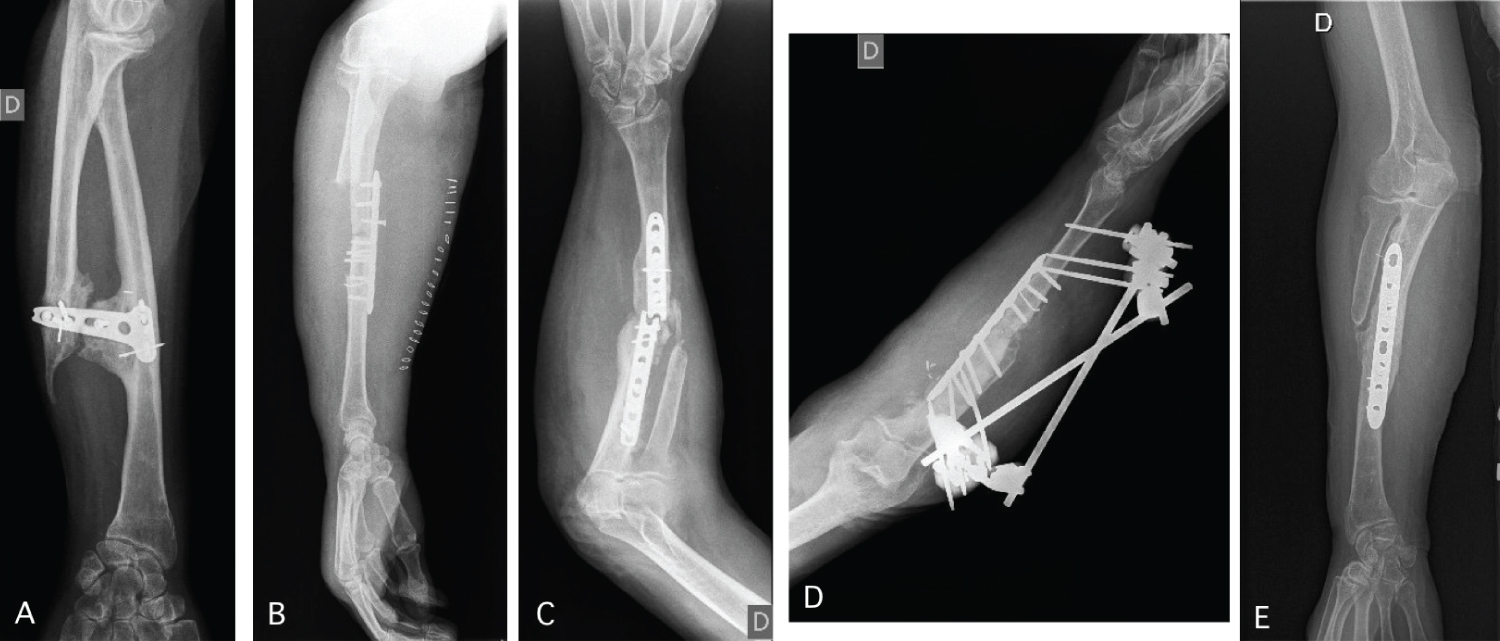
A 56-year-old woman presents chronic right-forearm pain after an aggression resulted in important distal radio-ulnar joint (DRUJ) instability. Following the initial Darrach procedure, she developed painful ulnar impingement and increased forearm instability. Multiple retakes including soft-tissue reconstruction, further ulnar resection, and latero-lateral arthrodesis were unsuccessful (Figure 1A).
Our team was consulted in September 2016 and the one-bone forearm (OBF) salvage procedure was performed in January 2017. Forearm bones were exposed using ananterior Henry approach, the ulnar stump was slightly shortened and the proximal radial diaphysis was partially resected, then the proximal ulna and distal radius was joined end-to-end at 40° of pronation. A compressive plate with 3.5 mm diameter screws ensured solid internal osteosynthesis, cancellous bone graft was packed in the junction, and an above-elbow plaster cast was used for post-operative immobilisation.
One-month later, X-ray images showed no signs of consolidation and significant displacement of the internal hardware (Figure 1B). The same procedure was repeated using a longer plate, but in June 2017, despite continued immobilisation, the internal plate failed following a fall (Figure 1C).
After the third retake, an external fixator was used for more rigid immobilisation. Early signs of consolidation were visible on X-ray images just one month later (Figure 1D) and complete consolidation was achieved by January 2018 (Figure 1E). One year later, the patient is extremely satisfied with the results.
Conclusion
Our hypothesis is that the new biomechanical constraints created by the OBF procedure can be so high that they exceed the stabilizing capacities of an internal plate and traditional plaster cast, resulting in repeated non-union. This is especially true for patients with traumatic aetiology or multiples previous surgical procedures, where bone vascularisation has been compromised by scar tissue. Considering that the OBF is a salvage procedure, most patients belong to this category, therefore we recommend immediate external fixation in all patients.
Declaration of Interests
None.
References
- Bessy H, Leemrijse Th, Cadot B, et al. (1996) La reconstruction des pertes de substance osseuse de l’avant-bras par cubitalisation du radius (one bone forearm) : A propos de six observations. Ann Chir Main Memb Supér 15: 199-211.
- Kim SY, Chim H, Bishop AT, et al. (2017) Complications and outcomes of one-bone forearm reconstruction. Hand (N Y) 12: 140-144.
- Tong CWC, Hung LK, Cheng JCY (1998) Lengthening of a one-bone forearm: a sequel of neonatal osteomyelitis. J Hand Surg Br 23: 453-456.
- Peterson CA, Maki S, Wood MB (1995) Clinical results of the one-bone forearm. J Hand Surg Am 20: 609-618.
- Jacoby SM, Bachoura A, DiPrinzio EV, et al. (2013) Complications Following One-Bone Forearm Surgery for Posttraumatic Forearm and Distal Radioulnar Joint Instability. J Hand Surg Am 38: 976-982.
- Dell PC, Sheppard JE (1984) Vascularized bone grafts in the treatment of infected forearm nonunions. J Hand Surg Am 9: 653-658.
Corresponding Author
Ingrid Tuzi, Faculty of Medicine, Free University of Brussels (ULB), Belgium
Copyright
© 2020 Tuzi I, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.