Mechanical Removal of Calcifications on a Silicone Intraocular Lens with a Shielded Light Pipe in Asteroid Hyalosis
Abstract
Purpose: Calcific deposits on the posterior surface of a silicone intraocular lens (IOL) are a rare visually significant complication of asteroid hyalosis (AH). We report the novel use of a shielded light pipe to remove calcifications on a silicone lens.
Observations: An 82-year-old woman with AH in the right eye and history of bilateral cataract extraction with Yttrium Aluminium Garnet (YAG) laser capsulotomies presented with visually significant calcifications on the silicone IOL of the right eye. Core vitrectomy was performed and a 27-gauge shielded light pipe with 0.045 mm between the tip of the shield and the light source was used to scrape calcifications off the posterior lens surface yielding a 5 mm central clearing. The lens remained in good position. Four months post-operatively, the lens's central axis remained clear and visual acuity improved.
Conclusions and importance: Mechanical scraping with a shielded light pipe and concomitant vitrectomy may be a safer alternative to addressing silicone lens calcifications without undergoing lens exchange.
Keywords
Asteroid hyalosis, Light pipe, Lens calcifications, Vitrectomy
Introduction
Calcification of intraocular lens implants (IOLs) remains a rare complication in patients with Asteroid Hyalosis (AH). This is prevalent on the posterior surface of silicone IOLs, and first line treatment is exchange of the silicone IOL for a hydrophobic acrylic lens. However, there is significant risk with this approach, especially in patients with a history of capsulotomy [1].
Here we present an alternative surgical approach in an AH patient with silicone IOL calcifications and prior capsulotomy undergoing IOL polishing using a 30 mm 27-gauge shielded light pipe with 0.045 mm between the tip of the shield and the light source (Dutch Ophthalmic Research Center (DORC), Exeter, NH).
Case Presentation
An 82-year-old Caucasian woman presented for gradually worsening blurry vision in the right eye over the course of three weeks. Her ocular history was significant for wet macular degeneration, bilateral cataract extraction with placement of 3-piece silicone intraocular lenses within the lens capsule in 2010, and bilateral Yttrium Aluminium Garnet (YAG) laser capsulotomies. Clinical presentation, imaging, and treatment were reviewed and obtained from the electronic medical record in a Health Insurance Portability and Accountability Act (HIPAA) compliant manner.
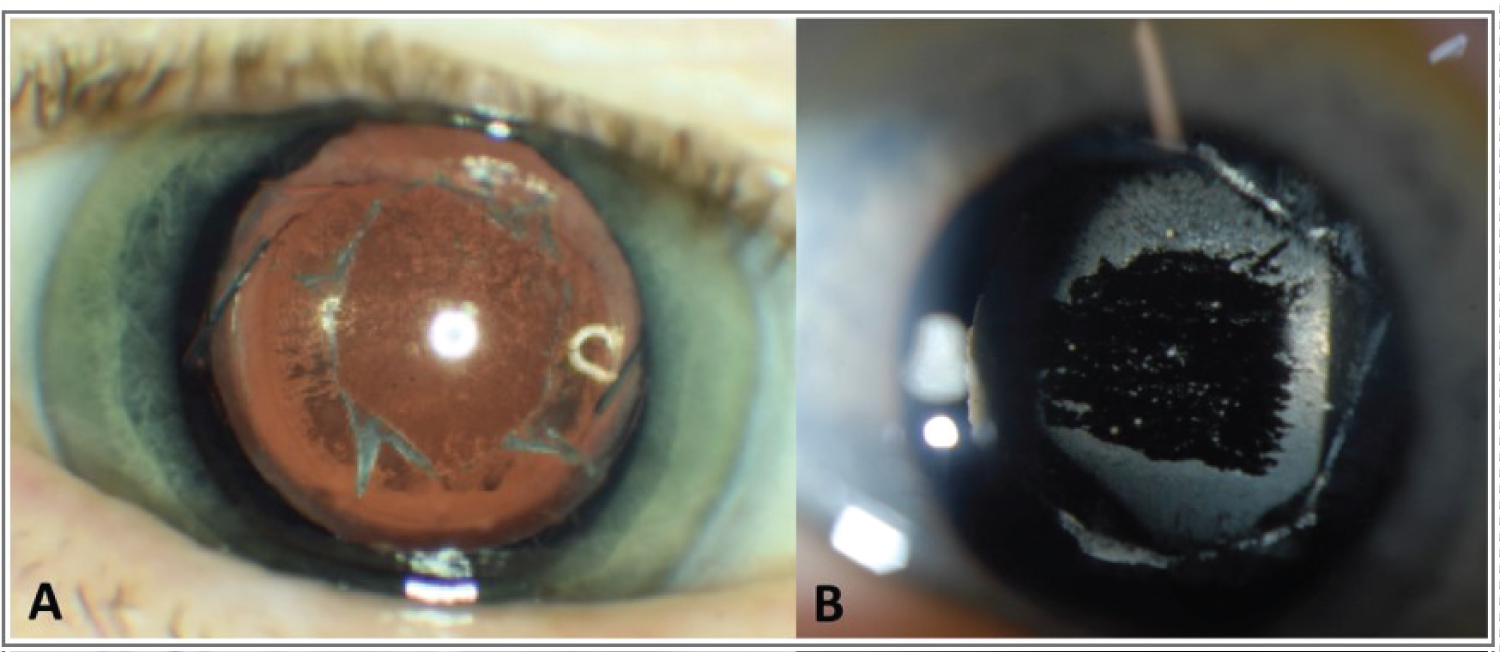
Visual acuity in the right eye was counting fingers (CF). Slit lamp examination and fundus exam of the right eye demonstrated extensive dense deposition of crystals on the posterior lens surface and vitreous opacities consistent with asteroid hyalosis (Figure 1A). Examination of the left eye did not reveal findings of asteroid hyalosis.
