Minimally Invasive Transconjunctival Threading Method of Shortening the Müller Muscle and the Levator Aponeurosis in Severe Involutional Blepharoptosis
Abstract
We have been performing involutional blepharoptosis repair by tucking the Müller muscle and levator aponeurosis with transconjunctival threading for over 10 years, while striving to improve this technique. The aim of the present paper is to introduce some progress in surgical quality.
The surgical technique described in this manuscript is performed in the following order: (1) The Müller muscle is exposed after the conjunctival fornix incision and a 7-0 nylon thread with double armed needle (MANI3365) is passed through the tarsal side. (2) From this site, a thread is passed 5 mm through the underside of the tarsal plate, and then after coming out again on the tarsal plate side. (3) From this point re-thread again to the site of the conjunctival incision in the conjunctival fornix. (4) At this site, a double armed needle thread from above the Müller muscle to a sufficient depth, including the posterior layer of the levator aponeurosis, so that both arms intersect. This surgical process for enhancing eyelid elevation is the most important in the present improved technique. (5) After ligation and checking the elevation of eyelid is satisfactory, cut the suture and close the conjunctival incision site by coagulation.
This technique may be more useful for treating involutional blepharoptosis than the previously reported procedures if the levator function is good. Additionally, we evaluated the safety, non-invasiveness, efficacy, and persistence of long-term surgical effects of this method and found that it can be recommended as a surgical procedure in severe cases as marginal reflex distance-1 (MRD-1) of 1 mm or less. This method is also one that is recommended for elder adults who use anticoagulants because the amount of blood during surgery is minimal.
Keywords
Involutional blepharoptosis, Internal approach, Müller muscle, Levator aponeurosis
Introduction
The number of patients with involutional blepharoptosis is increasing due to the increase in the aged population, resulting in a rise in the number of cases requiring surgery. There are two concepts of surgical methods for involutional blepharoptosis: External and internal approaches (transconjunctival method) [1]. The surgical approach of the former is from the skin side, while the latter is from the conjunctival side. The superiority and inferiority of these methods have been discussed from various perspectives [2,3]. Currently, the most commonly used transconjunctival ptosis surgery is shortening of Müller's muscle (Müller muscle conjunctival resection), which is also used for severe cases [3] in Western countries; however, the greater degree of intraoperative and postoperative invasiveness is an issue.
Selection of the surgical method is determined by the surgeon according to each patient's situation. The most important point for this selection is safety and efficacy. Given the importance of minimally invasive surgery for the increasingly elderly patient cohort, we pursued the feasibility of ptosis surgery with transconjunctival threading and found that this procedure was useful [4]. Subsequently, this procedure has been improved to expand the scope of surgery indications, and we have reported the better results [5]. However, some severe cases (MRD-1 of 1 mm or less) have experienced insufficient persistence of eyelid elevation after surgery and recurrence, which is a point for improvement.
Here, we present a modified threading method of the Müller muscle and levator aponeurosis, which is a non-invasive procedure. Furthermore, we describe the surgical results of this method obtained thus far for perspectives.
Subjects
This review article included adults with blepharoptosis. Written informed consent was obtained from all the subjects. This study was conducted as per the tenets of the Declaration of Helsinki. Patients whose image appears in this publication provided additional written consent for publication. Preoperative and postoperative MRD-1 was measured using anterior segment OCT (CASIA2, Tomey Corporation, Nagoya, Japan) [6] to ensure accuracy, and Bonferroni's method was used for the statistical significance test.
From 60 patients with involutional ptosis, 91 eyes underwent surgery in the past three years using the method reported here. Of these, severe patients (MRD-1 < 1 mm) who were followed for more than one year (follow-up was conducted every three months after surgery) consisted 3 males and 16 females (25 eyes in total), with a mean age of 68.9 years were focused. Preoperative levator function was better in all patients with 8 mm or higher and an average of 10.68 mm. The results of phenylephrine testing were positive for 11 patients and negative for 8 patients.
