Effect of Respirable Coal Mine Dust and Quartz on Lung Function Parameters of German Coalminers: A Longitudinal Study 1974-2004
Abstract
Purpose
Poorly soluble low toxic particulates (PSLT) and their particle specific effects on the respiratory system are under review in Europe. We aim to investigate the nature and magnitude of lung function deficits from coal and quartz exposure in coal miners.
Methods
Longitudinal inception cohort study (1974-2004) on miners who started working underground at two coal mines in Germany between 1974 and 1979. From the continuous exposure monitoring, the numbers of the shifts exposed and the shift-average concentration are available, so that long-term average and cumulative concentration of respirable coal dust and quartz component can be derived. The effects of exposure on lung function parameters (FVC, FEV1, FEV1/FVC) were estimated with generalized estimation equation (GEE) models, after adjusting for anthropometric factors, smoking behaviour, and lung function measuring devices.
Results
14,940 lung function tests were performed for 1352 miners during 30 years of follow-up. On average, 11.1 lung function tests were available per miner. Compared to reference values, the averaged FVC, FEV1, FEV1/FVC varied from 95% to 103% at the end of follow-up. GEE-regression models indicated a negative impact of long-term average concentration of respirable quartz dust on FVC (-0.097l/0.1 mg/m3, p < 0.001), as well as on FEV1 (-0.069 l/0.1 mg/m3, p = 0.003).
Conclusions
Negligible decline of lung function resulted from exposure to coal mine dust, while quartz dust concentration showed adverse effects.
Keywords
Coal mine dust, Crystalline silica, Respiratory morbidity, Lung function, Retrospective cohort study, Inception cohort
List of Abbreviations
PSLT: Poorly Soluble Low Toxic Particulates; FVC: Forced Vital Capacity; FEV1: Forced Expiratory Volume in 1 Second; FEV1/FVC: Ratio of Forced Expiratory Volume in 1 Second and Forced Vital Capacity; VC: Vital Capacity; GEE: Generalized Estimating Equation; COPD: Chronic Obstructive Pulmonary Disease; CWP: Coal Workers' Pneumoconiosis; RAG: Ruhr Coal Mine Aktiengesellschaft; BMI: Body Mass Index; L: Liter; GLI: Global Lung Function Initiative
Introduction
Coal mining is amongst the most intensively investigated occupation with respect to dust exposure and health outcomes. The effects of coalmine dust exposure on human health have implication for an array of particles with similar chemical and physical property in respect to the risk assessment and the evaluation of preventive measures. Currently, poorly soluble low toxic particulates (PSLT), such as carbon black, titanium dioxide, and coalmine dust are again the focus of research since European regulation evaluates the particle-specific effect on chronic inflammation, and finally carcinogenicity.
For a long time, the risk of developing lung cancer or pneumoconiosis attributed to coal mine dusts was the major concern, which was extensively studied in United Kingdom, United States of America, and Germany [1-3]. However, additional respiratory diseases, from clinically relevant loss of lung function to chronic obstructive pulmonary disease (COPD), are additional potential hazard of occupational exposure. Longitudinal studies from the British miners [4,5] and the US American miners [6-8] have shown that coal miners suffer a decline in lung function associated with dust exposure.
Enhanced endeavor has been committed from coalmine industry to preventing respiratory diseases, in particular coal workers' pneumoconiosis (CWP), in Germany since decades. Regulations required a standardized medical examination program and document in relation to identified health hazards, i.e. either past or present dust exposure, within the workplace. Within Ruhr Coal Mine AG (RAG), the largest German coal mining company, a comprehensive health protection program is subject to corporate health protection and disease prevention commitments. All miners working underground must undergo a qualification examination at entry to exclude potential risk. During the occupational career, a continuous health surveillance program, including physical examination, lung function tests and chest posterior- anterior radiographs every two years, was provided to prevent developing coal workers' pneumoconiosis and to identify impairment of lung function.
In our previous report based on an inception cohort of RAG, no manifest CWP case was found after 30 years of follow-up [9]. The present study aims to study the risk of lung function impairment from a long-term exposure to coal mine dust, with a follow-up from 1974 through 2004.
Material and Methods
Study design and study population
This study was designed as a retrospective inception cohort study of coal miners working underground. It is a part of an extensive epidemiological study program, which was described more in detail regarding the definition of the cohort, dust measurement, and the collection of medical data including quality assurance [9-11]. Based on this inception cohort, the findings on lung function changes from a follow-up through 1998 [11] and the risk of developing CWP through 2004 [9] were published in previous reports. Here, results concerning the change of lung function from an extended follow-up through 2004 is reported in the present study. The present study is based on 1352 coal miners, who had at least one lung function test. Differences to the former report [9] in respect of coal worker's pneumoconiosis are due to the restriction to the miners with at least one lung function test.
