Hair-Thread Tourniquet Syndrome; Emergent Diagnosable Condition
Abstract
Hair-thread tourniquet syndrome (HTTS), or hair tourniquet syndrome is a rare emergency condition that often occurs in infants and children when one or more appendages in the body like fingers, toes or external genitalia are circumferentially strangulated by strands of threads or human hair. If it is not recognized early it may jeopardize the viability of the segment and finally lead to necrosis of fingers, toes or external genitalia. Cultural difference in children's vulnerability to Hair-thread tourniquet syndrome were tried to describe in this article. To the best of our knowledge there were few revealed instances of HTTS around fingers and toes in Iranian patients compared with Europe. It appears to be that some social and cultural issues lead toward less predominance of HTTS among Iranian children.
Keywords
Hair, Emergency, Ischemia, Finger, Infant
Definition and History
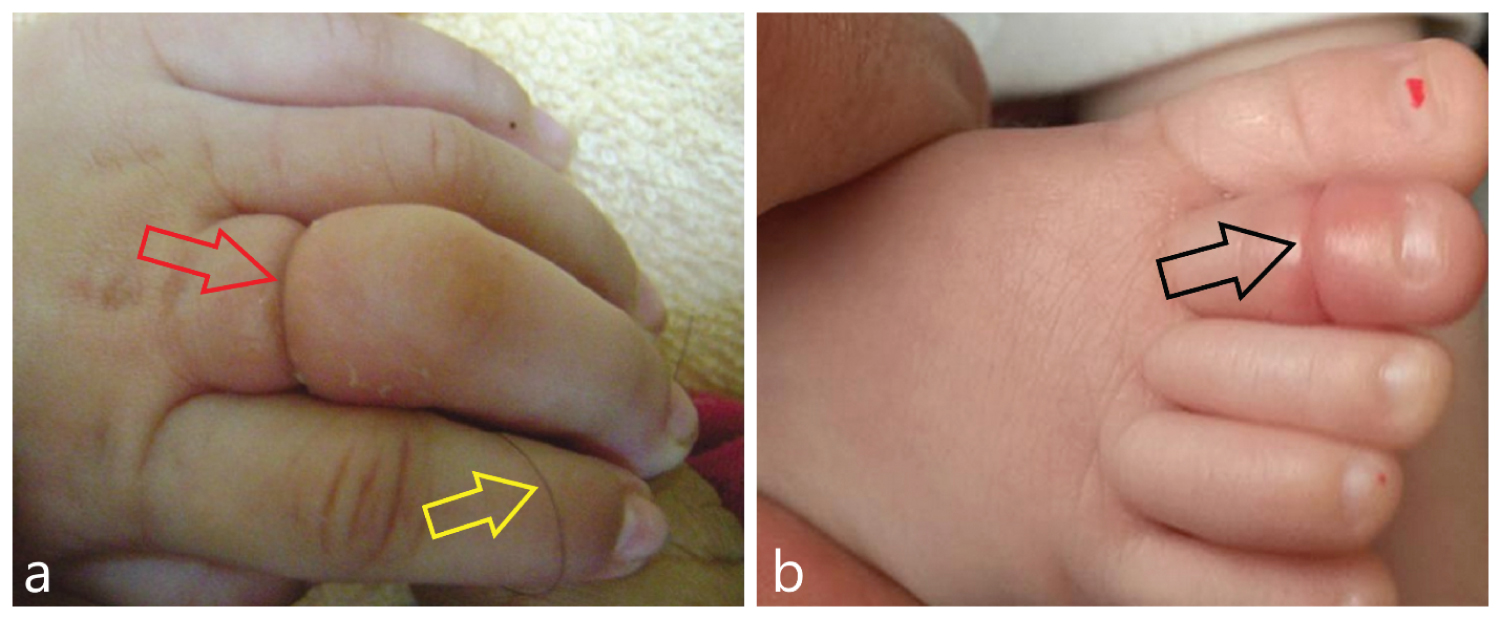
Hair-thread tourniquet syndrome (HTTS), or hair tourniquet syndrome has been perceived in 1612 when a strangulating hair was accounted for around the glands penis but there are variations in other articles that who firstly use "Toe-tourniquet syndrome" in the world but most of the articles said that Quinn used this word for the first time in 1971 [1]. Since that time irregular reports have showed up in the writing portraying Strangulation of limbs by human hair. Regularly the narrowing includes fingers (Figure 1a), toes (Figure 1b), or the penis.