Surgical Procedures
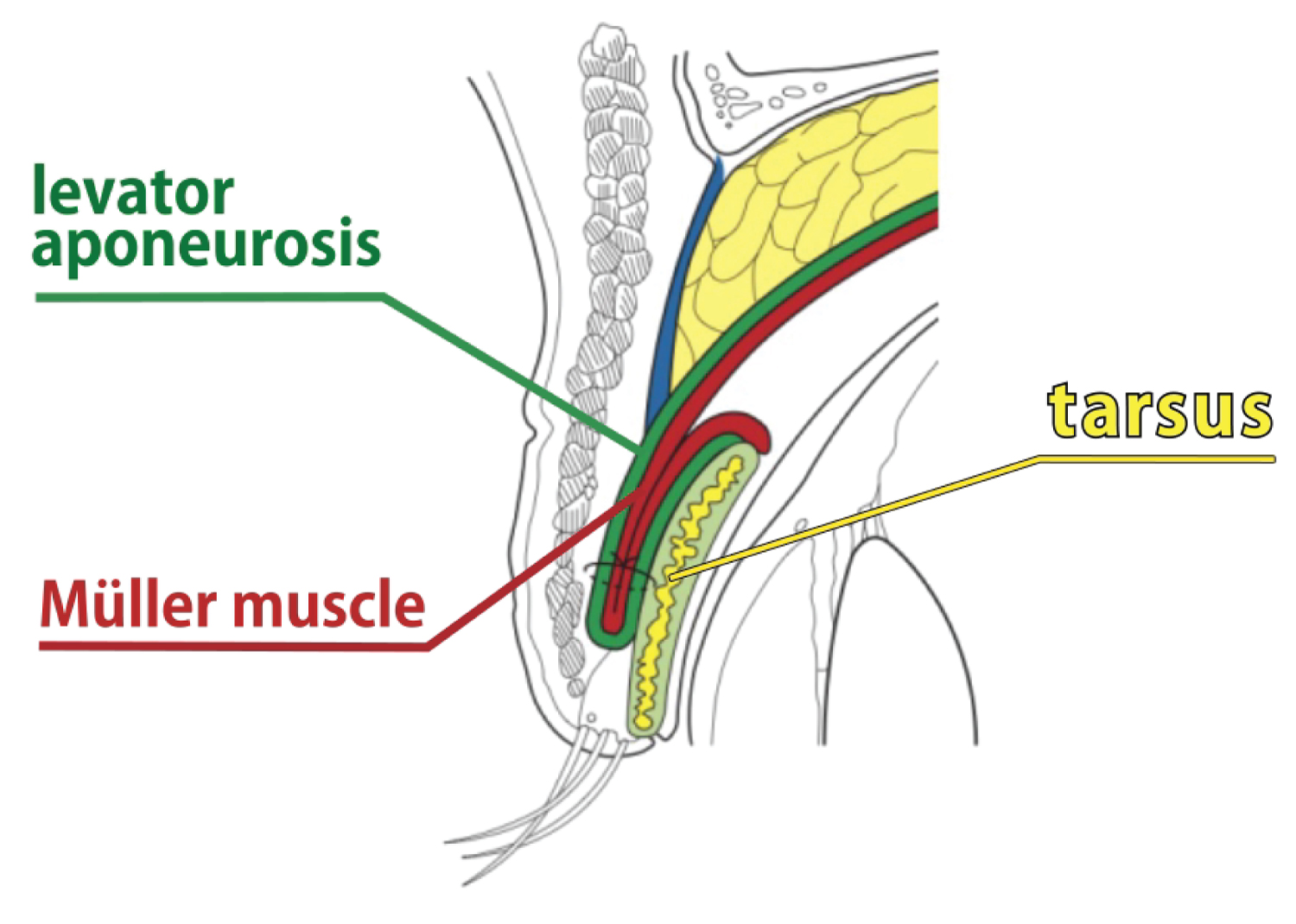
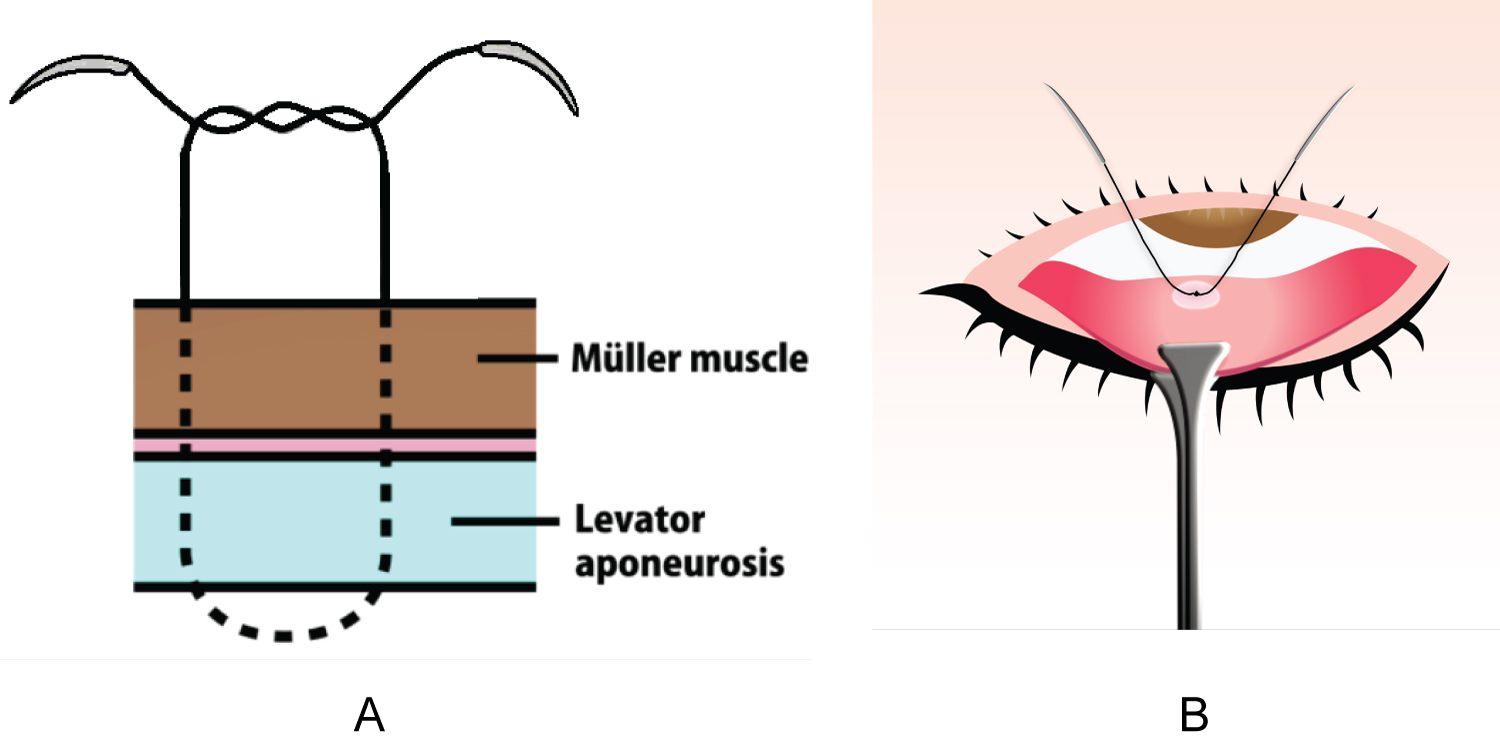
1) After anesthetizing with anesthetic eye drops, invert the upper eyelid and perform local anesthesia below the tarsal plate using 1% lidocaine without sympathomimetics. 2) Grasp the tarsal plate at 5 mm away from the eyelid using the tips of the fixation forceps (INAMI® S361) and invert the tarsal plate. 3) Apply a small amount of local anesthesia at approximately 5 mm away from where the forceps are holding the tarsal plate and make an incision approximately 5 mm wide into the conjunctiva using a high frequency scalpel, taking care not to damage the Müller muscle. 4) Thread 7-0 nylon double armed thread (MANI®3365) approximately 3 mm from the eyelid margin into the tarsal plate under the Müller muscle. 5) Thread approximately a further 5 mm through to the underside of the tarsal plate, and then, after coming out again on the tarsal plate side, re-thread again to the site of the conjunctival incision of the conjunctival fornix. 6) At this site, thread a double armed suture from above the Müller muscle to a sufficient depth, including posterior layer of the levator aponeurosis, so that both arms intersect. 7) After checking that the elevation of the eyelid is satisfactory, coagulate the conjunctival incision site and close. The above procedures are presented in the supplementary video and an image of the sagittal section of the upper eyelid after surgery is shown (Figure 1).