The present analyses are based on an inception cohort consisting of 1352 newly hired coal miners between 1974 and 1979 without prior relevant exposure in two big collieries in the Ruhr area (Heinrich Robertmine and Walsummine) of Germany. The cohort comprises 1369 coal miners (670 in Heinrich Robert and 699 in Walsum), thereof 1352 with lung function measurements. At Heinrich Robert colliery, high rank coking coal was mined which is used in steel production, while at Walsum colliery low rank gas and flaming coal was mined, which is used in energy production. Hence, this study population represents the typical stratigraphic horizons of the coal mined in the Ruhr area.
Dust exposure
Coal mine dust is a mixture of different components due to the geological structure of coal seams. The present study focuses on total respirable coal mine dust and its respirable quartz dust component. RAG (the operator of the two investigated collieries) implemented measures for dust control from the mid-1950s. The dust measurements were carried out gravimetrically with the dust sampling device MPG II [12] reference measuring device that was installed in RAG collieries since 1974 [13]. Dust samples were analyzed by infrared spectroscopy to determine the quartz dust fraction. This made it possible to measure the precise coal mine dust load at a defined workplace as well as its quartz component.
The person-based dust exposure of the coal miners in the study was quantified according to an individual performance record since January 1, 1974. The documentation system of these performance records was adjusted several times during the study period but throughout information about medical examinations, duration and type of employment, fine dust concentrations in the operation and person-related dust exposure values are available. The last version was developed according to the Regulation on Health Protection in Mining [13,14]. These data were used in the shift steering system at RAG to control for the long-term exposure limit value defined by the authorities.
Based on the documentation system at RAG, in which the shift data and performance records were entered, the type, scope and place of employment, 8-h shift average dust concentration for each underground employee was available for the study period from 1974 to 2010. Individual data on the number of underground shifts and the annual average concentration of respirable dusts were extracted. Annual cumulative exposure is a function of the shift average concentration and the number of shifts performed.
Lung function data
The mining regulation of the North Rhine-Westphalian Mining Inspectorate [15,16] and the Regulation on Health Protection in Mining [14] specified occupational health examinations for coal miners. Regulations required a standardized medical examination program and documentation in relation to identified health hazards. Regular physical examination, lung function tests and chest posterior-anterior radiographs every two years, were provided to identify impairment of lung function and to prevent the development of coal workers' pneumoconiosis.
Spirometry has been the standard method to examine the lung function. During the study period from 1974 to 2010, four different devices for lung function measurements were used.
• Bell spirometry [17]
• Wedge Type Spirometer Vitalograph [18,19]
• Oscillo-resistometer/spirometer CustoVit [20,21]
• Jäger's body plethysmograph [22,23]
The use of various devices was recorded longitudinally. The changes of staff members in a lung function measuring team at the Heinrich Robert mine was also documented as a potential influencing factor. For assuring the comparability of the measurements within a measurement team, internal trainings (separately in the two mines) and regular department meetings were organized. The spirometric devices were calibrated on a daily basis. Since approximately 1990, body plethysmographs have been introduced, with additional support of computer for the purpose of quality control. Before the spirometric data was entered into our data set, a team of trained occupational health physicians reviewed the data and categorized each measurement to one of four categories (not usable/normal finding/borderline pathological finding/pathological finding). For discrepancy of the review results, a consensus was reached among the participating physicians according to the criteria. Thus, each categorization represents an expert decision. Furthermore, plausibility of the data were checked with programs. Any non-plausible findings were reviewed timely by the physicians [10].
A total of 14,940 lung function tests were performed for the study population. When using bell spirometry, only vital capacity (VC) could be measured. Sub-group analyses including 14,062 lung function tests, after excluding the 878 measurements using the bell spirometry, are reported with respect to lung function profiles. The following lung function parameters were selected for the analyses [21]:
• Maximal value of vital capacity (VCmax): Maximum of either forced vital capacity (FVC) or in the case of measurement with a dry spirometer, the vital capacity (VC) measured in liter (L).
• Forced expiratory volume in 1 second (FEV1): Measured in L.
• Relative capacity in 1 second, the ratio calculated from forced expiratory volume in 1 s and forced vital capacity (FEV1%VCmax), measured in percentage (%).
