Double Adnexal Twist
A 48-year-old, gravida 3 paras 3, female presented in ER for acute abdominal pain. The ultrasound revealed a left 5 cm - 6 cm complex adnexal mass; Doppler showed evidence of blood supply occlusion.
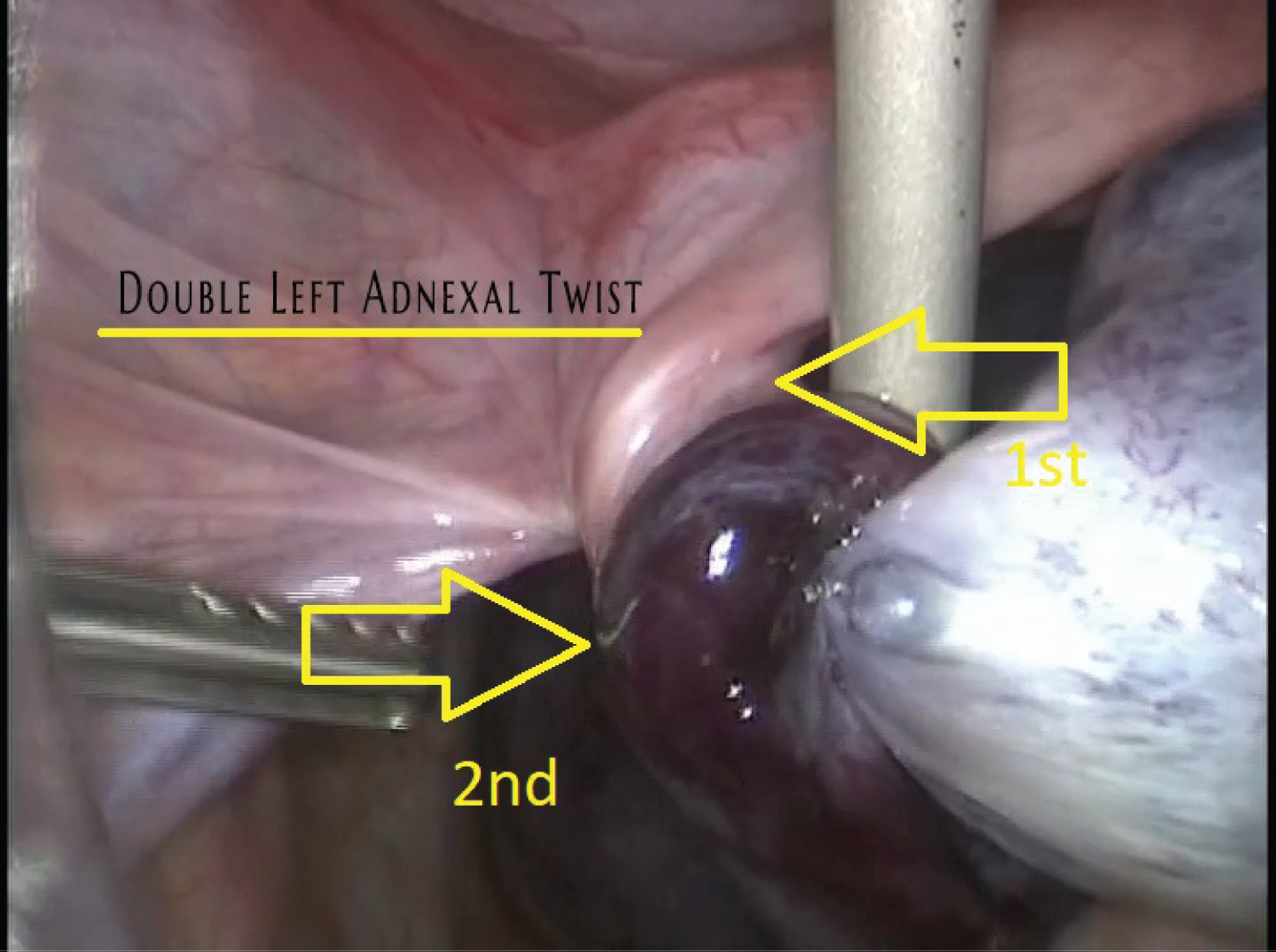