When compared with the previous paper [5], improvements in this surgical method include the following aspects: First, the Müller muscle was exposed after incising the conjunctiva. From this area, a thread was passed through the tarsal side and re-thread again to incised conjunctival fornix. Then, the thread was passed through the posterior layer of the levator aponeurosis and ligated for enhancing eyelid elevation (Figure 2). This process is the most important in the present improved technique, which is based on the proved anatomical findings [7]. Additionally, the tucking width of the Müller muscle and levator aponeurosis could be changed (by approx. 6 mm) by adjusting the threading site according to the distance from the tarsus, controlling the degree of eyelid elevation.
Results
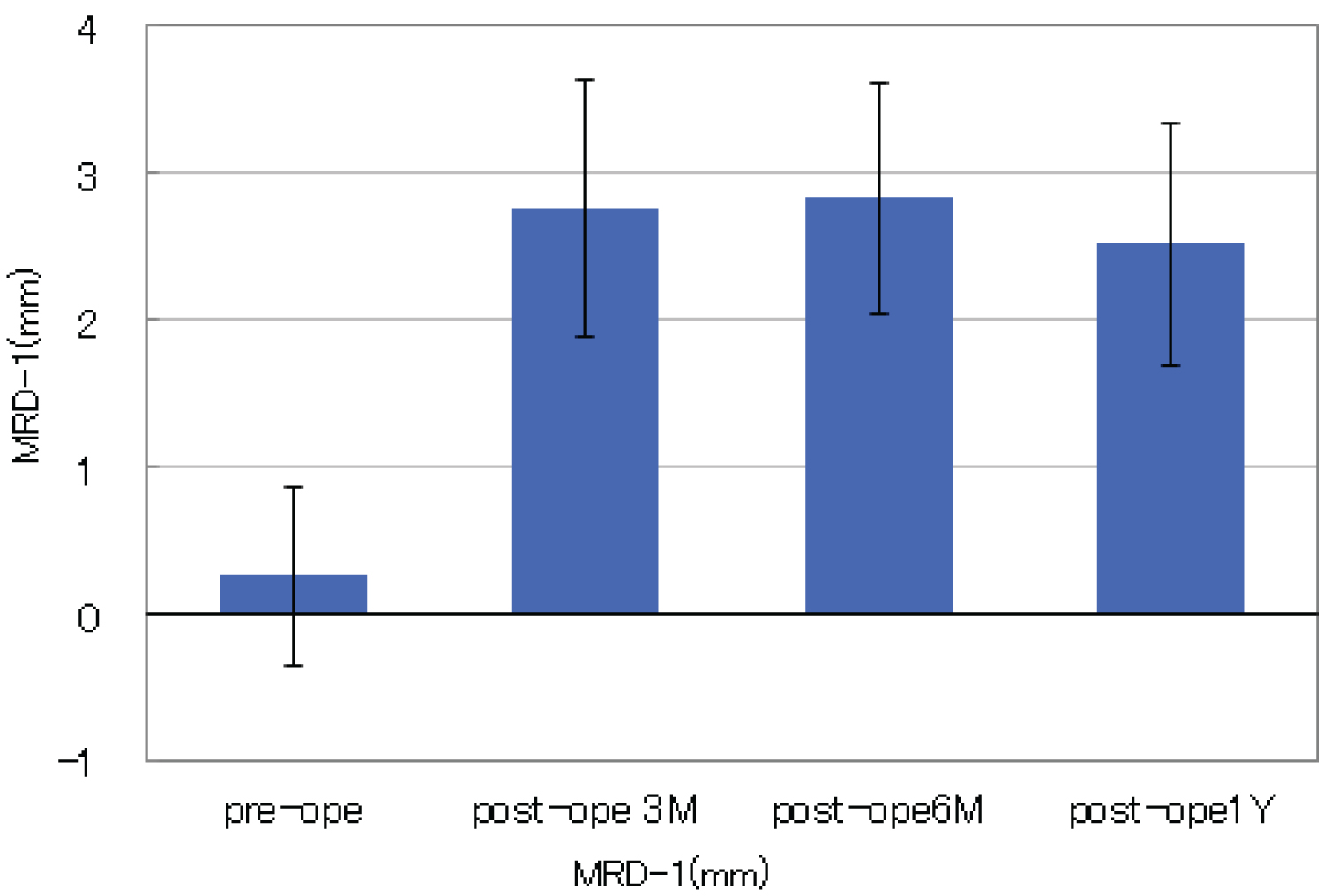
In severe involutional blepharoptosis, changes in MRD-1 improvement at 3 months, 6 months, and one year after surgery in 25 eyes are shown in Figure 3. The figure shows that there is no significant decrease in postoperative MRD-1 of each examined period for one year after surgery, which means sufficient persistence of eyelid elevation. These patients underwent ptosis correction only, and no blepharoplasty was performed for eyelids skin laxity. Furthermore, intraoperative bleeding among five patients who used anticoagulants was minimal. Postoperatively, several patients had slight corneal erosion, eyelid swelling, and subcutaneous eyelid bleeding, however, those are disappeared within a week with ophthalmic solutions. There were no cases of postoperative overcorrection or severe complications.
