Complicated Morgagni Hernia, Cardiac Tamponade, a Series of Unfortunate Events in the Same Patient: Case Report
Introduction
Congenital diaphragmatic hernia of Morgagni-Larrey is an uncommon entity that usually presents on the right side. It accounts for only 3% of all diaphragmatic hernias. These hernias, occurring in the anterior midline through the sternocostal hiatus of the diaphragm, are usually discovered incidentally when the patient has reached adulthood, or when they become symptomatic due to intestinal involvement (occlusive symptoms) or when respiratory dysfunction occurs [1].
Case Presentation
An 80-year-old patient with a history of asthma and high blood pressure attended the emergency room due to a 72-hour history of intestinal obstruction. On physical examination, he was haemodynamically stable, he presented abdominal distension, tympany to percussion, high-pitched bowel sounds and he also presented an inguinal hernia without signs of complications.
Diagnostic Testing
Emergency blood tests
Emergency blood tests showed an elevation of acute phase reactants, as well as normality of lactate in arterial blood gas.
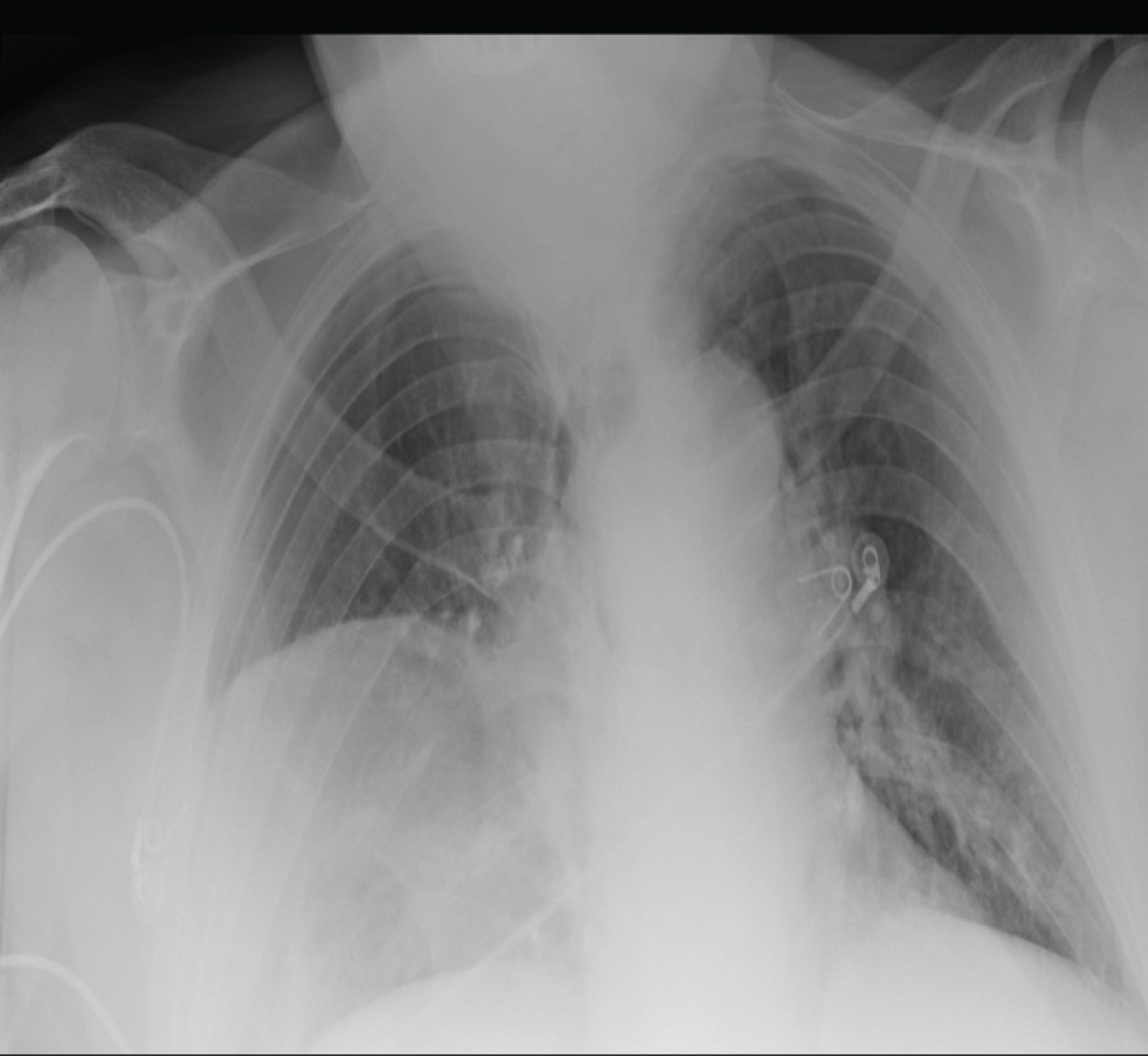
Emergency room chest X-ray; showed elevation of the right hemidiaphragm (Figure 1).