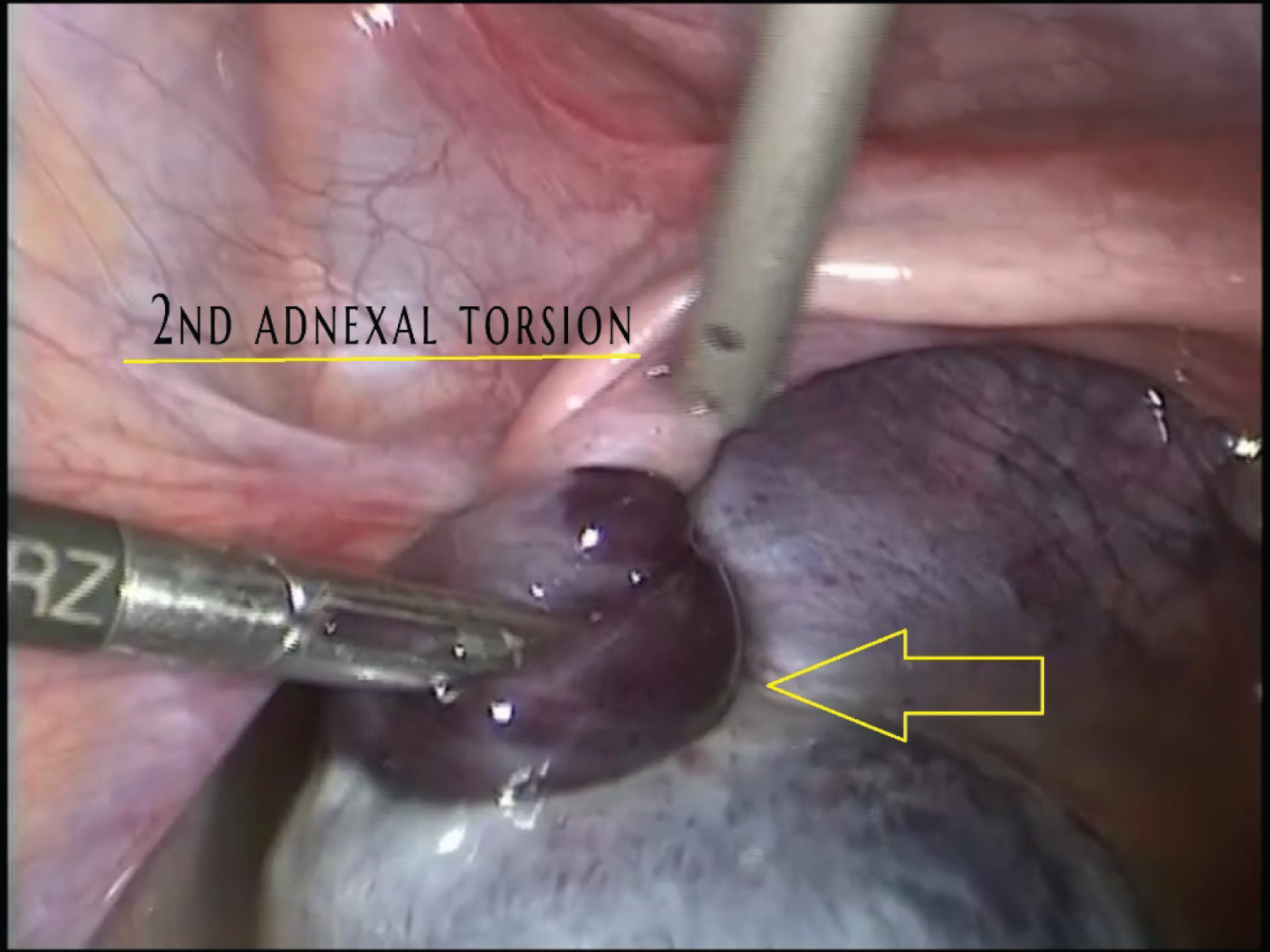
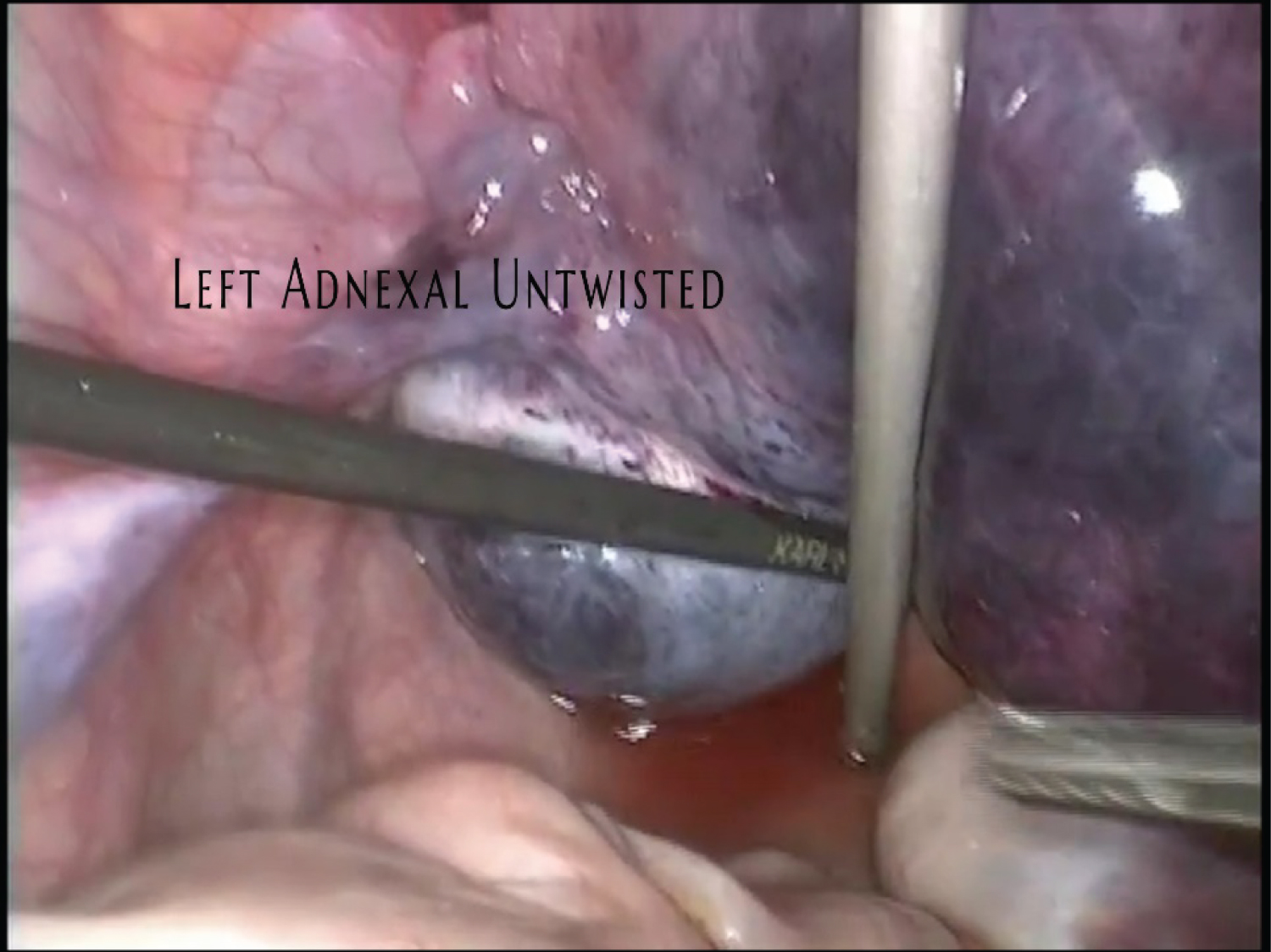
PE with pain on the left lower abdominal quadrant, vaginal bimanual examination with Chandelier's sign positive. Blood work with Lymphocytosis of > 14,000 cells/microL, D-dimer by ELISA testing was 1,500 ng/mL. Laparoscopic surgery was performed (Figure 1), showing double left adnexal torsion (Figure 2). The evidence of necrotic tissue was visualized (Figure 3), and a left salpingo-oophorectomy was performed. The patient's recovery was unremarkable, without any complicated issues.
