Challenges following Prenatal Diagnosis of Bilateral Renal Agenesis and Spontaneous Therapy of Fetal Renal Replacement, or Transplant by Auto-Amnioinfusion in a Monoamniotic Twin Discordant Twin with Associated Postnatal Diagnosis of Anorectal Malformation
Abstract
Bilateral renal agenesis (BRA) is often diagnosed on prenatal diagnosis by ultrasound because it leads to an oligohydramnios. When both kidneys are absent this condition is not compatible with life. 40% of babies with bilateral renal agenesis will be stillborn, and if born alive, the baby will live only a few hours. The other sequelae include pulmonary hypoplasia associated multiple gestations, congenital malformations, features of Potter's syndrome, etc. Few reported cases in twins have all been fatal in the neonatal period with no reported cases of survival beyond 2 months. We wish to report an extremely rare and interesting case of an infant with bilateral renal agenesis diagnosed prenatally in one of the monoamniotic discordant twins who had no oligohydramnios, normal pulmonary function, no Potter's syndrome and who had an association of anorectal malformation as part of the VACTREL association diagnosed postnatally. The baby survived fetal period due to renal replacement or transplant by auto amnioinfusion and plasmapheresis in the neonatal period followed by peritoneal dialysis thereafter in infancy and is doing well in the toddler period while awaiting a renal transplant. We wish to report a very rare and interesting case of a 1.5-year-old toddler boy who presented with this combination of congenital anomalies posing various challenges.
Keywords
Anorectal malformation, Auto-amnioinfusion, Bilateral renal agenesis, Fetal therapy, Peritoneal dialysis, Plasmapheresis, Prenatal diagnosis, Renal transplant, Twinning, VACTERL
Abbreviations
BRA: Bilateral Renal Agenesis; GPAL: Gravida, Parity, Abortion, Living Child; APGAR: Appearance, Pulse, Grimace, Activity and Respiration; CTPL: Cross Table Prone Lateral; ARM: Anorectal Malformation; VACTERL: Vertebral, Anal, Cardiac, Tracheal, Esophageal, Renal, Limb; PSARP: Posterior Sagittal Anorectoplasty
Introduction
Our team has an extensive experience of prenatal diagnosis, fetal surgery interventions and twin gestations but have never come across such an exciting case with several issues and implications with regards to the diagnosis and subsequent therapeutic interventions requiring in depth advanced communication and consultation skills in a multidisciplinary institutional set up [1-4]. Bilateral renal agenesis leads to oligohydramnios and in contrast, gastrointestinal obstruction proximal to the ligament of Treitz reduces effective removal of amniotic fluid, leading to polyhydramnios. While case reports describe normal amniotic fluid volume and pulmonary function in monoamniotic twins discordant for bilateral renal agenesis, [5,6] few reports describe singleton pregnancy with renal agenesis and duodenal atresia presenting without pulmonary hypoplasia [7]. We wish to share our exciting experience in the management of such a complex case and review several technical, ethical, social, cultural and political challenges involved.