The individual decline of lung function parameters was assessed in a longitudinal manner. In addition, the most recent available lung function measurement was compared to the reference value in a cross-sectional manner.
Data on confounding factors
The basic anthropometric data of body weight and height, and information on smoking behavior were collected from all study participants. Data on smoking status and pack-years are based on self-report of the miners during the medical examinations. Missing data for smoking were imputed according to the rule of "last observation was carrying forward" for the years without an examination. The miners are classified into active smokers, former smokers, and never smokers. Two different coal types, coking coal comparing to gas and flaming coal, from the involved coal mines was adjusted in the regression models. Thus, a potential clustering effect across the mines was considered.
Statistical analyses
Two different reference values based on general population [24,25] are calculated based on gender, age, height, and nationality for each participant and year. In the cross-sectional analysis, we compare the last available examination of lung function parameters with these external reference values. Additionally, yearly and age-specific mean values of the measured and predicted values and of their quotients are calculated.
With respect to the changes of the lung function parameters over time, generalized estimating equations (GEE) models are used to estimate the effect of dust exposure. GEE models take the correlation between the repeated intra-individual measurements into account [26,27]. We applied an exchangeable working correlation matrix as an underlying correlation structure. The models are adjusted for the following potential confounding factors: height, weight, age, the lung function measuring device, year of measurement, nationality (German or other), smoking status, and cumulative pack-years. Age was additionally classified into two group (> 25 years or ≤ 25 years), and entered separately into the model to account for the non-linear age effect on lung function parameters as described in Quanjer, et al. [24] and GLI [25].Covariates were selected depending on their significance: all variables that had a significant effect (p ≤ 0.05) in at least one model (i.e. on one of the relevant lung function parameters and in one of the two approaches) were included into all GEE models in order to attain comparability of all models.
In order to estimate the effect of exposure to respirable coal mine dust or respirable quartz, two approaches are used: (i) Cumulative dust exposure; (ii) Long-term average dust exposure in combination with exposure duration were considered in the models, respectively in linear or logarithmic form.
All calculations were performed using the Stata Version 13 [28] statistics package. A statistical significance level of 5% is applied throughout our analyses.
Results
Characteristics of the present inception cohort are summarized in Table 1a, restricted to the 1352 coal miners with lung function measurements after exposure onset. At the beginning of follow-up, the study subjects were in average 20.4 years old. Almost 31% and 68% of the miners have reported to be active and never smokers, respectively. The smoking status have changed during the follow-up, so that respectively 50%, 24%, and 26% of the miners reported to be active, former, and never smokers at the end of the follow-up.
Dust exposure
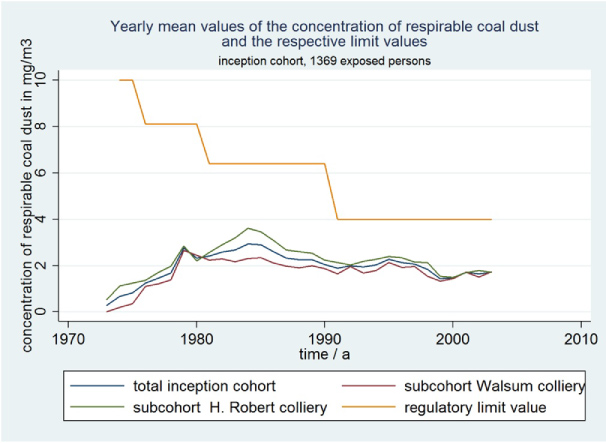
Statistical measures of personal long-term average concentration, exposure duration, and cumulative exposure to respirable coalmine dust and respirable quartz component are summarized in Table 1b. The average duration of exposure to respirable dust was 17.1 dust-years (where a dust-year is defined to be 220 shifts with dust exposure). The long-term average concentration of exposure to respirable coalmine dust and quartz was respectively 2.34 (sd = 0.65) and 0.09 (sd = 0.03) mg/m3 at the end of exposure, while two individuals exceeded the exposure level of 4 mg/m3. The cumulative exposure to respirable coalmine dust and quartz was respectively 37.0 (sd = 19.7) and 0.99 (sd = 0.67) mg/m3-years on average.
Temporal trends of yearly average dust concentrations are demonstrated according to the coalmines and total cohort in Figure 1, with comparison to the occupational exposure limit values over time. The average exposure level started from a low level at the beginning of the follow-up. A peak exposure level below 4 mg/m3was observed in the mid 80's, followed by a steady downward trend with less volatility after 2000.
