Mucocele of the Appendix: A Case Report
Abstract
Appendicular mucocele is an infrequent entity that constitutes a descriptive term to define an enlarged cecal appendix with accumulation of mucus in its interior, which can be due to both neoplastic and non-neoplastic causes.
Patients are usually asymptomatic, becoming an incidental finding. However, in other cases the symptoms are highly variable (abdominal pain, palpable abdominal mass, digestive bleeding...) and differential diagnosis can become a challenge.
In this way, imaging studies as ultrasound (US), computed tomography (CT) or magnetic resonance imaging (MRI) play an important role in preoperative diagnosis, since they provide information that can be decisive when it comes to select the most appropriate surgical intervention modality.
We report a case of a patient who presented an incidental mass in lower right quadrant that turned out to be an appendicular mucocele.
Introduction
Mucocele of the appendix is a rare entity that is found in less than 1% of appendectomies. Historically, this pathology appears more frequently in middle-aged patients and its incidence is higher in females (4:1). The majority of patients are asymptomatic, but in other cases diverse clinical manifestations such as abdominal pain, a palpable mass or gastrointestinal bleeding can be present.
This entity has to be included in the differential diagnosis of cystic lesions located in the right iliac fossa. In addition, it is important to remember the importance of the various imaging studies available in order to establish both preoperative diagnosis and most appropriate type of surgical intervention.
Case Presentation
A 72-year-old woman with a history of hypertension, ischemic heart disease and chronic gastritis was referred to the emergency department of our hospital with complaints of abdominal pain located in the right iliac fossa for several days associated with nausea and low-grade fever.
Physical examination revealed the existence of an elastic tumor in the right hemiabdomen. The mass was slightly painful and not displaceable. Except for minor alterations in the analysis (mild leukocytosis and neutrophilia), no other abnormalities could be found.
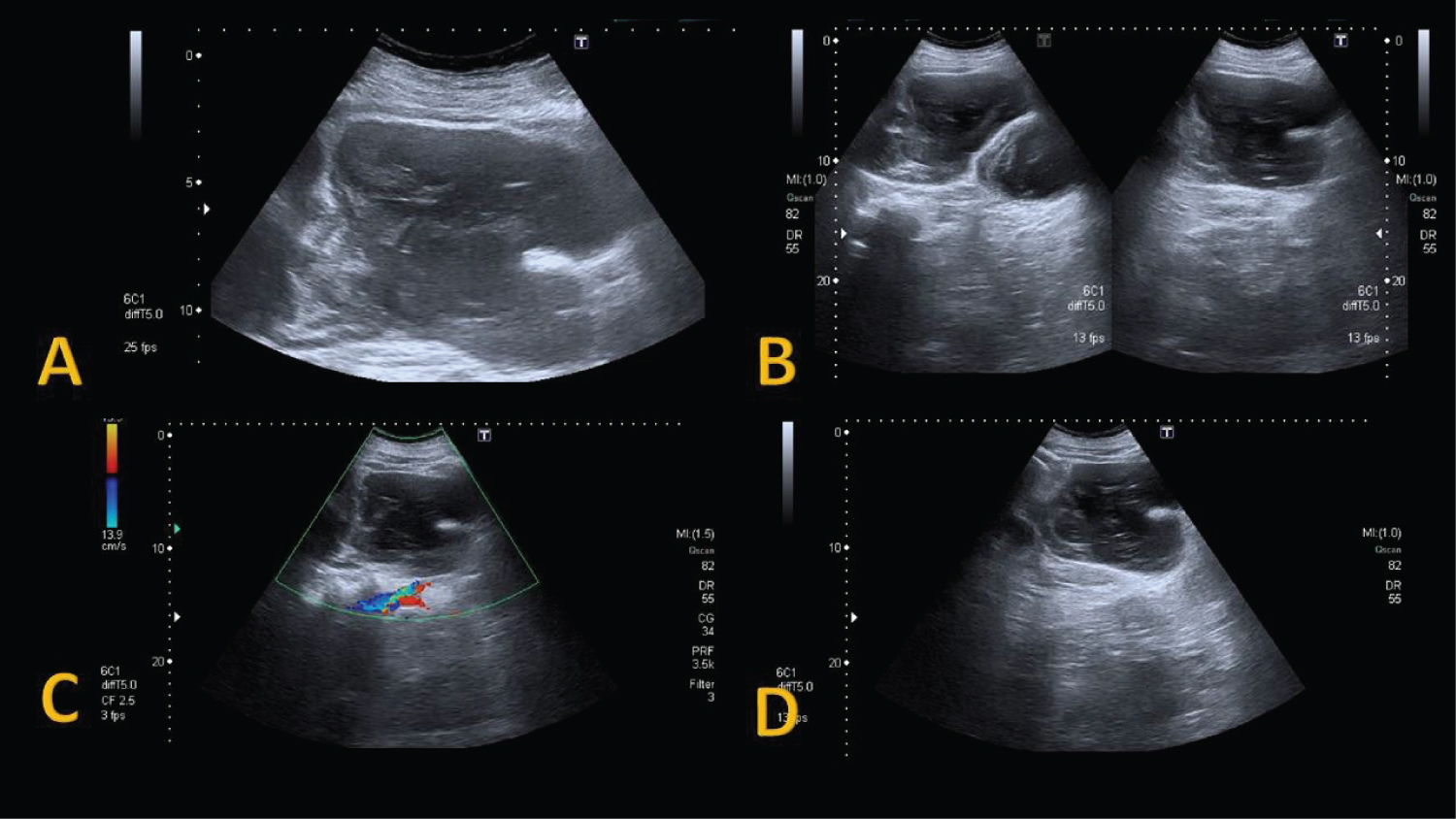
Given the suspicion of acute appendicitis, an urgent abdominal ultrasound was requested. US showed up a large, heterogeneous and polylobulated mass with multiple internal septa located in lower right quadrant (Figure 1). These findings suggested the possibility of adnexal tumor. The patient was discharged and a complementary CT study was scheduled in the following week.
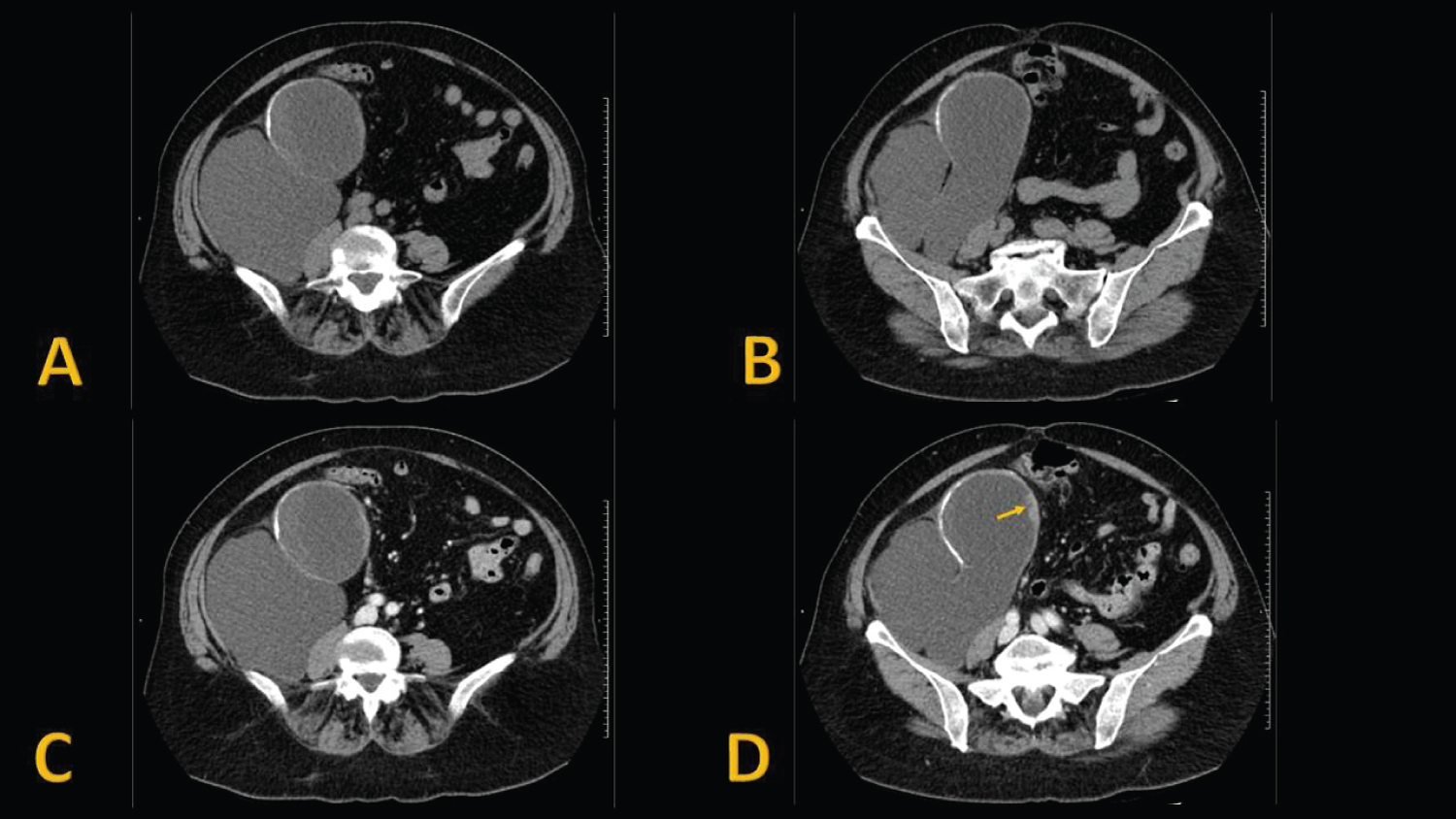
CT findings showed up a voluminous and low-attenuation cystic mass located on the right flank and right iliac fossa, losing plane of separation with the cecum (Figure 2). These findings suggested an appendicular mucocele.