Case Report
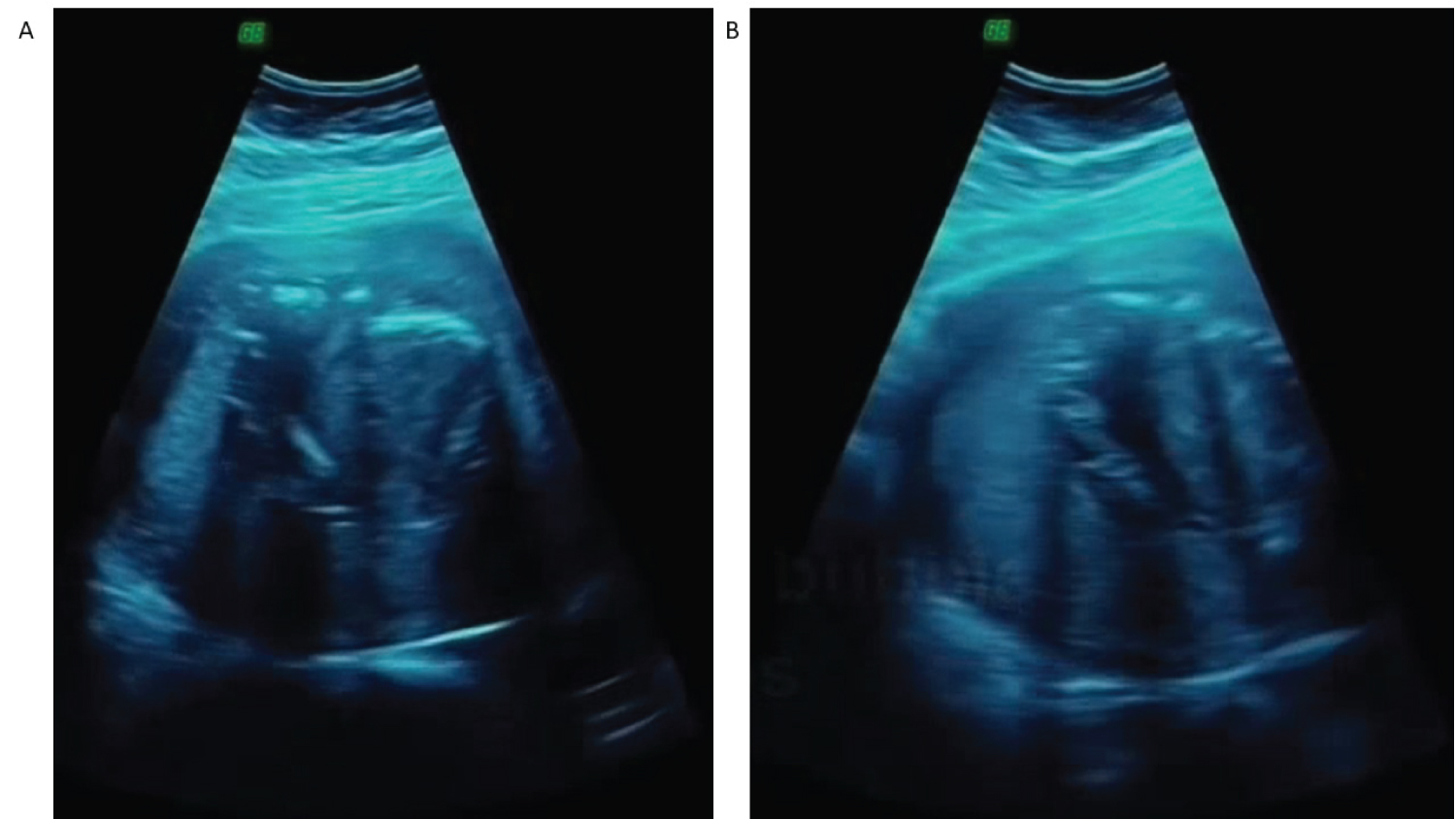
A 24-year-old G1P1A0L0pregnant woman presented for prenatal ultrasound scan at which she was diagnosed with a twin pregnancy. One of the twin boys had been noted to have bilateral renal agenesis with absent bilateral renal tissue in the abdomen (Figure 1A) and non-visualisation of the bladder bubble in the pelvis (Figure 1B) but the amniotic fluid and the pulmonary development appeared normal. The mother was monitored during pregnancy which was uneventful and underwent an uncomplicated delivery at 36 weeks of gestation of normal-appearing twin boys.
One of the boys who had the bilateral renal agenesis was showing apparently healthy appearance with normal APGAR scores and normal phenotype without any evidence of Potter's syndrome, was doing well with no respiratory difficulties and normal physical examination findings except supernumerary little toe digits bilaterally, an imperforate anus and has not passed urine. Nasogastric tube was passed easily without any hold up in the esophagus and vital signs were within normal limits.