Lung function
Totally, 14,940 lung function tests had been performed among the 1,352 study participants during an average of 19.6 years of follow-up, which is in accordance with a desired examination frequency of every two years for each miner. Different lung function measuring devices have been applied over the follow-up period. Among the total measurements, 6,913 (49%), 3,218 (30%), and 3,931 (26%) lung function tests were performed respectively with Vitalograph, Custo Vit, Body plethysmograph, while only 878 (6%) measurements were performed with bell spirometry from 1974 to 1978.
Results from the cross-sectional analyses of the last available lung function examination at the end of follow-up are summarized in Table 2. Lung function parameters in relationship to the predicted values are presented respectively according to Quanjer, et al. [24] and Global Lung Function Initiative approach, GLI [25]. Based on GLI approach, the average relative lung function parameters, FEV1, VCmax, and FEV1/VCmax, ranged from 95% to 99%, while the results based on Quanjer, et al. [24] approach were numerically higher, ranging from 100% to 103%.
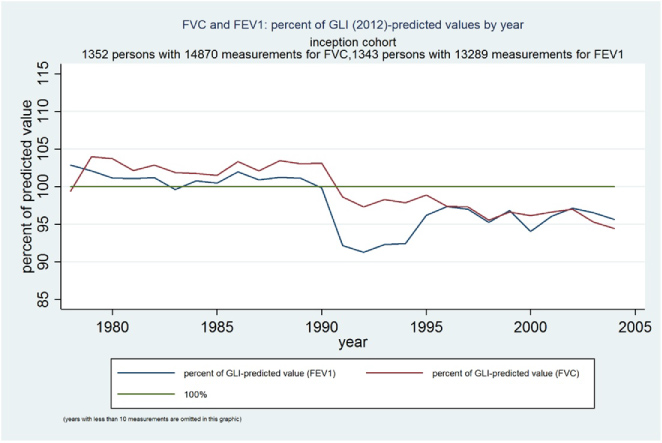
Figure 2a displays the course of the averaged quotients (FEV1 and VCmax) according to the calendar years. In Figure 2b the same quotients are displayed separately by lung function measurement device, which demonstrates the pronounced influence of the measuring devices on the result.
In longitudinal analyses, the effects of dust exposure on the long-term change of lung function were estimated with GEE models. The linear function of exposure measures met better the assumption of normal distribution than the logarithmic transformed exposure measures; we focus the results handling exposure measures in a linear scale.
With approach 1, the effect of cumulative exposure to coal mine dust was estimated. Statistically significant effect was found with respect to VCmax (-0.002 liter per mg/m3.years of coalmine dust, p = 0.074), while no significant effect on FEV1 and FEV1/VCmax was found (Table 3a).
With approach 2, long-term average concentration in combination with exposure duration, on a linear scale, were included at the same timein the regression models (Table 3b). Both long-term average concentration of coalmine dust and exposure duration showed a non-negative impact on VCmax, FEV1, and FEV1/VCmax with no statistical significance. Declining lung function parameters were significantly associated with increasing age, both for the age groups below and over 25 years.
Analogously, the impact of respirable quartz dust were estimated with GEE models, respectively with approaches 1 and 2. Table 4a summarizes the risk estimates of cumulative exposure, which does not show a negative association with VCmax and FEV1, as well as non-significant association with FEV1/VCmax.
In contrast, long-term average concentration of respirable quartz dust showed statistically significant negative impact on VCmax and FEV1. Table 4b summaries the risk estimates with approach 2, every 0.1 mg/m3 increase of quartz dust concentration was indicated to be link with 0.097-liter loss of VCmax, as well as 0.069-liter loss of FEV1.
Discussion
We evaluated the relationship between exposure to coalmine dust containing quartz and long-term lung function loss in a German inception cohort of coal miners. As compared to external reference values, lung function of the participants was unexceptional at the end of follow-up. Although a qualitative assessment was not foreseen in the study plan, prevalence of an obstructive patter (FEV1 / FVC < 70% and FEV1 < 80% of predicted value) was elevated from 6.3% at the beginning to 9.0% at the end of the follow-up. GEE regression models were used to estimate the impact of exposure to respirable coal mine dust and its quartz fraction on lung function, after adjusting for biological aging effect and other relevant confounders. No statistically significant negative effect of exposure to coal mine dust on FEV1 and FEV1/VCmax could be determined. Despite of marginally statistical non-significance, an estimate of -0.002 liter per mg/m3.year of coalmine dust on loss of VCmax would imply a loss of 75 ml of VCmax totally, provided an average cumulative exposure to coalmine dust of 37.41 mg/m3.years. Meanwhile aging showed consistently negative impact on VCmax and FEV1, would a decline of approximately 30 ml. The results from our models showed that even increments of age below 25 years have a negative impact on lung function, which is contrary to the normal age course of lung function. This could be resulted from a collinear relationship between age and cumulative exposure, and age appears to have captured largely the impact of exposure on lung.