CT
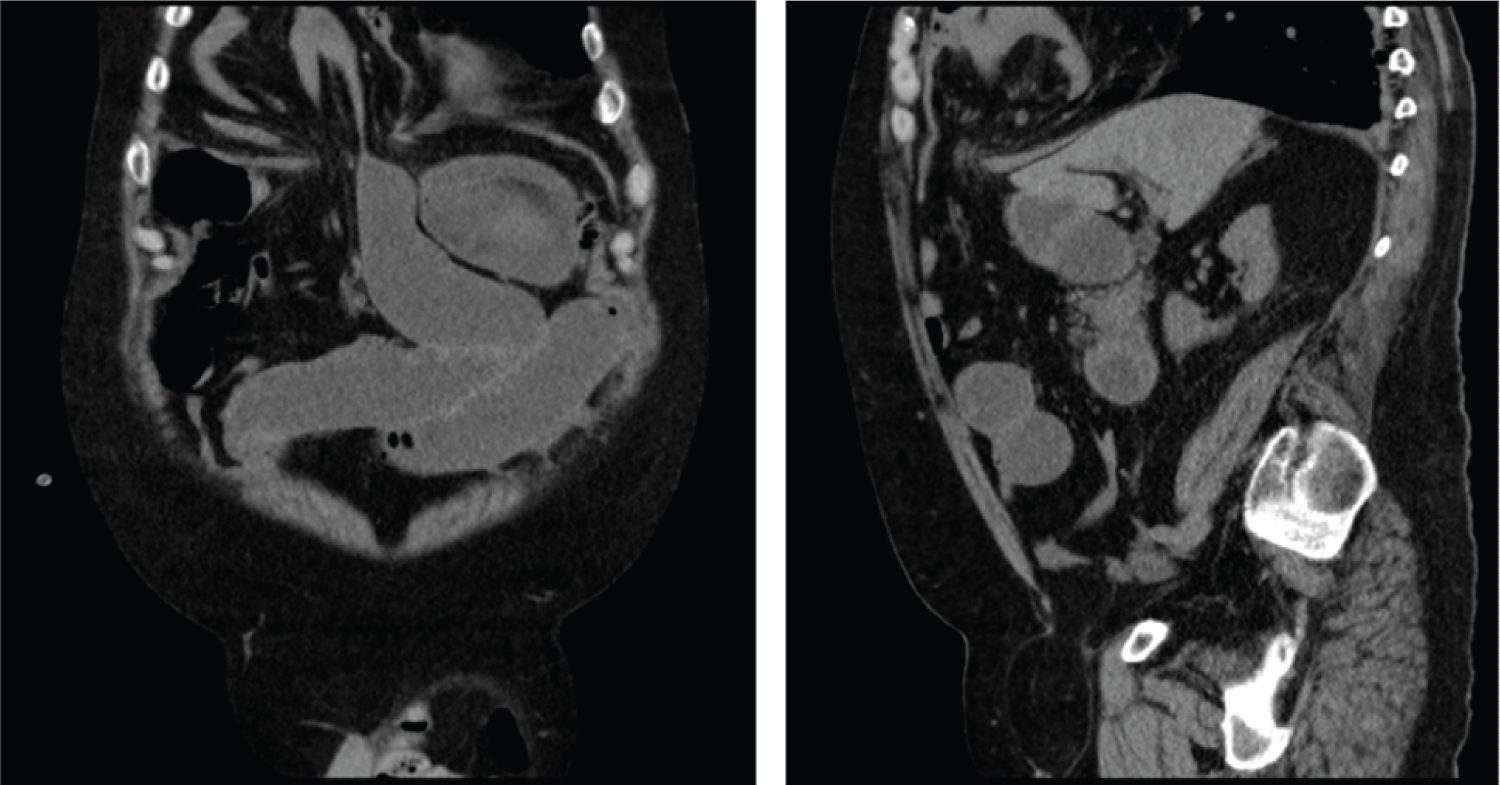
Anterior diaphragmatic hernia in the right hemithorax complicated with obstructive symptoms of the small intestine, with a change in caliber in the jejunal loop, which conditions severe retrograde dilation (Figure 2 and Figure 3).
Due to the findings, urgent surgical management was decided.
Treatment
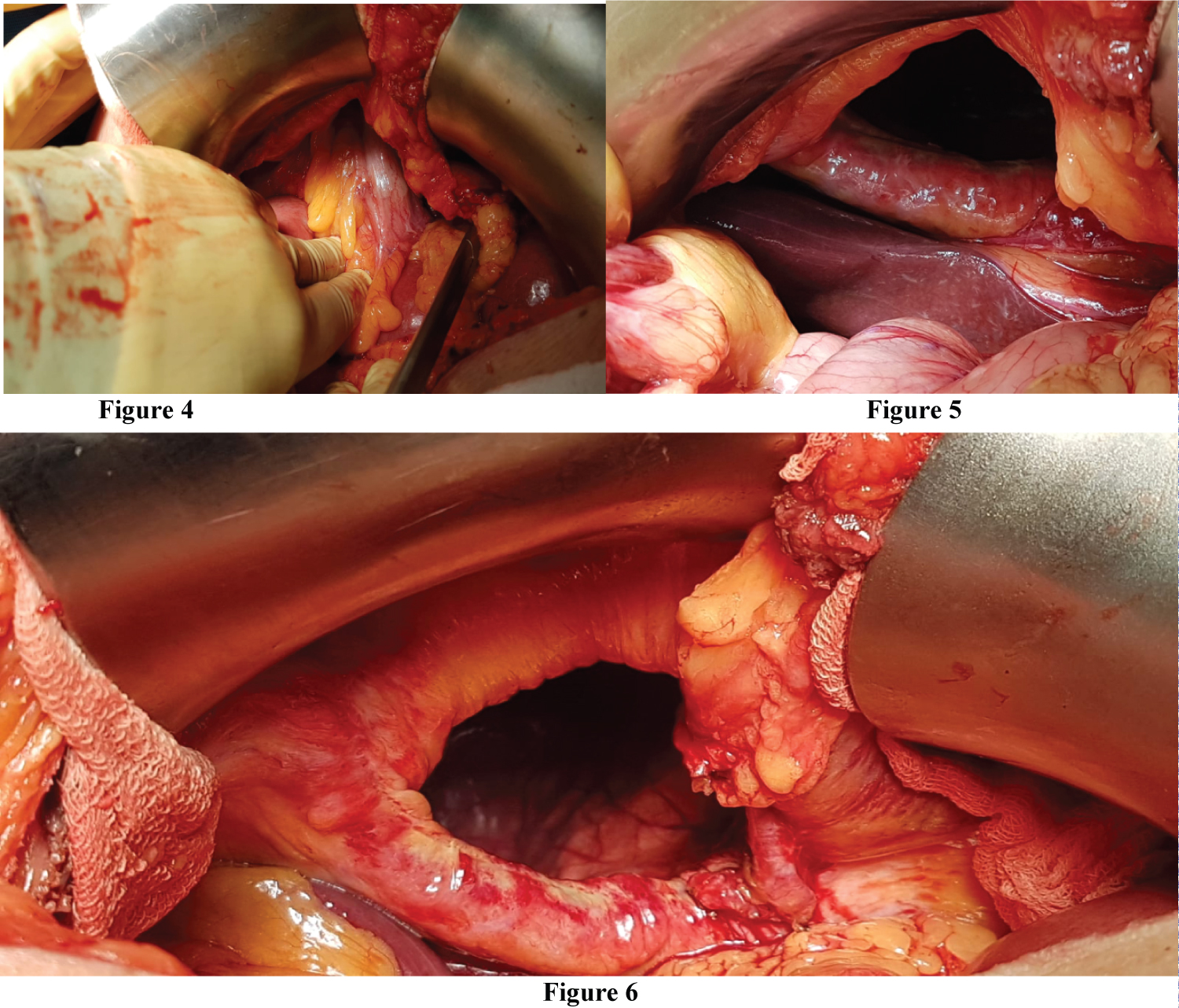
Median laparotomy was performed, it was evidenced: Morgagni hernia with a hernial sac of approximately 4 × 7 cm, contained in its interior thickened small intestine, transverse colon and omentum. No signs of ischemia were found (Figure 4, Figure 5 and Figure 6).
Hernial sac was reduced. Parietal peritoneum dissection to make a pocket where a 15 × 15 cm polypropylene mesh was placed, fixed by means of a 5 mm titanium fixation device. Review of hemostasis and closure by planes.
Postoperative
