A Comparison of Single Bite and Double Bite Biopsy Techniques in Gastrointestinal Endoscopy: A Scoping Review
Abstract
Endoscopic biopsies may be taken as single or double bite. In the former method intubation time may be proportionately prolonged depending upon the number of biopsies. In contrast to this, in the latter approach, although, a greater number of biopsies may be taken per unit time, equally, it may have effect on the quality of the biopsy specimen. This is because there is a perception that taking biopsies in such a manner may lead to crush artifacts and difficulty with orientation of the specimens. This, as a result, may pose diagnostic challenge to the histopathologist. A literature search was performed, and 11 studies, examining the histological quality of biopsies taken by these techniques, were identified. There were conflicting results. This is because there are considerable differences in the methodology, study power and interpretation of these studies. A holistic study is needed, which is clinically relevant, minimises selection bias and has sufficient power to clarify conflicting issues.
Keywords
Biopsies, Endoscopy, Single bite, Double bite
Introduction
Specimen collection is a routine procedure during endoscopy for the diagnosis and surveillance of various conditions. Furthermore, it is considered as gold standard and, at times, histopathological examination may be the only clue to the diagnosis of certain conditions such as microscopic colitis [1]. Moreover, both endoscopic and histologic diagnostic foci may be patchy; hence, multiple samples are recommended [2]. Similarly, in surveillance of chronic conditions i.e. Barrett's oesophagus, the number of biopsies taken may range from four to 40, depending on the length of the segment [3].
Biopsy samples which include mucosa and sub mucosa [1] and slides providing orientated mucosal tissue in a perpendicular plane demonstrating the entire layer of mucosa, from the mucosal surface to the Muscularis mucosa, may affect the diagnostic yield [3]. This is why histopathological examination requires meticulous handling and proper orientation of specimens i.e. to avoid tangential or horizontal sectioning [4]. An endoscopic biopsy devoid of mucosa is usually considered inadequate for assessment [1]. Attached to this concept, using special pinch forceps, with or without a central spike, biopsies may be taken using either single (SBB) or double bite (DBB) techniques [5].
Considerable controversy exists in the manner of collection of biopsies. This is because of a perception that taking DBB biopsies may cause distortion or misalignment, hence, leading to diagnostic error. Equally, taking DBB may well reduce intubation time, and so complications associated with the procedure itself. Identifying the evidence behind both SBB and DBB may help endoscopist to weigh the pros and cons of histopathological accuracy and endoscopic time and this may change practice in a way that best serves the interest of patients. Therefore, the aim of this review is to consider the way biopsies are taken during gastrointestinal endoscopy.
Results
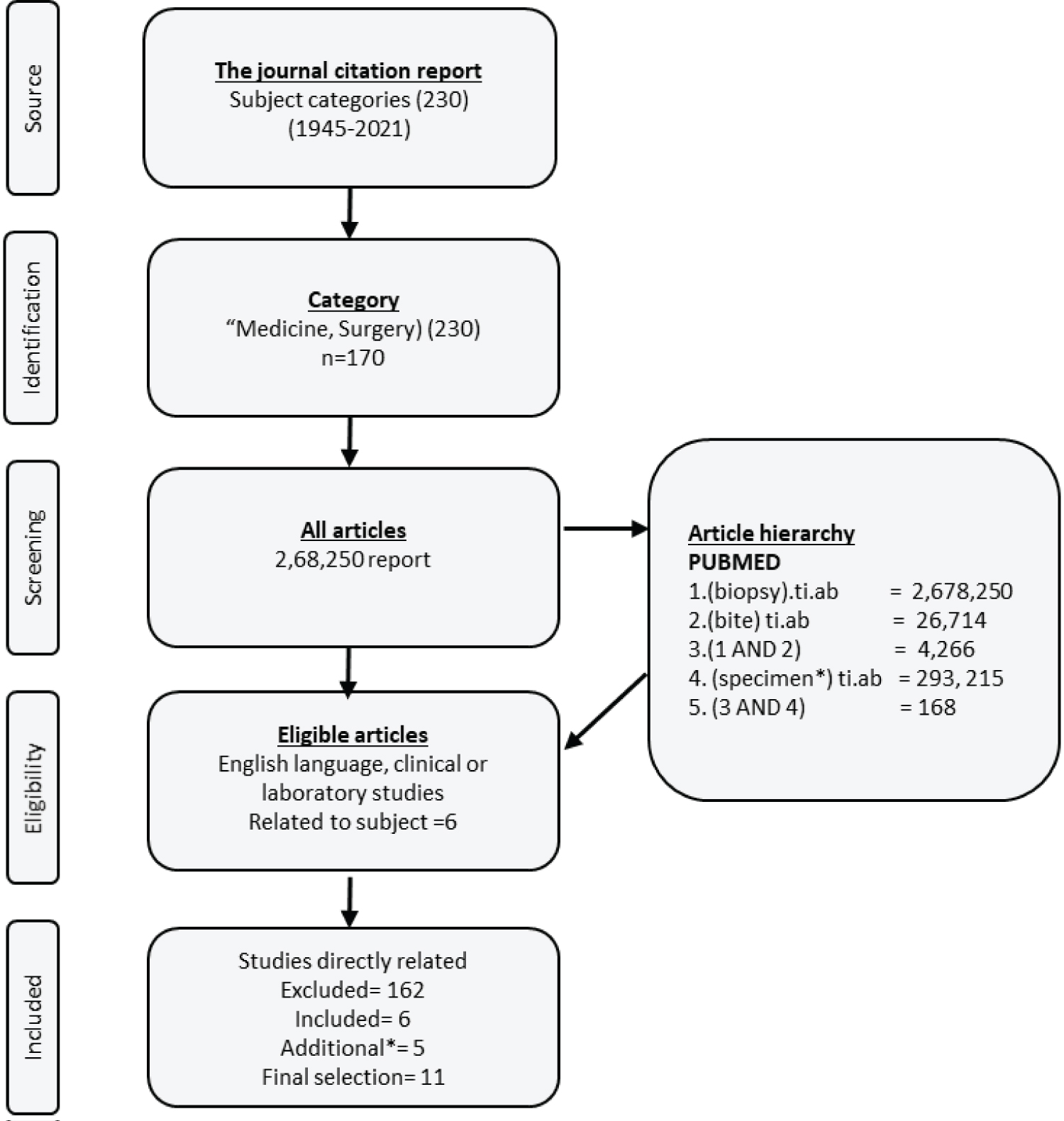