Comparing the long-term average concentration (0.09 mg/m3) with the current occupational exposure limit value (OEL) (0.05 mg/m3) for quartz in Germany, loss of 44.5 ml on VCmax or 31.6 ml on FEV1 would be prevented if the OEL had been complied with during an average exposure of 11.46 quartz-years.
The relationship between coalmine dust and decline of lung function has been reported in numerous cross-sectional studies [5-7,29-32]. Since results from cross-sectional studies without considering temporal order have potential for bias, two longitudinal studies were conducted to address this relationship in the British and Australian cohorts [4,33]. The findings of this inception cohort study are not consistent with that from these cohorts. Apart from the methodological limitations of these studies, such as secondary selection and lack of statistical power, the magnitude of the dust exposure was much higher than that of the present cohort since the 70's. A straightforward comparison between the studies would be difficult [34].
Very few existing longitudinal studies involving repeated measurements provide an insight of profile of lung function over time. Two previous studies [8,35] reported an early impairment pattern observed in the US and the Chinese coal miners. In the US study, a rapid initial decline was indicated between two measuring points, comparing the FVC and FEV1 prior to and post the cross-sectional examination around 1972-1975, while no additional loss of lung function related to dust exposure could be detected during the following 15 years. The Chinese study reported a longitudinal observation of 15 repeated lung function tests within 36 months. A rapid decline of FEV1 of 0.12l was observed for those aged over 20 years during the first 12 months, while the impact of exposure to coal mine dust (-0.0002l per mg/m3, p = 0.3033) was almost negligible in the regression model comparing to the effect estimates of age and group. Comparing with our study with a regular examination every two years over 30 years of follow-up, the Chinese study is advantageous because of much more frequent measurements within a short time period, while the US study compared the changes from the measurement at two time points.
A longitudinal observation of the lung function parameters from 1974 to 1998 based on the present inception cohort was reported in previous publications, with focus on the risk assessment of nitrogen oxides [34,36,37]. From these previous analyses based on the same inception cohort, nitrogen oxides did not show noticeable negative impact on any lung function parameters. Therefore, the impact of nitrogen oxides are not taken into account in the present analysis. The present study with extended follow-up through 2004 is consistent with the former reports [10,11,34,36,37]. The risk estimates of quartz concentration came out to be significantly positive on VC and marginally significant on FEV1.
An apparent decline of lung function in 1990 was noticeable in the present cohort. This finding can be the result from: 1) An artefact resulting from the change of measuring devices; 2) A biasing effect due to selection because healthier miners exited from the cohort; 3) True lung function impairment after 15 years of exposure. To check the possible artefact from change of measuring devices, we studied the profile of lung function, grouped according to the measuring devices (refer to Figure 2b). Only 878 lung function tests were performed with bell spirometry from 1974 to 1978. The average FVC for this time period varied between 80% and 85% of predicted value. This finding is not plausible because a primary healthy-worker-effect, i.e. the healthier employees are more likely to be selected into the work force, would be expected from an occupational cohort at the beginning of the exposure [38]. The majority of tests were performed with Vitalograph, whose test results varied from 102% to 109%, which application was abandoned in 1990. Afterwards, Custovit and Body plethysmograph were the major measuring devices since the 90's, which test results were relatively stable over time. The favorable status before the 90's could be a result both from the primary healthy-worker-effect and from the overestimation of Vitalograph readings. The recorded lung function measuring devices showed significant impact on the lung function profile (cf. Figure 2b) in addition to measurement errors. This observation stresses again considering the process of data collection and particularly recording the evolution of measurement devices and techniques during the long-term course of follow up, in order to avoid misinterpretation of data [39,40]. To assure the maximal comparability of the measurements, physicians and technicians of the occupational health departments were trained for quality management.