Conclusion
We have confirmed that as long as the levator function is good, the present technique is useful for the patients with severe involutional blepharoptosis (MRD-1 < 1 mm). This procedure, through threading and fixing not only the Müller muscle, but also the posterior layer of the levator aponeurosis, appears to increase and stabilize the elevation strength of the eyelids. Moreover, surgery time is short with almost no bleeding. The post-operative burden on patients in terms of eyelid swelling and pain etc. is also reduced, meaning that this procedure can be performed safely even on elderly patients and those taking anticoagulants.
There also appears to be advantage for double eyelids and in terms of there being minimal impact on the shape of the eyelid, less postoperative overcorrection, the ability to re-operate, and that it is easy to perform if simultaneously performing surgery to treat blepharochalasis.
Cases for which this surgery would not be suitable include patients with congenital ptosis, patients with acquired ptosis following a neurological disorder or ophthalmic surgery and patients with poor levator function. Ptosis seen in patients who have side effects of glaucoma medication over a long period such as DEUS (deepening of upper eyelid sulcus) and/or PAP(prostaglandin-associated periorbitopathy) maybe treated by another procedures.
Disclosure
The author reports no conflict of interest.
Acknowledgement
The author would like to thank Mr. Hisato Nakatsubo for editing the surgical video and Mr. William Faris for his English narration of the video.
References
- Allen RC, Saylor MA, Nerad JA (2011) The current state of ptosis repair: A comparison of internal and external approaches. Curr Opin Ophthalmol 22: 394-399.
- Saonanon P, Sithanon S (2018) External Levator Advancement versus Muller Muscle-Conjunctival Resection for Aponeurotic Blepharoptosis: A Randomized Clinical Trial. Plast Reconstr Surg 141: 213e-219e.
- Sweeney AR, Dermarkarian CR, Williams KJ, et al. (2020) Outcomes after Müller Muscle Conjunctival Resection Versus External Levator Advancement in Severe Involutional Blepharoptosis. Am J Ophthalmol 217: 182-188.
- Odashima S, Ogasawara K (2006) New suture technique to correct ptosis without incision of the eyelid or the conjunctiva. Jap J Ophthalmic Surg 19: 579-582.
- Ogasawara K (2019) Ptosis surgery with an improved method of shortening the Müller muscle and the levator aponeurosis with transconjunctival threading. J Ophthalmic Surg 2: 7-12.
- Ogasawara K (2020) Application of Second-Generation Swept-Source Anterior Segment-OCT in the Measurement of Marginal Reflex Distance-1 (MRD-1). Clin Ophthalmol 14: 635-642.
- Kakizaki H, Zako M, Nakano T, et al. (2005) The levator aponeurosis consists of two layers that include smooth muscle. Ophthalmic Plast Reconstr Surg 21: 379-382.
Corresponding Author
Kosuke Ogasawara, MD, PhD, Medical Corporation, Ogasawara Eye Clinic, 3-10-12, Takamatsu, Morioka Iwate 020-0114, Japan, Tel: +81-19-(662)-3223, Fax: +81-19-(662)-7331.
Copyright
© 2022 Ogasawara K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.