The first postoperative hours required vasoactive drug support, due to an increased need for them, an urgent evaluation was requested by Cardiology, and an urgent echocardiogram was performed in the postoperative room, finding cardiac tamponade, which was resolved with urgent pericardiocentesis and pericardial drainage.
The patient improved hemodynamically, an urgent CT scan was performed to determine the cause of cardiac tamponade. Chest CT: Postsurgical pericardial effusion. Possible injury to the right ventricle, close to the ventricle there was a mesh fixation device, with no evidence of contact with the pericardium.
Evolution
The pericardial drain was removed 48 hours later, without complications. The patient was admitted to the surgical area, discharged on the 7th postoperative day, due to good clinical evolution and resolution of intestinal obstruction symptoms.
Discussion
The diaphragm is a dome-shaped musculotendinous structure that represents the lower part of the pleural cavity and the roof of the abdominal cavity. The muscular part originates from the entire circumference of the opening lower thoracic and is divided into three parts. The pars lumbalis originates on both sides of the lumbar spine and participates in the formation of the esophageal and aortic hiatus.
At right sternocostal trigone forms the cleft of Morgagni, and in the left sternocostal trigone, the cleft of Larrey. The tendinous part (Speculum Helmotii) is the central area and presents the vein passage hole lower cellar. Because of extensive pericardial attachment on the left which does not allow herniation, the hernia is more common on the right side and is situated anteriorly. Almost 90% of Morgagni's hernias are reported to be on the right side, with 2% located on the left and 8% bilateral. The sac lies between the pericardium and the right pleura.
It is frequent that is diagnosed in adult age of an incidental way, since they are in the habit of being asymtomatic. It produces symptoms in situations of increase of abdominal pressure or when they strike new entrails in herniary sac. Herniary contents, according to frequency, are epiplum, colon, stomach, liver and small bowel [2,3].