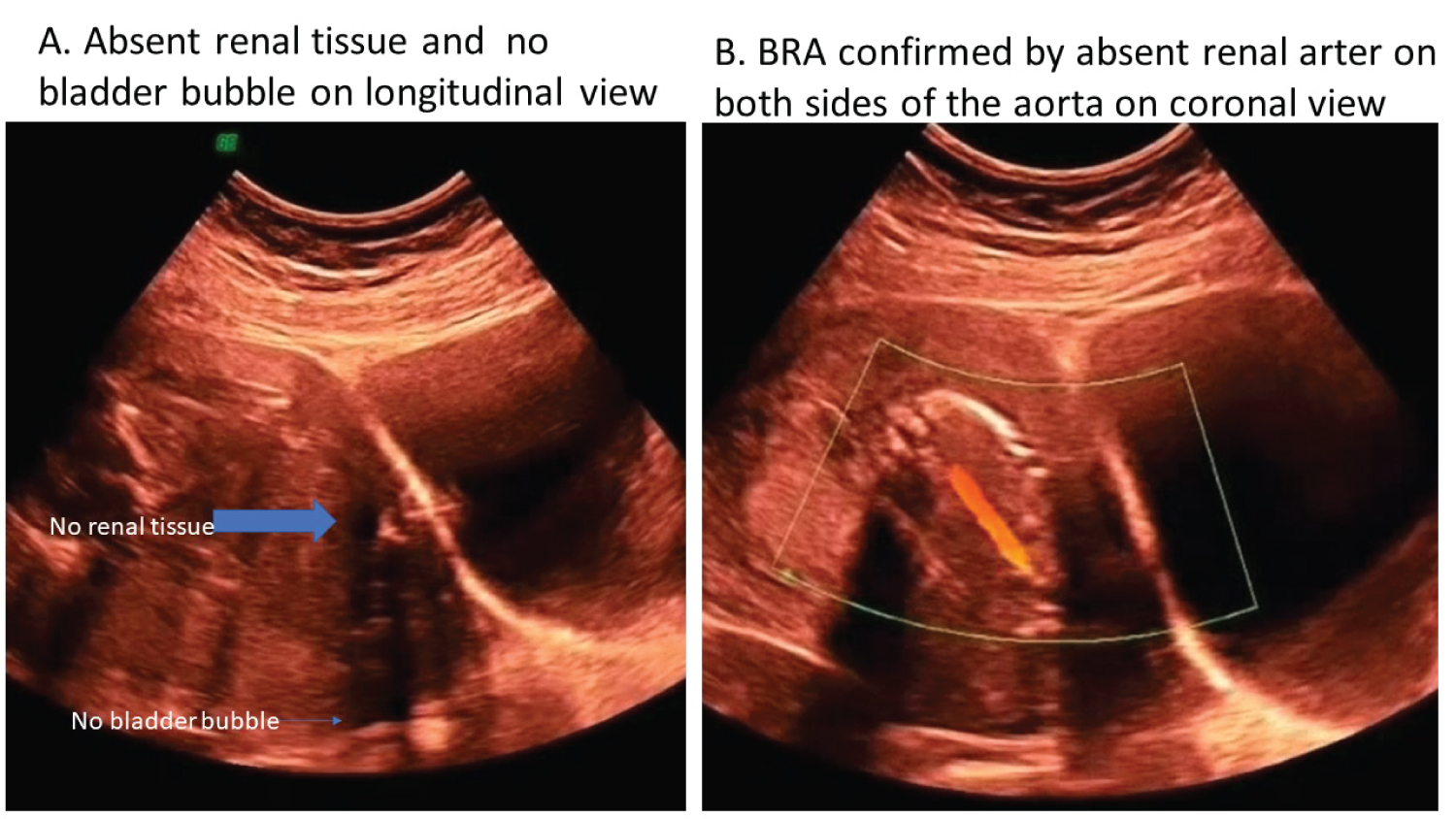
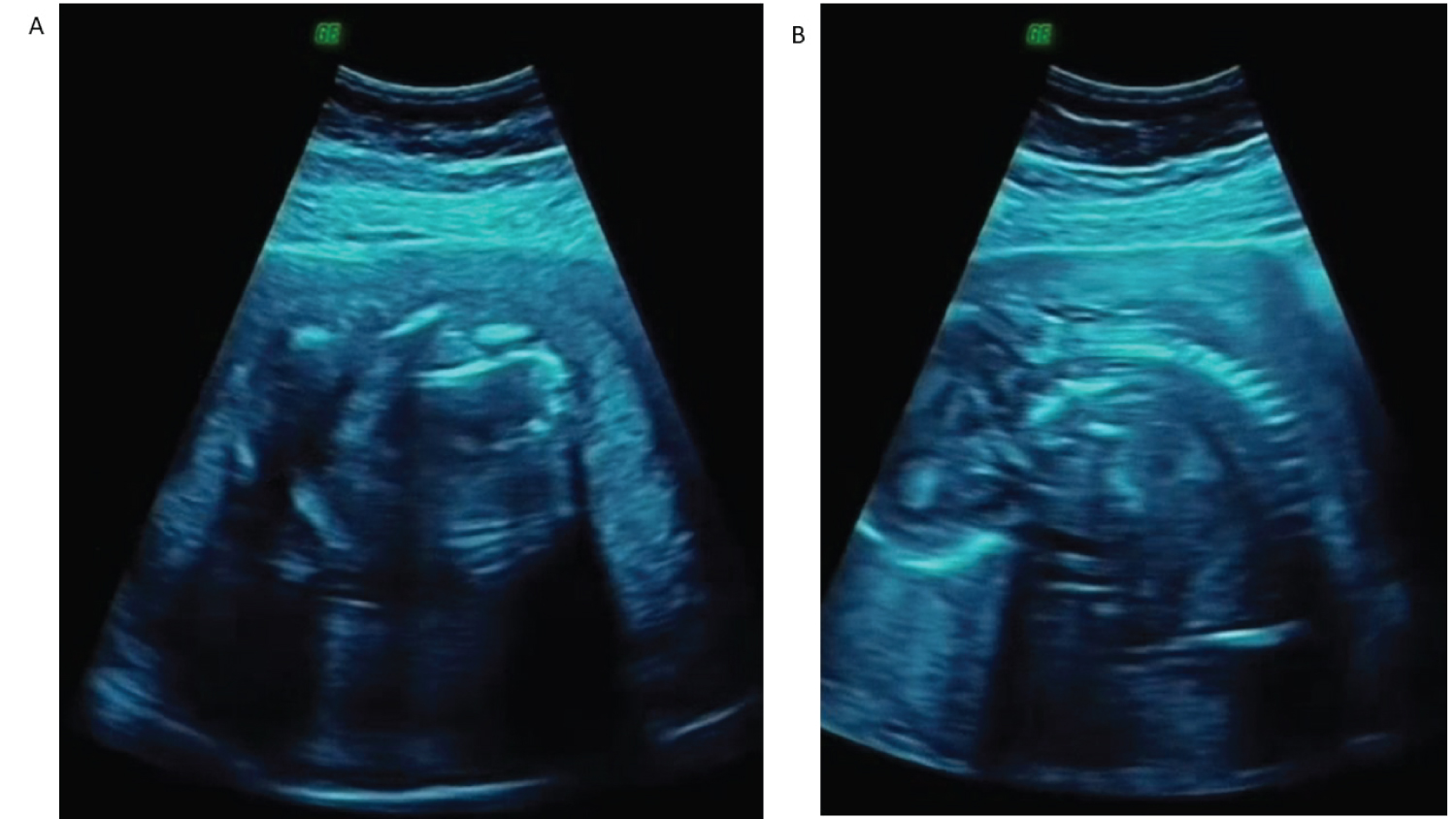
The laboratory values at birth were normal but the subsequent results were consistent with renal failure. Abdominal and renal/bladder ultrasonography and color Doppler scans of the abdomen and pelvis confirmed no evidence of kidneys (Figure 2A and figure 2B). Ultrasound of the heart (Figure 3A) and spine (Figure 3B) were normal as part of the VACTREL association study. Echocardiogram was normal.