A secondary selection occurring during the long-term follow-up [41], either the young or the healthier miners exited from the cohort earlier because of downsizing policy or the unhealthier miners left because of deteriorated health status, might result in a biasing effect. Unfortunately, the reasons for an exit from the cohort were not reliably documented; the biasing effect is, therefore, difficult to be estimated. We checked tentatively in two respects. First, the duration of follow-up approximates the duration of employment (Table 1), we believe that the end of employment, either scheduled retirement or downsizing of workforce, are the major reasons for an exit. Furthermore, we compared tentatively the subgroups of those miners with total exposure duration less than 15 years and the latest exit in 1990 (N = 235) with the remaining cohort (N = 1108) who would have dropped out in 1990 hypothetically. The lung function parameters did not seem to differ systematically. Thus, the censoring status did not seem to be associated with health status.
For exposure assessment, on-going stationary dust measurements were assigned to individual miners. Stationary samplers are considered inferior for measuring a worker's exposure than personal samplers, because the concentration of the respirable dust in the breathing zone of the worker is the relevant parameter for health effect. Dahmann and co-workers discussed the strength and weakness of the personal and static samplers for exposure assessment to silica dust in epidemiological studies [42]. The authors pointed out that the personal samplers usually have considerably lower suction rates than static samplers do, although both suction rates model the human breathing physiology. The influence of the measurement strategies was evaluated by comparing the US (personal) and German (static) samplers by simultaneous sampling. Higher average concentration of the respirable quartz with static sampler was found than that with personal samplers [43].
Information on smoking status and pack-years was based on self-reporting at each medical examination throughout the follow-up period. Both qualitative and quantitative smoking behavior are incorporated into the GEE model in a time-dependent manner, and showed significant impact on lung function profiles. Fletcher and Peto [44] studied the natural history of chronic airflow obstruction in a male cohort, and found that FEV1 falls gradually over a lifetime. Quitting smoking might contribute to slowing down the deteriorating effect. This finding is supported by the results from the Framingham offspring cohort [45]. Considering the dynamic changes of smoking behavior rather than the information on a given time point represents to be a strength of the study.
Additional strengths of this study are the unique study base of an inception cohort being free of relevant exposure prior to study begin, accompanied with regular dust exposure measurements and repeated medical examinations in approximate 2 years interval for over 30 years. In RAG, a dose-based concept for dust control, based on the cumulative exposure, has been implemented throughout their collieries since 1974. This concept foresees that miners with exposure to respirable dusts must not exceed a limit value for cumulative exposure to respirable dust evaluated for each miner over an assessment period of 2 years. For more details of this dust control and health surveillance program, please refer to Bauer [13] and Yong, et al. [9]. These findings from the well-established epidemiological coal miner cohorts shed light onto the current issue in terms of exposure to poor soluble low-toxic (PSLT) particulates and non-malignant respiratory diseases.
Conclusion
Negligible decline of lung function resulted from exposure to coal mine dust, while quartz dust concentration showed adverse effects in the present study. Divergent findings to that of the older studies could be explained partly by different study designs (here: longitudinal studies, no prior exposure), but also by lower dust levels. Stringent dust control measures and health surveillance program might contribute to prevent the respiratory disease.
Declarations
Ethics approval and consent to participate
This study is approved from the ethics committee of the University of Cologne, Germany.
Consent for publication
This manuscript does not contain any individual person's data in any form.
Availability of data and material
The data of the present study are not accessible publicly.
Competing interests
The authors declare no competing interests. PM, RD, HL are former employees of RAG. The design, conduct, analysis, and conclusions of the study are exclusively those of the authors.
Funding
This study is funded by a research contract with Ruhr Coal Mine AG (RAG). PM, RD, HL are former employees of RAG. The design, conduct, analysis, and conclusions of the study are exclusively those of the authors.
Authors' contributions
Study design and study conduction: PM, HL, RD; Statistical analysis and results interpretation: MY, LA, PM; Drafting and reviewing of the manuscript: MY, LA, HL, RD, PM.
Acknowledgements
We wish to thank the whole team from the department of occupational medicine in RAG for their continuous commitment to dust control and health protection for the past decades and their support in this study. The complete list of occupational physicians, industry hygienists, and statisticians who have contributed to this work is too long for listing.
References
- Graber JM, Stayner LT, Cohen RA, et al. (2014) Respiratory disease mortality among US coal miners; results after 37 years of follow-up. Occup Environ Med 71: 30-39.
- Miller BG, MacCalman L (2010) Cause-specific mortality in British coal workers and exposure to respirable dust and quartz. Occup Environ Med 67: 270-276.
- Morfeld P, Lampert K, Emmerich M, et al. (2002) Staubexposition, Pneumokoniose und Lungenkrebs: Eine epidemiologische Studie aus dem Saarländischen Steinkohlenbergbau. Zbl Arbeitsmed Arbeitsschutz Ergon 52: 382-397.