A total of 168 articles were identified from PubMed and after a detailed assessment, six papers met the search criteria. A further five were identified from google scholar and the final number of articles included in the study was 11. Figure 1 and Table 1 summarise the search strategy and results in a flow diagram.
Discussion
The studies cited above (Table 1) have all considered the issue of biopsy techniques i.e. SBB and DBB or multi-bite from different anatomic regions i.e. stomach, small or large intestine, in both human and animal models spanning different geographic regions across the world. Since the approach in studies is different the features will be highlighted in a thematic rather than chronological manner.
Comparison of protein quantity of biopsy specimen
Using a colorimetric technique, Frimberger, et al., [7] compared the protein content, a surrogate marker for adequacy of tissue, of biopsies collected through SBB (n = 79) and DBB (n = 79) techniques. Specimens were obtained from multiple regions i.e. Duodenum (n = 3), antrum (n = 10), corpus (n = 18), rectum (n = 30), sigmoid colon (n = 9) and colon (n = 9). They reported increased mean protein content (43%, p < 0.01) with DBB (66% specimens). Although, the study is a balanced randomised design with representative samples from all regions, it used an indirect assessment of tissue quantity and may lack histopathological and clinical applicability, the main issues in question.
Studies comparing the histological qualities of biopsy specimens
Several studies have compared the histological quality of tissue specimens. Amaro, et al. [7] compared small bowel biopsies and reported overall superiority of SBB specimens but the biopsies were collected from the small intestine only. Similarly, Padda, et al., [8] in their prospective randomised study (n = 16) directly compared the histological quality of SBB (n = 96) and DBB (n = 196) biopsy and no histological differences were reported. The study was a well designed prospective analysis and used one pathologist, thus reducing intra-observer variability in reporting. It was, however, low powered and only collected species from two regions. Later, Fan tin and Colleagues [9] improved on the design by defining the term histological quality which included; diameter, depth, artefacts, orientation and diagnostic quality of specimen. They too did not report any difference between, SBB (n = 510) and DBB (n = 520).
Chu, et al., [10] in contrast to the above two studies, compared histological quality in terms of; size, crush artefact, depth, adequacy, weight and overall rating in biopsies collected with forceps with needles. It was a well-designed prospective study (n = 240) and the pathologists were blinded, but the study only compared only gastric biopsies. Anecdotally, gastric biopsies are easy to take. Following this, Zaidman, et al., [11] studied muliti-bite pelican forceps in collection of porcine specimens in a study (n = 2, biopsy = 36), comparing SBB, DBB and multi bite forceps and did not report major differences in histological quality. However the pathologists were not blind to the techniques of biopsy collection. This finding was confirmed in a conference paper (n = 142) [12] and by a study (n = 21) using canine specimens [13]. However the purpose of the quoted studies [9-11,13] was the comparison of different types of forceps per se, and not the technique i.e. SBB and DBB.