Infants are amazingly free of occlusive vascular illness. Except for embolic illness following enormous vessel catheterization, meningococcemia and a few different types of destructive coagulopathy, ischemia of infant body parts is uncommon [2] and loss of extremities may happen mostly from mechanical tightening coming about because of circumferential imprisonment with strands of material found in the infant's current circumstance [3]. The strangulated parts become progressively swelled, painful and ischemic and if it is not recognized early it may jeopardize the viability of the segment and finally lead to necrosis of fingers, toes or external genitalia. Diagnostic symptoms are kids with excessive crying without any fever, decrease in activity and poor feeding [4].
There are some reports about cultural differences in occurrence of HTTSin pediatrics population. To the best of our knowledge there are no case report of this syndrome in extremities till this time in Iran although it has been reported more frequently in Europe.
The aim of this study is to describe these syndrome andsome effects of cultural differences that dispose children to Hair-thread tourniquet syndrome.
Incidence
The true incidence of Hair-thread tourniquet syndrome is not known but the annual incidence of HTTS is reported 0.02% in some articles [5-6].
HTTS can occur at any age, but most of the affected children are between 12 days up to 6 months of age and near 80% of them are under the age of 2 months [7] which coincide with Telogen effluvium phase of hair development during post-partum period. Hair loss during this period is a well-known phenomenon that is occurs frequently in post-partum women [8-9].
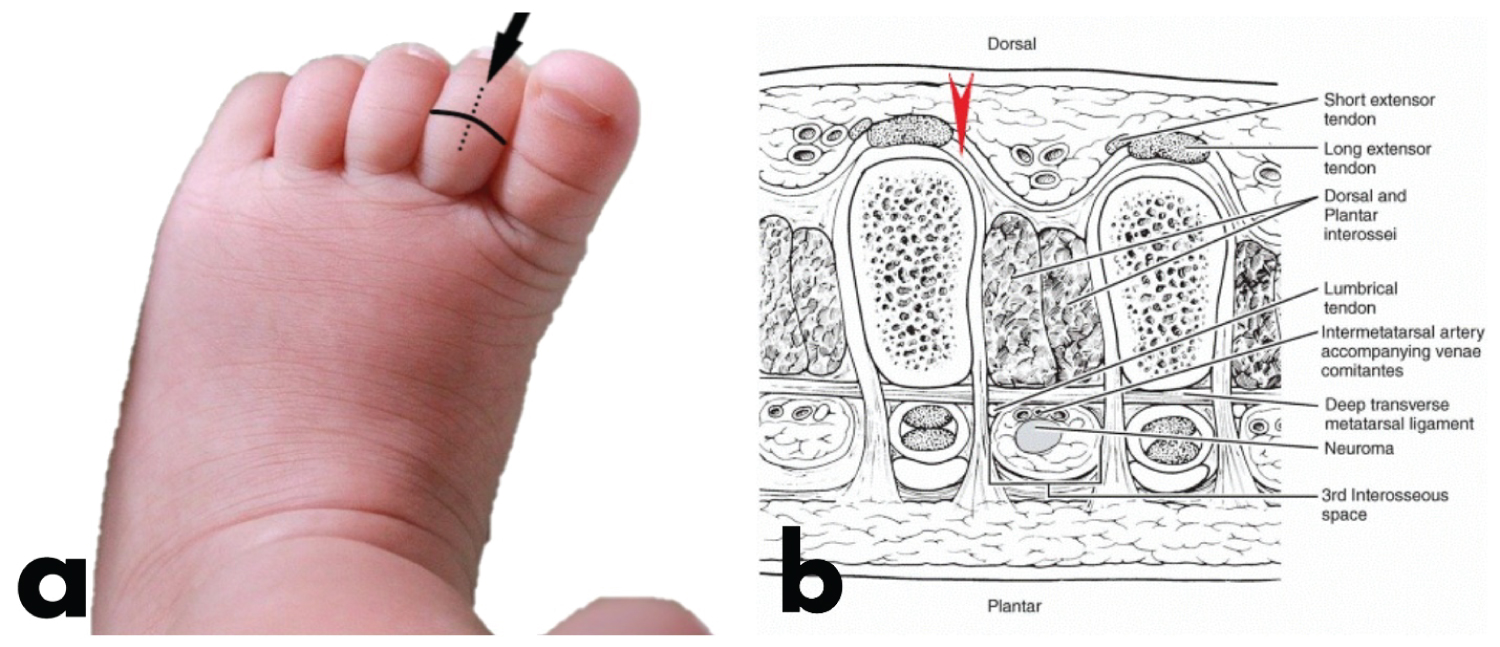
In a literature review and meta-analysis, Mat-Saad et al,. reported that this syndrome affects penis (44.2%), toes, (40.4%), fingers (8.57%), and other sites (female external genitalia, uvula, neck)in 6.83% of cases(10).In 25% of patients two or more toes were involved [11] (Figure 2) and Males and females are involved equally [3].