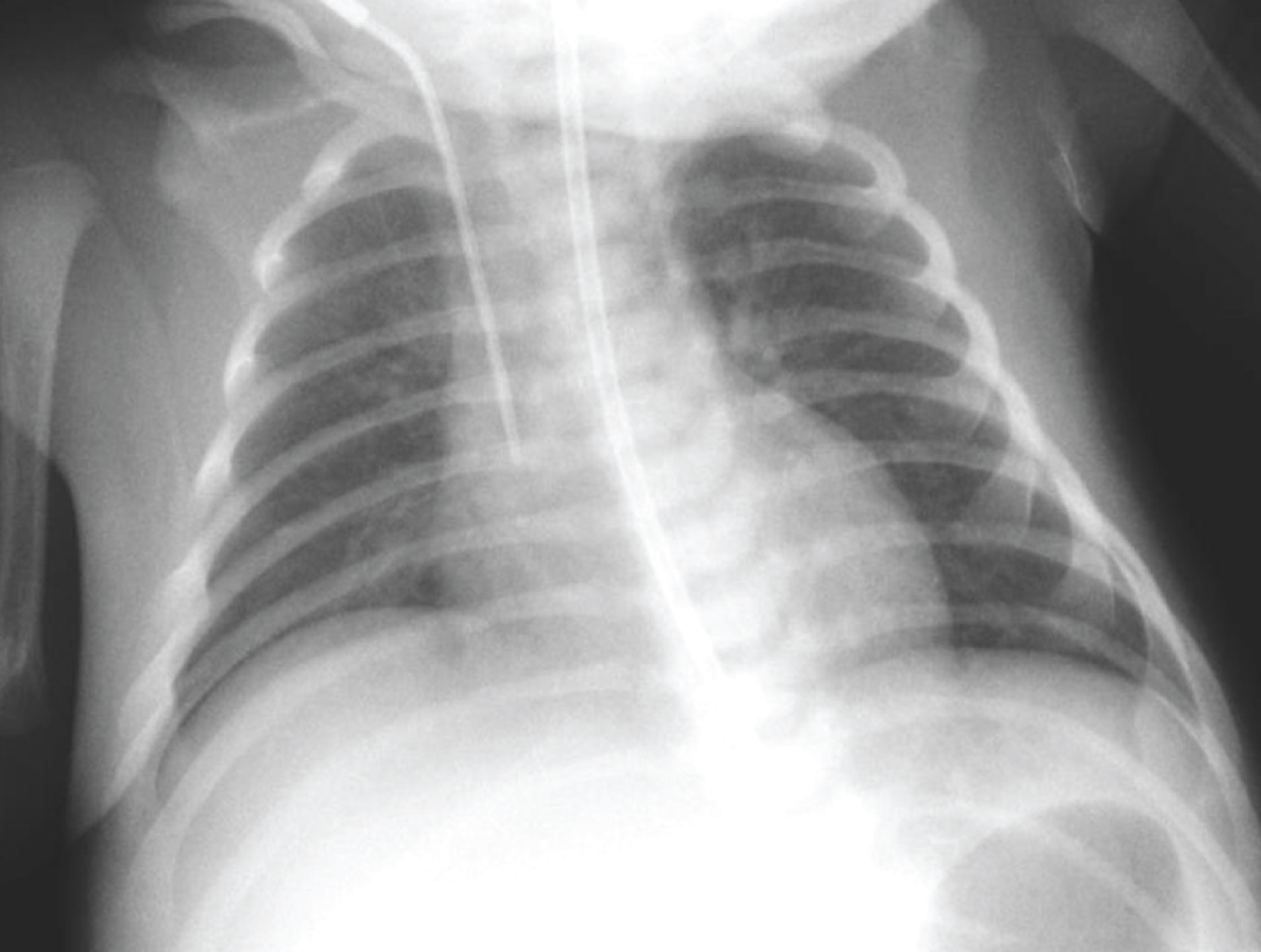
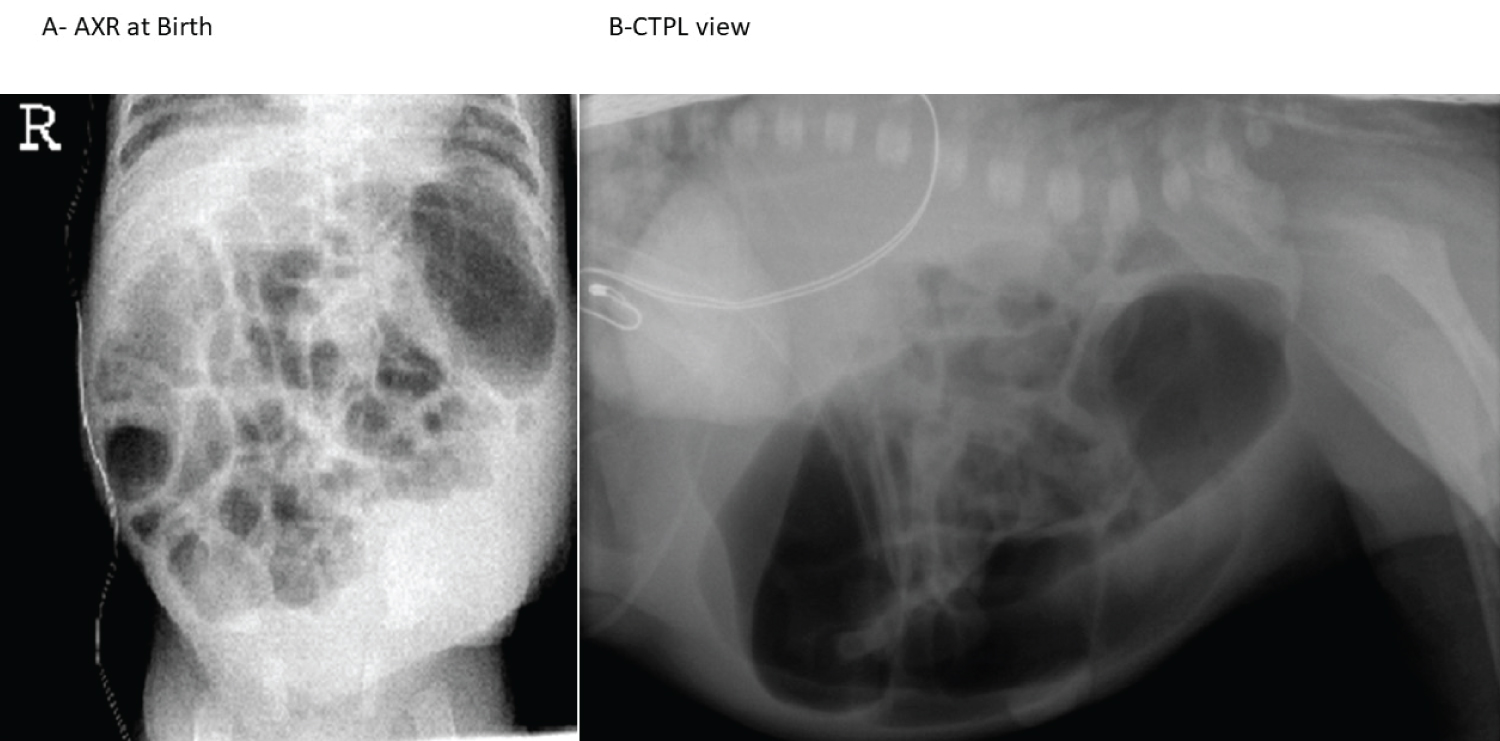
Chest radiograph showed normal pulmonary fields and cardiac image and no vertebral anomalies were noted (Figure 4). A 24-hour delayed abdominal radiograph (Figure 5A) showed normal gas pattern with some dilated bowel on the left side of the abdomen but no vertebral anomalies and the cross table prone lateral (CTPL) view of the pelvis centred over the greater trochanter (Figure 5B) revealed high type of the anorectal malformation (ARM) and the VACTREL (vertebral, anal, cardiac, tracheal, renal, esophageal, limbs) association was diagnosed with renal and anal involvement.