Studies comparing the histological quality in context of a defined GI pathology
Hookey, et al., [14] conducted a prospective equal arm randomised and blind study comparing the evaluation of histological specimens for dysplasia in ulcerative colitis (n = 12), in specimens (n = 468) collected through SBB and DBB. They noticed DBB specimens were comparatively inadequate for assessment of dysplasia when compared to tier counterpart, SBB (OR = 2.78, 95% CI 1.37 to 5.59; P = 0.005). The study design, conduct and methodology are different in that an important clinical outcome i.e. dysplasia detection was under question. Dysplasia is patchy in UC [15]. Which may mean that a specimen collection bias could have affected the study.
Latorre, et al., [16] in a prospective cohort and blinded study examined the histological orientation of the biopsy specimen obtained through either SBB or DBB from the duodenum of patients (n = 86) with suspected (n = 47%), known (n = 36%) Coeliac disease (CD) and (n = 17%) controls. SBB yielded well oriented specimens in 66% patients and DBB returned in 42% (p < 0.01) and matched pairs showed improved orientation with the SBB (OR 3.1; 95% CI, 1.5-7.1; P < 0.01). The study was well designed and blinded; however, similar to Hookey, et al., [14] it only examined one specific region. Furthermore, duodenal cap biopsy specimens which are useful in the diagnosis of CD were excluded [17].
Finally, Pappas, et al., [18] did not report any histological difference between biopsy technique (n = 48) in a surveillance study for hereditary diffuse gastric cancer.
Studies comparing the time taken to take biopsies
Several studies compared the time taken to collect biopsies. Zaidman, et al., [11] reported that SBB took relatively longer but it is noteworthy that this study was based on a canine model. A recent study, using gastric biopsies, compared time taken between the two techniques and reported reduced overall time for biopsies taken through DBB [18]. It may be noted that it is easy to take gastric biopsies hence time taken per biopsy cycle may well be constant and predictable, whereas, time taken for colonic and oesophageal biopsies may not be predictable per cycle. This is because of the technical difficulty in colonic biopsies if specimens are taken from a difficult fold or the endoscope reaches the target area on an unstable loop. Oesophageal biopsies are prone to loss or difficult to take.
Studies comparing the specimen loss
Specimen loss was an aim in several studies. Although, Frimberger and colleagues [6] reported relatively less specimen loss with spiked forceps it was not the comparison of technique per se. Padda, et al., [8] reported relatively increased first specimen loss (25%, p = 0.02) with DBB and the loss was worse with non-spiked forceps (28.1% vs. 13.3%; p = 0.01). It is interesting to note that oesophageal samples were relatively more prone to loss as compared to gastric specimens. Although Stren, et al., [12] has referred to significant sample loss with DBB technique, figures given are not objective. Hookey and colleagues [14] reported that 14 biopsy specimens (6.0%) were lost in DBB as compared to eight (3.4%) SBB specimens (OR 1.8, 95% CI 0.69 to 5.04; P = 0.27). An objective comparison of lost specimens needs to be undertaken using different regions in a randomised study.
Material and Methods
This seems an odd place to put this after the results.
Literature and search strategy
A scoping literature search was conducted in September 2021 using PUBMED. The following terms were applied, searching for titles and abstract (TiAb): (biopsy).TiAb, AND bite AND specimen. Moreover, using the same search terms in Google scholar further unique articles (n = 5) were identified. Additionally, one conference presentation was also included.
Ethical approval
No ethical approval was required for this scoping review.
Conclusion
There is significant methodological inconsistency and variations in the studies cited above. Frimberger, et al., [6] used multiple regions but their study lacked clinical application as they measured protein content only. Other studies have been based on animal models [10,11]. Some authors have compared techniques indirectly [9,13].
The exact clinical value of either taking DBB or SBB is not clear from the studies cited above. This is because, using a large prospective sample, none has specifically assessed the diagnostic or prognostic value of these techniques but one may infer that taking biopsies by either method does not matter much.