Etiology
The etiology of this syndrome is thought to be accidental but it should be aware of intentional cases like child abuse [12] but till now the exact etiology in unknown.
Circumferential constriction of appendages by hair or thread, progressively block lymphatic and venous drainage causing distal swelling, redness and pain. Further obstruction can occlude arterial flow that may finally lead to ischemia, tissue necrosis and amputation. When swelling is great, the offending material especially hair was not detected easily.
The toes and external genitalia strangulated mostly by hair, while in the fingers, they are constricted mainly by a piece of thread from woolen or nylon mittens [10-11]. Most of the time only single toe involves in the process, although involvement of multiple toes have been reported. Child maltreatment and abuse should be suspected when multiple toes and digits are involved [10,13]. Some theories were postulated to describe the etiology and occurrence of this syndrome: During the post-partum period, most of the women (up to 90%) experienced a significant hair loss caused by hormonal alteration. This self-limited excessive hair-loss phenomenon that is named Telogen effluvium, occur commonly between 2 and 6 months post-partum [8-9].This phenomenon increase the risk of strangulation of body appendages with maternal hear.
There is a strong relationship between this disorder and sleepwear with encased feet that have been more than once washed [1,14-16]. It is imagined that the unfamiliar material remaining parts in the sleepwear and isn't cleaned out except if the Materials of clothing is washed back to front. It is proposed that human hair property can change when it is wet. Alpert et al postulated that human hair becomes stretched when wet and so more pliable. When the wet hair dries, it starts to constrict and lead to strangulation of an appendage [3,17-20].
There is an association between HTTS and sleepwear with enclosed mitten feet [1,15].When the presence of hair or thread is combined with the increased plantar reflex that is commonly observed in infants, result in creation of enclosed loops that predispose the appendage to be strangulated [15]. If the garment does not turn out during washing the hair or thread may wrapped around the body segment and cause strangulation and ischemia [1,3].
Although it is not a common cause, it should be always consider child abuse as a differential diagnosis of this syndrome. Klusmann and Lenard reported four cases of child abuse as a cause of strangulation. The key findings that we should suspect child abuse as an etiology of HTTS are lack of explanation by the parents, multiple ecchymosed, involvement of multiple toes and digits, and multiple strands of hair with tight knots [21]. Ongoing endeavors to build public familiarity with kid abuse may bring about an expanded number of wrong reports of suspected kid abuse. The creators accept that advanced hair strangulation ought to be incorporated among the conditions that might be mistaken for kid abuse. A review was directed to test this theory.
Experts from the fields of medication, nursing, and youngster government assistance were furnished with a set of experiences and photographic discoveries of a kid with a regular instance of the toe tourniquet condition. Members were reviewed in regards to their understanding of the depicted wounds. Over half of all respondents showed that they would report this case as presumed abuse. Kid government assistance laborers reacted that the wounds were reminiscent of abuse (83%), fundamentally more regularly than general wellbeing medical attendants did (45%) [15].
Cultural aspects
There are many cultural points about HTTS In the literature. The practice of wrapping hair around fingers and toes of children and adults to ward off evil spirits in Gypsies was explained [15,18].
Families and their cultural variables were associated with an increased risk of injury in so many ways (not just HTTS): Household crowding, one or more family moves within the past year, poverty, and inability of mother or father to read well. However, children in single parent households and children whose parents did not drive a car, had less education, or were of rural origin, did not have an increased rate of injury [22]. One way to wean the babies from breastfeeding is wrapping hair around nipple in some Africa culture [18]. Strangulation of penis by tightening a ribbon, band or hair around it to prevent nocturnal enuresis was reported in some cultures [23]. In some cultures parents' ties a piece of hear around penis. They belief this will improve sexual function in adulthood [24].