The decision was made to undergo 27-gauge pars plana vitrectomy (PPV) with lens debridement to clear the visual axis without IOL removal.
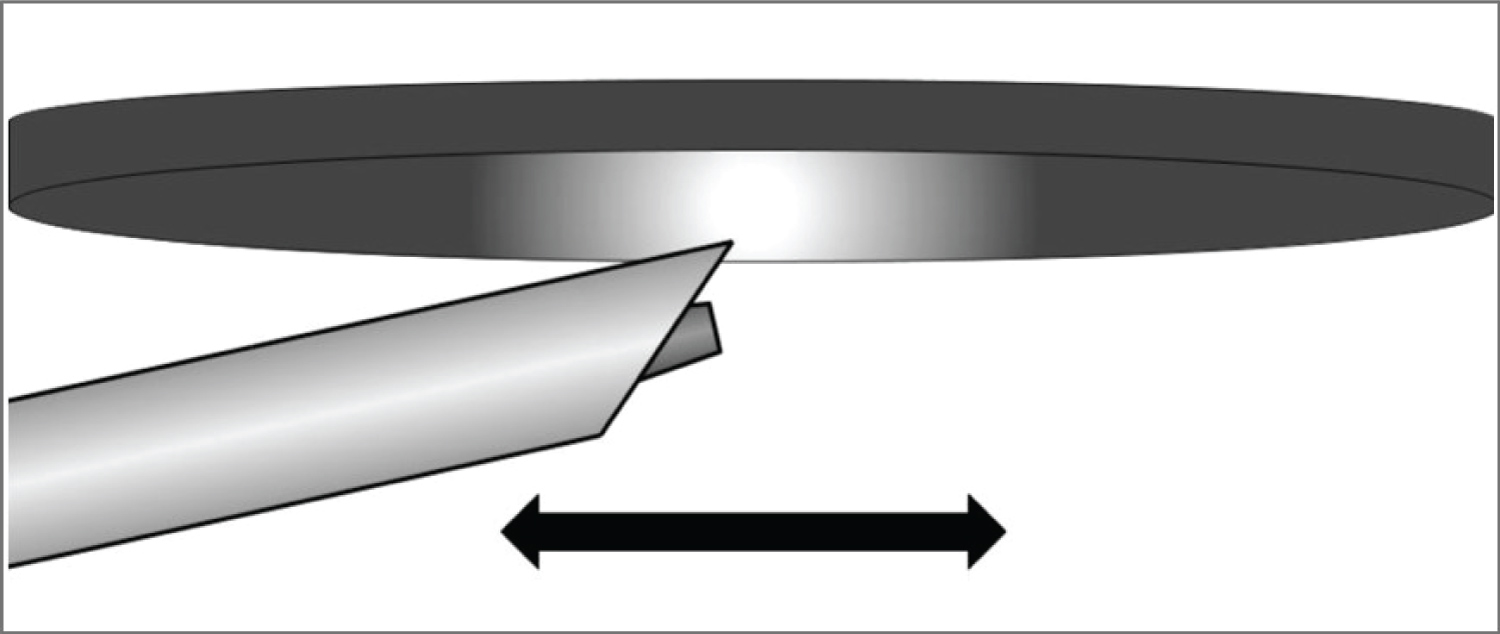
Core vitrectomy was performed, after which, attention was directed towards the IOL. Attempts to remove crystalline deposits on the posterior lens capsule with a vitrector and soft-tip cannula were not successful. A shielded light pipe was then used to gently scrape the posterior surface of the IOL using the hooded tip of the light pipe yielding a central clearing of 5 mm without dislocating or damaging the IOL (Figure 2). Intraoperative anti-VEGF injection was performed.