Diagnosis is usually done by conventional radiography with occasionally missed cases. Computed tomography scan can be useful in diagnosing the contents of the hernia sac and is noninvasive and accurate. Pleuropericardial cyst, lipoma, intrathoracic tumours, and eventration of diaphragm should be differentiated from Morgagni's hernia while making a diagnosis [4-6].
To avoid the risk of strangulation, some recommend repair even in asymptomatic patients whereas some advocate conservative approach because Morgagni's hernia remains asymptomatic for a long time [7]. A subxiphoid preperitoneal approach has the benefit of a small incision. In cases of certain diagnosis, abdominal approach (open or laparoscopic) [8] is preferred over thoracic approach for surgery because of easier reduction of the hernia and because abdominal viscera within the hernia can be easily pulled down to their normal location [6,9].
About injuries caused by fixation devices. Mesh fixation in Morgagni hernia repair using titanium mechanical fixation devices is not without risk. Cases of intestinal fistula secondary to intestinal perforation have been described, which suggests that they are not the safest fixation methods in this type of hernias. It is necessary to consider the proximity of the anterior diagram to the right ventricle, which is of vital importance when applying this type of device [10-12].
Conclusion
Most of the patients are asymptomatic and present late usually with complications. Diagnosis in suspected case can be confirmed by computed tomography scan. Surgery by abdominal approach is management of choice. It is important to describe the possible complications of the use of mesh fixation devices, as well as the anatomical proximity of the right ventricle with this type of hernias.
References
- Torralba JA, Liron R, Morales G, et al. (2002) Hernia de morgagni gigante. Tratamiento laparoscopico mediante protesis bilaminar (composite) de polyester. Cirugía Española 72: 303-305.
- Gangopadhyay N, Upadhyaya VD, Gupta DK, et al. (2007) Obstructed morgagni's hernia. Indian Journal of Pediatrics 74: 1109-1110.
- Kelly MD (2007) Laparoscopic repair of strangulated morgagni hernia. World Journal of Emergency Surgery 2.
- Taskin M, Zengin K, Unal E, et al. (2002) Laparoscopic repair of congenital diaphragmatic hernias. Surg Endosc 16: 869.
- T Loong, HM Kocher (2005) Clinical presentation and operative repair of hernia of morgagni. Postgrad Med J 81: 41-44.
- Rakas FS, Dayma KG, Gabukamble DB (1988) Obstructed morgagm's hernia (A case report). Indian Journal of Surgery 50: 144-146.
- Comer TP, Clagett OT (1966) Surgical treatment of hernia of the foramen of morgagni. The Journal of Thoracic and Cardiovascular Surgery 52: 461-468.
- Arora S, Haji A, P Ng (2008) Adult morgagni hernia: The need for clinical awareness, early diagnosis and prompt surgical intervention. Ann R Coll Surg Engl 90: 694-695.
- Hussong RL Jr, Landreneau RJ, Cole FH Jr (1997) Diagnosis and repair of a morgagni hernia with video-assisted thoracic surgery. Ann Thorac Surg 63: 1474-1475.
- Bellon JM, Buján J, Contreras L, et al. (1996) Comparision of a new type of plytetrafluoroethyelene patch (micromesh) and polypropilene protesis (Marlex) for repair of abdominal wall defects. J Am Coll Surg 183: 11-18.
- Morales Conde S, Morales Mendez S (2003) Hernioplasthy with the double crown technique. In: 57 Leblanc KA, Laparoscopic hernia surgery. An operative guide. Arnold, London, 133-142.
- Nguyen SQ, Divino CM, Buch KE, et al. (2008) Postoperative pain after laparoscopic ventral hernia repair. A prospective comparison of sutures versus tacks. JSLS 12: 113-116.
Corresponding Author
Juan Emmanuel Sánchez Lara, MD, Department of General and Gastrointestinal Surgery, Salamanca University Hospital, Paseo de San Vicente, 182, 37007 Salamanca, Spain, Tel: +34-923291100
Copyright
© 2021 Lara JES, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.