Although penile strangulation in Iranian patients was reported in literatures [25-26] but there is no reported cases of HTTS around fingers and toes in Iranian patients in the literature. It seems that some cultural, environmental or behavioral points lead to less prevalence of HTTS among Iranian kids. For example most of the children in Iran put on socks or mitten-type gloves during the most of daily activities and consequently they are less vulnerable to strangulation of fingers and toes by hair or threads also Iranian parents were washed their infant clothes separately so it protect them from accidental hairs on the ground or in their clothes.
Diagnosis
The diagnosis of HTTS is mainly clinical. Patients usually present with pain and irritability. On clinical examination there is swelling and redness of the affected parts. in rare situation the child may present with more severe strangulation and tendon or bone erosion [12,27] Systemic sign is absent. Child abuse should be considered in cases with atypical clinical presentation.
Differential diagnosis
Differential diagnosis includes ainhum (dactylosis spontaneity), pseudoainhum, pachyonychia congenital, pityriasis rubra pillar's, mal de Meleda, congenital constriction band, infections, insect bite and allergic reaction [2,12,16,27- 28].
Treatment
Treatments usually simple and effective. It is essential to remove the encircling material completely with the aid of magnifying lo ups to restore the blood circulation of strangulated part. Cut the strand of hair or thread all that is needed but sometimes it is difficult to find and cut the hair or thread especially when severe edema accompanies the strangulation. In this situation cutting the skin maybe needed and as a surgical procedure a careful cutting edge is utilized to make a short, longitudinal, profound cut over the zone of strangulation on the dorsal part of the toe (Figure 3a). The profundity of the cut should reach the phalanx bone, accordingly permitting the total crosscut of the contracting strands (Figure 3b). When the tightening has been delivered, the finish of the cut across hairs/filaments rise and might be effortlessly eliminated by forceps and at the end prophylactic antibiotics directed at Staphylococcus aurous should be administered [3]. The swelling and color change in the digit will resolve rapidly and the child's finger will develop normally [29]. The child should be re-evaluated in the clinic within 24 hours to reassess perfusion, to reassess the wound, and for parental reassurance [17]. Although surgery techniques are gold standards for treating this situation but if minimal edema is present, less invasive techniques can help, for example depilatory agent with a thioglycolate base like hair removal creams can admit to the suspected site for minutes and observe the location for signs of increasing blood flow [4].
Prevention and recommendation
Most of the time, HTTS is preventable and several preventive techniques have been explained in the literature like bellow [3,17,30-31].
1. Educational programs for parents, physicians, nurses and other health care providers to enhance their knowledge about prevention and diagnosis of this syndrome.
2. Washing mother's and infant's clothes separately.
3. Infant's clothes including socks first should be turned inside out and then wash them.
4. Management of postpartum hair loss by keeping the mother's hair tied back, brushed frequently and collecting and disposing of any shed hair.
5. Regularly examine and remove loose strands of hair from clothing and the baby's diaper.
6. Examine the infant's appendages regularly for any sign of swelling and redness.
7. Child abuse should be considered in every child with atypical presentation.
Conclusion
HTTS has to be considered as a cause of toe swelling and discoloration in children. An accurate search of the hair must be performed using magnifying loupes because the hair tourniquet may not be detectable to the naked eye. Early recognition and urgent treatment are mandatory to avoid potential complications. Child abuse should be rule out and preventive issues should teach to infant's parents.
References
- Quinn NJ (1971) Jr. Toe tourniquet syndrome. Pediatrics 48:145-146 .
- Harris EJ (1997) Pediatric lower extremity amputations. Clin Podiatr Med Surg 14: 621-665.
- Harris EJ (2002) Acute digital ischemia in infants: The hair-thread tourniquet syndrome--a report of two cases. J Foot Ankle Surg 41: 112-116.
- Alruwaili N, Alshehri HA, Halimeh B et al. (2015) Hair tourniquet syndrome: Successful management with a painless technique. Int J Pediatr Adolesc Med 2: 34-7.
- Claudet I, Pasian N, Debuisson C, et al. (2009) Tourniquet syndrome: Interest of a systematic analysis of families' social conditions to detect neglect situations. Child Abuse Negl 33: 569-572.
- Kesu Belani L, Leong JF, Narin Singh PSG, et al. (2019) Hair thread tourniquet syndrome in an infant: Emergency exploration saves limbs. Cureus.11: 6377.