Vitreous fluid was sent for biopsy, revealing pink radial spherical bodies that were consistent with asteroid hyalosis.
Postoperatively, visual acuity improved to 20/200 from CF at baseline, likely limited due to wet macular degeneration. Slit lamp examination demonstrated a clear central axis through the posterior lens surface without recurrence of crystal deposition. At postoperative month four, visual acuity remained stable without evidence of recurrent crystal deposition (Figure 1B). Fundus exam showed trace residual asteroid bodies.
Discussion
We present a case of successful debridement of calcifications on the posterior surface of a silicone IOL with a shielded light pipe and PPV in a patient with asteroid hyalosis. The standard treatment for opacified lenses is IOL explantation and exchange. However, this is associated with a high rate of complications such as corneal decompensation, loss of capsular support, and changes in refractive error. In addition, up to 33% of patients required anterior vitrectomy for vitreous prolapse and 48% required anterior vitrectomy if the patients had a history of capsulotomy [2]. To avoid IOL exchange, a few case reports described alternative techniques to clean the posterior silicone lens surface. Mehta, et al. successfully used a 23-gauge vitrector to scrape and aspirate central calcific deposits without intraoperative complications [1]. However, Ullman, et al. and Rainsbury, et al. were both unsuccessful in removing deposits in a similar fashion with 23/25-gauge vitrectors [1,3]. Platt, et al. utilized a 23-gauge vitrector and a silicone-tipped cannula but had the most success using a lighted pick to scrape off the deposits without intraoperative complications [4]. Both Mehta, et al. and Platt, et al. did not report recurrent opacification at 12 and 6 months, respectively [1,4].
To our knowledge, this is the first case describing silicone IOL polishing with a light pipe. Although Platt, et al. reported using a lighted pick, the light pipe's broader beveled tip and wider area of illumination may make silicone IOL scraping more efficient [4]. Also unique to this case, concomitant vitrectomy was performed to remove asteroid bodies from the vitreous to prevent reaccumulation of deposits on the implant. Similar to the report by Platt, et al., a 27-gauge vitrector and a soft-tipped cannula were ineffective at dislodging the deposits [4]. This combination of mechanical silicone IOL polishing with a shielded light pipe and PPV may prove to be safer and more effective than IOL exchange for treatment of silicone lens calcifications. Longer follow-up is needed to determine the long-term success rate of this method and compare it with other forms of management for calcifications on silicone lens implants. Of note, posterior calcification of silicone IOLs is morphologically different to calcification of hydrophilic acrylate IOLs in which calcification not only affect the surface but also the subsurface. Thus, mechanical scraping would not address the subsurface calcifications seen in hydrophilic acrylic lenses [5].
Conclusions
There are numerous ways to address opacified silicone implants caused by calcifications. In the setting where the posterior capsule is open, gently polishing the silicone lens implant with a hooded light pipe may be a safe way to clear the visual axis and improve the patient's vision without need for lens explantation and associated risks.
Patient Consent
The patient(s)/patient's legal guardian consented to publication of the case in writing/orally.
Acknowledgements and Disclosures
Conflicts of interest: none.
No funding or grant support.
All authors attest that they meet the current ICMJE criteria for Authorship.
No acknowledgments.
References
- Ullman DI, Gupta S (2014) Pars plana vitrectomy for dystrophic calcification of a silicone intraocular lens in association with asteroid hyalosis. J Cataract Refract Surg 40: 1228-1231.
- Mehta N, Goldberg RA, Shah CP (2014) Treatment of dystrophic calcification on a silicone intraocular lens with pars plana vitrectomy. Clin Ophthalmol 8: 1291-1293.
- Rainsbury PG, Lochhead J (2014) Pars plana vitrectomy for posterior surface calcification in a silicone intraocular lens in asteroid hyalosis - a report of mistaken identity? Clin Ophthalmol 8: 2239-2241.
- Platt SM, Iezzi R, Mahr MA, et al. (2017) Surgical removal of dystrophic calcification on a silicone intraocular lens in association with asteroid hyalosis. J Cataract Refract Surg 43: 1608-1610.
- Durr GM, Ahmed IIK (2021) Intraocular lens complications: Decentration, uveitis-glaucoma-hyphema syndrome, opacification, and refractive surprises. Ophthalmology 128: e186-e194.
Corresponding Author
Yevgeniy Shildkrot, Department of Ophthalmology, University of Virginia, 1300 Jefferson Park Ave, Charlottesville, VA 22903, USA, Tel: 434-924-5653
Copyright
© 2022 Ambati NR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.