- Love RG, Miller BG (1982) Longitudinal study of lung function in coal-miners. Thorax 37: 193-197.
- Marine WM, Gurr D, Jacobsen M (1988) Clinically important respiratory effects of dust exposure and smoking in British coal miners. Am Rev Respir Dis 137: 106-112.
- Attfield MD (1985) Longitudinal decline in FEV1 in United States coalminers. Thorax 40: 132-137.
- Attfield MD, Hodous TK (1992) Pulmonary function of US coal miners related to dust exposure estimates. Am Rev Respir Dis 145: 605-609.
- Seixas NS, Robins TG, Attfield MD, et al. (1993) Longitudinal and cross sectional analyses of exposure to coal mine dust and pulmonary function in new miners. Br J Ind Med 50: 929-937.
- Yong M, Anderle L, Lenaerts H, et al. (2018) The risk of developing coal workers' pneumoconiosis in a German inception cohort of Coal Miners of Ruhr area - results after 30 Years of follow-up. Ann Lung Cancer 2: 39-47.
- Morfeld P, Ambrosy J, Bengtsson U, et al. (2001) Aufbau einer epidemiologischen Studie zur Auswirkung von untertägigen Belastungen im Steinkohlenbergbau auf die Lungenfunktion und das Vorliegen einer Pneumokoniose im Röntgenbild bei Steinkohlenbergleuten. Atemw-Lungenkrkh 27: 407-409.
- Büchte SF (2007) Epidemiologie als Werkzeug zur Erfolgskontrolle für die Begrenzung der Staubbelastung im Steinkohlenbergbau an der Ruhr für den Zeitraum 1974-1998. Fakultät für Energie- und Wirtschaftswissenschaften der Technischen Universität Clausthal.
- Wazau G (1973) Bedienungsanleitung zum Staubmeß- und Probenahmegerät MPG II System SFI/IGF. Berlin: Dr.-Ing. Georg Wazau Mess- und Prüftechnik.
- Bauer HD (1995) BIA-Report 7/95. Staubjahre. Möglichkeiten ihrer Ermittlung unter Einbeziehung unerschiedlicher Meßsysteme und Verfahren der Arbeitseinsatzlenkung-Bearbeitungshinweise. Sankt Augustin: Hauptverband der gewerblichen Berufsgenossenschaften (HVBG).
- Ges Berg V (1991) Gesundheitsschutz-Bergverordnung vom 31. Juli 1991(BGBl. I S. 1751), die zuletzt durch Artikel 5 Absatz 6 der Verordung vom 26. November 2010 (BGBl. I. S. 1643) geändert worden ist. Bundesminister für Wirtschaft, Berlin.
- BVOSt (1970) Bergverordnung des Landesobergbergamts Nordrhein-Westfalen für die Steinkohlenbergwerke. Landesoberbergamt Nordrhein-Westfalen, Dortmund.
- BVOSt (1986) Bergverordnung des Landesobergbergamts Nordrhein-Westfalen für die Steinkohlenbergwerke vom 20. Landesoberbergamt Nordrhein-Westfalen, Dortmund.
- Bartels H, Bücherl E, Hertz CW, et al. (1959) Lungenfunktionsprüfungen. Methoden und Beispiele klinischer Anwendung. Springer-Verlag, Berlin.
- Vance JW (1963) A bellows-type spirometer for measuring the forced expirogram. Chest 43: 57-61.
- (1973) Vitalograph: Lungenventilationsmessung - ein einfaches Verfahren. Ein Handbuch zur Untersuchung der Ventialtionsfähigkeit mit dem Vitalograph-Keilbalgspirometer. Vitalograph Ltd., Buckingham.
- Pleger E, Müller E, Frank W, et al. (1991) Die Oszillationsmethode - eine kostengünstigere Alternative für die atemmechanische Funktionsdiagnostik in der Praxis? Z Arztl Fortbild 85: 187-192.
- Ulmer WT (1998) Lungenfunktions-manual. Georg Thieme Verlag, Stuttgart.
- Fruhmann G, Woitowitz HJ (1997) Chronisch-obstruktive bronchitis und lungenemphysem. Dtsch Arztebl 94: 192-193.
- Ulmer WT, Bengtsson U, Reischig HL (1991) Lungenfunktionswerte bei bergarbeitern in der bundesrepublik deutschland. Kompaß 13-6.