There is a lack of a clinical study which, simultaneously, taking multi-regional samples, examines histological adequacy, time taken to complete the biopsy cycles and specimen loss in a holistic manner. This will, as anticipated, give clear guidance to the endoscopists to adapt a standardised method of taking endoscopic samples.
Authors' Contribution
Conceptualization: HM, SO, JFM; Methodology: HM, SR, SA, JFM; Formal analysis: HM, SA, SO JFM; Writing original draft preparation: HM, SO; writing review and editing: HM, SO, SA, JFM.
All authors have read and agreed to the published version of the manuscript.
Funding
This review article received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Burke KE, D'Amato M, Ng SC, et al. (2021) Microscopic colitis. Nat Rev Dis Primers 7: 39.
- Battat R, Casteele NV, N, Pai RK, et al. (2020) Evaluating the optimum number of biopsies to assess histological inflammation in ulcerative colitis: A retrospective cohort study. Aliment Pharmacol Ther 52: 1574-1582.
- Fitzgerald RC, Di Pietro M, Ragunath K, et al. (2014) British society of gastroenterology guidelines on the diagnosis and management of Barrett's oesophagus. Gut 63: 7-42.
- Das P, Vaiphei K, Amarapurkar AD, et al. (2021) Best practices of handling, processing, and interpretation of small intestinal biopsies for the diagnosis and management of celiac disease: A joint consensus of Indian association of pathologists and microbiologists and Indian society of gastroenterology. Indian J Pathol Microbiol 64: S8-S31.
- Lim C, Choi M, Kim WC, et al. (2000) Performance and cost of disposable biopsy forceps in upper gastrointestinal endoscopy: Comparison with reusable biopsy forceps. Clin Endosc 45: 62-66.
- Frimberger E, Becker P, Roesch T, et al. (2000) 7121 Double bite biopsy-a method to save biopsy time in endoscopy. Gastrointest. Endosc 51: AB272.
- Amaro R, Lubin J, Barkin JS (2000) 4744 Endoscopic small intestine biopsy: Comparison of two techniques. Gastrointestinal Endoscopy 51: AB219.
- Padda S, Shah I, Ramirez FC (2003) Adequacy of mucosal sampling with the "two-bite" forceps technique: A prospective, randomized, blinded study. Gastrointest Endosc 57: 170-173.
- Fantin AC, Neuweiler J, Binek JS, et al. (2001) Diagnostic quality of biopsy specimens: Comparison between a conventional biopsy forceps and multi bite forceps. Gastrointest Endosc 54: 600-604.
- Chu KM, Yuen ST, Wong WM, et al. (2003) A prospective comparison of performance of biopsy forceps used in single passage with multiple bites during upper endoscopy. Endoscopy 35: 338-342.
- Zaidman JS, Frederick WG, Furth EE, et al. (2006) Comparison of Pelican single-use multi bite biopsy forceps and traditional double-bite forceps: Evaluation in a porcine model. Gastrointest Endosc 64: 582-588.
- Stern JE, Greenwald DA, Ochoa E, et al. (2005) "Single-Bite" Versus "Double-Bite" Biopsy Specimens: Is There a Difference? Gastrointest Endosc 61: AB123.
- Edery EG, Scase T, Kisielewicz C, et al. (2018) Comparison of standard single-bite with multiple-bite biopsy forceps for collection of gastrointestinal biopsies in dogs: A prospective study. Vet Rec 183: 624.
- Hookey LC, Hurlbut DJ, Day AG, et al. (2007) One bite or two? A prospective trial comparing colonoscopy biopsy technique in patients with chronic ulcerative colitis. Can J Gastroenterol 21: 164-168.
- Allen DC, Biggart JD, Pyper PC (1985) Large bowel mucosal dysplasia and carcinoma in ulcerative colitis. J Clin Pathol 38: 30-43.
- Latorre M, Lagana SM, Freedberg DE, et al. (2015) Endoscopic biopsy technique in the diagnosis of celiac disease: One bite or two? Gastrointest Endosc 81: 1228-1233.
- Murch S, Jenkins H, Auth M, et al. (2013) Joint BSPGHAN and Coeliac UK guidelines for the diagnosis and management of coeliac disease in children. Arch Dis Child 98: 806-811.
- Pappas A, Tan WK, Waldock W, et al. (2021) Single-bite versus double-bite technique for mapping biopsies during endoscopic surveillance for hereditary diffuse gastric cancer: A single-center, randomized trial. Endoscopy 53: 246-253.
Corresponding Author
Humayun Muhammad, Department of Life Science, University of Roehampton, UK.
Copyright
© 2022 Muhammad H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.