Ovarian twist refers to the complete or partial rotation of the ovary, often resulting in partial or complete obstruction of its blood supply and may affect females of all ages [1]. It is one of the most common gynecologic surgical emergencies. It is uncommon to find a double twist on the same side.
Chronic adnexal torsion with complete occlusion of the ovarian blood supply will ultimately result in necrosis of the torted tissues and loss of ovarian function [2].
The incidence of adnexal torsion is unknown. In a report of a 10-year review of patients at a women's hospital, ovarian torsion accounted for 2.7 percent of emergency surgeries [3]. Torsion was the fifth most common surgical emergency [4].
Over 85 percent of patients with ovarian torsion have an ovarian mass. Large size, which increases the risk of torsion. Torsion is most likely to occur when the ovary is 5 cm in diameter or larger [5,6].
In 90 percent of the cases, the onset of the pain is suddenly and usually moderate to severe [7]. The character of the pain may be sharp, dull, stabbing, colicky, or crampy, and it may radiate to the flank, back, or groin.
A torted ovary should be considered potentially viable as ovarian necrosis is rare. Salpingo-oophorectomy is indicated in a nonviable ovary that is clearly necrotic [8,9].
The pelvic anatomy is mandatory to do laparoscopic surgical excision of a necrotic pelvic tissue [10].
Disclosure Statement
The authors declare that they have no conflicts of interest and nothing to disclose.
References
- Sanfilippo JS, Rock JA (2015) Surgery for benign disease of the ovary. In: Jones HW, Rock JA, TeLinde's Operative Gynecology. (11th edn), Wolters Kluwer.
- Takeda A, Hayashi S, Teranishi Y, et al. (2017) Chronic adnexal torsion: An under-recognized disease entity. Eur J Obstet Gynecol Reprod Biol 210: 45-53.
- Hibbard LT (1985) Adnexal torsions. Am J Obstet Gynecol 152: 456-461.
- Bouguizane S, Bibi H, Farhat Y, et al. (2003) Adnexal torsion: A report of 135 cases. J Gynecol Obstet Biol Reprod (Paris) 32: 535-540.
- Varras M, Tsikini A, Polyzos D, et al. (2004) Uterine adnexal torsion: Pathologic and gray-scale ultrasonographic findings. Clin Exp Obstet Gynecol 31: 34-38.
- Houry D, Abbott JT (2001) Ovarian torsion: A fifteen-year review. Ann Emerg Med 38: 156-159.
- Cohen A, Solomon N, Almog B, et al. (2017) Adnexal torsion in postmenopausal women: Clinical presentation and risk of ovarian malignancy. J Minim Invasive Gynecol 24: 94-97.
- Oelsner G, Cohen SB, Soriano D, et al. (2003) Minimal surgery for the twisted ischaemic adnexa can preserve ovarian function. Hum Reprod 18: 2599-2602.
- Harkins G (2007) Ovarian torsions treated with untwisting: Second look 36 hours after untwisting. J Minim Invasive Gynecology 14: 270.
- Carlos L, Espinoza V, Valenzuela A, et al. (2020) The Bermuda Triangle� a didactic description of the retroperitoneal anatomy. J Minim Invasive Gynecol 27: S118.
Corresponding Author
Carlos Leal, MD, PhD, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Hospital Christus Muguerza Del Parque, Universidad Autónoma de Chihuahua, Calle de La Llave #1419 suite 103 Colonia Centro, CP 31000, Mexico.
Copyright
© 2022 Leal C, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.