- Quanjer PH, Tammeling GJ, Cotes JE, et al. (1993) Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests, European community for steel and coal. Official statement of the European respiratory society. Eur J Respir Dis 6: 5-40.
- Global lung function initiative.
- Diggle PJ, Liang KY, Zeger SL (2000) Analysis of longitudinal data. In: Atkinson AC, Copas JB, Pierce DA, Schervish MJ, Titterington DM, Oxford statistical science series 13. Oxford University Press Inc., New York.
- Liang KY, Zeger SL (1986) Longitudinal data analysis using generalized linear models. Biometrika 73: 13-22.
- (2014) StataCorp. Release 13. Statistical software. College Station, StataCorp LP, TX.
- Hnizdo E, Vallyathan V (2003) Chronic obstructive pulmonary disease due to occupational exposure to silica dust: A review of epidemiological and pathological evidence. Occup Environ Med 60: 237-243.
- Jacobsen M (1993) Pulmonary function of US coal miners related to dust exposure. Am Rev Respir Dis 148: 257.
- Rogan JM, Attfield MD, Jacobsen M, et al. (1973) Role of dust in the working environment in development of chronic bronchitis in British coal miners. Br J Ind Med 30: 217-226.
- Seixas NS, Robins TG, Attfield MD, et al. (1992) Exposure-response relationships for coal mine dust and obstructive lung disease following enactment of the federal coal mine health and safety act of 1969. Am J Ind Med 21: 715-734.
- Leigh J (1990) 15 year longitudinal studies of FEV1 loss and mucus hypersecretion development in coal workers in New South Wales, Australia. VIIth Int Pneu Conf 1988. Pittsburgh, 112-121.
- Morfeld P, Noll B, Büchte SF, et al. (2010) Effect of dust exposure and nitrogen oxides on lung function parameters of German coalminers: A longitudinal study applying GEE regression 1974-1998. Int Arch Occup Environ Health 83: 357-371.
- Wang ML, Wu ZE, Du QG, et al. (2007) Rapid decline in forced expiratory volume in 1 second (FEV1) and the development of bronchitic symptoms among new Chinese coal miners. J Occup Environ Med 49: 1143-1148.
- Morfeld P, Noll B, Büchte SF, et al. (2009) Einfluss von Staubbelastung und Stickoxiden auf Lungenfunktionsparameter von Steinkohlenbergleuten an der Ruhr - Eine Längsschnittstudie mit GEE-Regressionsmodellen, 1974-1998/Teil I. Kompass 119: 4-11.
- Morfeld P, Noll B, Büchte SF, et al. (2009) Einfluss von Staubbelastung und Stickoxiden auf Lungenfunktionsparameter von Steinkohlenbergleuten an der Ruhr - Eine Längsschnittstudie mit GEE-Regressionsmodellen, 1974 - 1998/Teil II. Kompass 119: 8-15.
- Arrighi HM, Hertz-Picciotto I (1993) Definitions, sources, magnitude, effect modifiers, and strategies of reduction of the healthy worker effect. J Occup Med 35: 890-892.
- Rothman KJ, Greenland S, Lash TL (2008) Modern epidemiology. (3rd edn), Lippincott Williams & Wilkins, Philadelphia.
- Cameron AC, Trivedi PK (2005) Microeconometrics. Methods and applications. University Press, Cambridge.
- Checkoway H, Pearce N, Kriebel D (2004) Research methods in occupational epidemiology. (2nd edn) Oxford University Press, Oxford.
- Dahmann D, Taeger D, Kappler M, et al. (2008) Assessment of exposure in epidemiological studies: the example of silica dust. J Expo Sci Environ Epidemiol 18: 452-461.
- Büchte SF, Burggraf C, Langefeld O, et al. (2004) Comparative dust sampling program of respiable coal mine dust concentrations taken during 2002 at US coal mines applying German and American dust sampling strategies. Tijdschrift voor toegepaste Arbowetenschap 2: 77-78.
- Fletcher C, Peto R (1977) The natural history of chronic airflow obstruction. Br Med J 1: 1645-1648.
- Kohansal R, Martinez-Camblor P, Agusti A, et al. (2009) The natural history of chronic airflow obstruction revisited: An analysis of the Framingham offspring cohort. Am J Respir Crit Care Med 180: 3-10.
Corresponding Author
Dr. Mei Yong, PD, Institute for Occupational Epidemiology and Risk Assessment of Evonik Industries AG, Rellinghauser Straße 1-11, 45128 Essen, Germany, Tel: +49-201-177-4400, Fax: +49 201-177-4403.
Copyright
© 2019 Yong M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.