We have explained the final diagnosis of bilateral renal agenesis with high anorectal malformation and how the donation of the amniotic fluid by the fellow twin brother has miraculously helped auto amnioinfusion in these monoamniotic discordant twins during fetal life providing intrauterine renal replacement or transplant which allowed normal pulmonary development and avoided associated oligohydramnios causing Potter's syndrome.
Our multidisciplinary team meeting was held where parents were given detailed information allowing them to ask questions and concerns and the given an overview of all available options in the treatments for an informed decision. The first-time new parents were very emotional with the good news of fetal normal development and were excited to have normal twin pregnancy and uneventful delivery and wanted to do whatever possible for this unfortunate twin brother. It was decided to do staged correction of the high anorectal malformation with initial colostomy and plasmapheresis via central line and place peritoneal dialysis catheter followed by posterior sagittal anorectoplasty (PSARP) and finally closure of the colostomy.
Plasmapheresis was started and the patient underwent examination under anesthesia, insertion of the peritoneal dialysis catheter and left descending colostomy uneventfully. Once the colostomy was mature gradual shift of the plasmapheresis to peritoneal dialysis was performed successfully. At 3 months of age the patient underwent posterior sagittal anorectoplasty and the extra peritoneal colostomy closure was carried out after 6 weeks of the PSARP uneventfully.
At 18 month follow up, the patient is asymptomatic, thriving well and doing well on home peritoneal dialysis and is on the renal transplant waiting list.
Discussion
BRA is commonly associated with stillbirth or perinatal death as is usually not compatible with life, due to the consequences of severe oligohydramnios: Chest and body compression of the fetus with resultant cardiac failure, and/or severe pulmonary failure after prolonged inability to expand and mature the alveolar tree. BRA in one of a pair of monoamniotic twins is an exception to this situation, as the co-twin with normal renal function has the ability to compensate fluid volume for the affected fetus, changing the natural history of the condition. Only two previous reports of such events are reported with maximum survival of two months in one of them [6,7].
Our case is exceptional and contrary to the many of the accepted facts such as role of amniotic fluid in the pulmonary development, oligohydramnios related Potter's syndrome and associated deformations, difficulty in diagnosing associated anomalies like ARM and no option of termination of pregnancy in view of lethal outcome in such hopeless cases.
One of the Monoamniotic twins, thought prenatally to be having only bilateral renal agenesis, were discordant for multiple malformations including high anorectal malformation making a VACTERL association at birth. In 1980's Michael Harrison the first fetal surgeon from the California, USA started an era of prenatal diagnosis and intervention and we followed the suit. The technological advances allowed many if not all of the congenital malformations to be diagnosed [1]. In our case imperforate anus could not be diagnosed and is an exception to the rule and in other similar case a VACREL association with anorectal malformation, tracheoesophageal fistula and other limb anomalies were all missed [8]. The VACTERL association is a conglomeration of various malformations but it may be diagnosed with as few as 3 components present and our case had renal, anal and limb components.
Amnioinfusion has been used for fetuses with bilateral renal agenesis and shows the lengthiest recorded survival in an infant with bilateral renal agenesis [7,9,10]. The affected twin had BRA, but normal pulmonary development because the co-twin produced amniotic fluid and donated in utero to the affected twin. Surviving patients of BRA are exceedingly rare and search showed eight cases infants with BRA with one surviving beyond 2 months of age. Many cases of BRA in monoamniotic monochorionic twins demonstrate the following pattern: Normal lung tissue, lack of Potter's sequence, and extra renal comorbidities, and incremental improvement in BRA survival [10]. Congenital renal anomalies are the most common cause of pediatric end stage renal disease, accounting for two fifth of pediatric transplants.