- Sudhan ST, Gupta S, Plutarco C et al. (2000) Toe-tourniquet syndrome--accidental or intentional? eur j pediatr 159: 866.
- Lynfield YL (1960) Effect of pregnancy on the human hair cycle J Invest Dermatol 35: 323-327.
- Strahlman RS (2003) Toe tourniquet syndrome in association with maternal hair loss. Pediatrics. 111: 685-687.
- Barton DJ, Sloan GM, Nichter LS et al. (1988) Hair-thread tourniquet syndrome. Pediatrics. 82: 925-928 .
- Mackey S, Hettiaratchy S, Dickinson J (2005) Hair-tourniquet syndrome--multiple toes and bilaterality. Eur J Emerg Med 12: 191-192.
- Mat Saad AZ, Purcell EM, McCann JJ et al. (2006) Hair-thread tourniquet syndrome in an infant with bony erosion: a case report, literature review, and meta-analysis. Ann Plast Surg. 57: 447-452.
- Miller PR, Levi JH (1977) Hair strangulation. J Bone Joint Surg Am. 59: 132.
- Conners G (1997) Index of suspicion. Case 2. Hair tourniquet syndrome. Pediatr Rev 18:283, 285.
- Biehler JL, Sieck C, Bonner B, et al. (1994) A survey of health care and child protective services provider knowledge regarding the toe tourniquet syndrome. Child Abuse Negl 18 : 987-993.
- Chapman HL (1968) Digital strangulation by hair wrapping. Can Med Assoc J 98: 125.
- Smith AM, Peckett W, Davies M et al. (2003) Acquired constriction ring syndrome. foot Ankle Int. 24: 640-641.
- Pester RD, Ballew KK, Harkless LB et al. (1998) The tourniquet syndrome. A case report. J Am Podiatr Med Assoc 76: 354-355.
- Templet TA, Rholdon RD (2016) Assessment, treatment, and prevention strategies for hair-thread tourniquet syndrome in infants. Nurs Womens Health 20: 421-425.
- Alpert JJ, Filler R, Glaser HH et al. (1965) Strangulation of an appendage by hair wrapping. N Engl J Med. 273: 866-867.
- Hoppa EC, Wiley JF (2006) Bathing suit mesh entrapment: An unusual case of penile injury. Pediatr Emerg Care 22: 813-814.
- Summers JL, Guira AC (1973) Hair strangulation of the external genitalia: Report of two cases. Ohio State Med J 69: 672-673.
- Klusmann A, Lenard HG (2004) Tourniquet syndrome--accident or abuse? Eur J Pediatr 163: 495-498; discussion 499.
- Agran PF, Winn DG, Anderson CL, et al. (1998) Del Valle C. Family, social, and cultural factors in pedestrian injuries among hispanic children. Inj Prev 4: 188-193.
- Thomas AJ Jr Timmons, JW, Perlmutter AD et al. (1997) Progressive penile amputation. Tourniquet injury secondary to hair. Urology 9: 42-44.
- Sallami S, Ben Rhouma S, Cherif K, et al. (2013) Hair-thread tourniquet syndrome in an adult penis: Case report and review of literature. Urol J 10: 915-918.
- Hamid A, Seyyed Mahmood Fatemi B, Ali K, Behzad L et al. (2019) Penile Strangulation by Hair: A Case Report. Case Reports in Clinical Practice 4.
- Sheikh Andalibi MS, Azarfar A, Esmaeeli M, et al. (2017) Penile hair tourniquet syndrome due to a coil of hair: first report in iran. the journal of nephro-urology monthly 9: 9788.
- Bizzotto N, Sandri A, Regis D, et al. (2014) Serious delayed hair toe tourniquet syndrome with bone erosion and flexor tendon lesion. Case Rep Pediatr 2014: 592323.
- Gottlieb M, Holladay D, Spearman D et al. (2019) Current approach to the evaluation and management of hair-thread tourniquets. Pediatr Emerg Care 35: 377-379.
- Sivathasan N, Vijayarajan L (2012) Hair-thread tourniquet syndrome: A case report and literature review. Case Rep Med 2012: 171368.
Corresponding Author
Amir Hussein Tavallaei, Department of Physical Medicine and Rehabilitation, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Copyright
© 2022 Tavallaei AH. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.