Conclusion
We presented the unusual case of a monoamniotic twin discordant twin diagnosed bilateral renal agenesis prenatally with normal pulmonary function and amniotic fluid but were unable to diagnose the associated high anorectal malformation as part of VACTREL association. This case shows the importance of normal renal function of the fellow twin in the production of amniotic fluid that was able to donate it due to monoamniotic twin and its relationship to the proper development of the pulmonary system and avoiding oligohydramnios. Recent advances in prenatal diagnosis, perinatal care, peritoneal dialysis, highly skilled professionals, superb home care team, the Government of India financial health card welfare schemes, both dedicated parents being highly educated college teachers and educated family made the survival possible and to deal with end stage renal disease with its attendant morbidities.
Compliance with Ethical Standards
Acknowledgments
We are grateful to Dr Jitendra G Govani, Primary Care Physician and Dr. Deepak G Makadia MD, DCH consultant pediatrician for referring the patient to us and monitoring the home peritoneal dialysis and coordinating with our home dialysis team.
Conflict of interest
The authors have no conflict of interest to declare. No funding source was involved in this study.
Ethical approval
All procedures performed on human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from the parents and all the relatives involved prior to all the procedures. Parents and all involved parties were informed about the procedure.
References
- Patel RV, Sharma RK (2000) Ultrasonic Prenatal Diagnosis. Gynecology & Obstetrics Update 2: 37-43.
- Patel RV, Anthony FM, Govani ND, et al. (2022) Abdominal Wall Defects and Hernias-lessons learnt from observations from the experimental fetal surgery gastroschisis model in rabbits and their clinical extrapolation. Medp Pediatr Child Health 1: 8-15.
- Patel RV, Lawther S, McCallion WA (2013) Discordant monozygotic total colonic Hirschsprung's disease presenting with neonatal isolated ileal perforation. BMJ Case Rep 2013: bcr2013200743.
- Patel R, Frost J, Ninan GK (2013) Neonatal urinary ascites complicated by ileal perforation in a recipient of twin-to-twin transfusion syndrome. Int Urol Nephrol 45: 17-20.
- Perez-Brayfield MR, Kirsch AJ, Smith EA (2004) Monoamniotic twin discordant for bilateral renal agenesis with normal pulmonary function. Urology 64: 589.
- Klinger G, Merlo P, Aloni D, et al. (1997) Normal pulmonary function in a monoamniotic twin discordant for bilateral renal agenesis: report and review. Am J Med Genet A 73: 76-79.
- George L, Manimtim W, Sharma J (2017) A Singleton Infant with Bilateral Renal Agenesis and Normal Pulmonary Function. Case Rep Pediatr 2017: 1710371.
- Lebel RR, Jones G, Israel J, et al. (2002) Renal agenesis without lung hypoplasia, VACTERL syndrome. TheFetus.net.
- Michaela O, Pavel D, Martin G, et al. (2022) Unilateral macrocystic dysplasia and contralateral agenesis in a monoamniotic twin. Ceska Gynekol 87: 278-281.
- Atherton JG, Ferguson JM, Hastings MC, et al. (2016) Long-term survival in a patient with bilateral renal agenesis. Open J Clin Med Case Rep 2: 1133.
Corresponding Author
Ramnik V Patel, Director-Professor, Department of Pediatric Surgery, Postgraduate Institute of Child Health and Research and K T Children Government University Teaching Hospital Rajkot 360005 Gujarat, India; Specialist Pediatric Surg/Pediatric Urologist at the NHS, UK, Tel: 00447956896641, Fax: 00441162893395
Copyright
© 2022 Govani DJ, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.