Given the imaging findings, the patient underwent surgery and a right hemicolectomy was performed. The histopathological study confirmed an appendicular mucinous neoplasm with several high-grade dysplasia foci compatible with mucinous cystadenocarcinoma. She was discharged 2 days after surgery.
She was put on regular follow-up and did not receive any other treatments. The patient was asymptomatic and had no recurrence on follow up.
Discussion
Appendicular mucocele (AM) is a macroscopic description of an appendix abnormally distended by mucin [1]. It constitutes a rare entity found in 0.2%-0.3% of appendectomy specimens and in 8% of appendiceal tumors and they typically appear in middle-aged female patients (4:1) [2].
Mucocele in the appendix may be classified according to the histological characteristics in four different subtypes: simple or retention mucocele, hyperplastic mucocele, mucinous cystadenoma and mucinous cystadenocarcinoma [3]. Histological subtype as well as the extent of dissemination consist significant prognostic factors.
In general, most patients are asymptomatic and appendicular mucocele appears as an incidental finding during surgical act, endoscope or imaging studies performed for other reasons [2]. However, other patients can be symptomatic presenting various clinical manifestations such abdominal pain located in the right iliac fossa, a palpable pelvic mass, weight loss or gastrointestinal bleeding. Other symptoms appear related to complications of appendicular mucocele (intussusception, acute appendicitis or pseudomyxoma peritonei). Symptomatic manifestation from superinfection of a mucocele can be clinically indistinguishable from nontumoral acute appendicitis [4].
Preoperative diagnosis of appendicular mucocele is very important for the selection of an adequate surgical method to prevent peritoneal dissemination, to prevent intraoperative and postoperative complication, and repeated surgery [5]. Imaging techniques as ultrasound (US), computed tomography (CT) or magnetic resonance imaging (MRI) are quite useful in order to evaluate the full extent of the lesion [4]. Also, these studies are essential to spot serious complications such as an accidental rupture with the subsequent diffuse intraperitoneal accumulation of gelatinous material and development of a pseudomyxoma peritonei, which is potentially lethal [2].
Most frequent form of presentation in US examination is a cystic mass with variable internal echogenicity depending on the composition of the mucinous element. Features highly suggestive of a mucocele are internal concentric echogenic layers, acoustic shadowing, and a pear-shaped appearance [1]. Frequently these lesions do not show vascularization on Doppler ultrasound. However, although ultrasound is considered as primary diagnostic tool, US findings are not specific and the differential diagnosis might include ovarian neoplasms, lymphoma, enteric duplication, mesenteric cysts and hydrosalpinx [4,6].
CT is the preferred modality for evaluating mucoceles of the appendix. AM presents as a well circumscribed spheric or tubular low-attenuation mass contiguous with the base of the cecum. The presence of curvilinear mural calcification is highly suggestive of the diagnosis, but this finding only appears in less than 50% of cases [4,6]. Soft-tissue thickening and irregularity of the mucocele wall, intraperitoneal fluid and surrounding fat stranding are nonspecific findings that suggest malignancy, secondary inflammation, or both [4]. Nevertheless, we must keep in mind that CT findings of acute appendicitis with associated mucocele can overlap those of the pathological condition without additional appendiceal lesion [6].
Treatment is always surgical, but there are different options are considered depending on each case. If benign appendicular mucocele is suspected (negative resection margins and resection without perforation), a simple appendectomy is preferred. In other hand, in patients with suspicion of malignancy through imaging studies (large size, wall enhancement...), signs of perforation, positive excision margins, positive cytology or involvement of appendiceal lymph nodes, a right hemicolectomy and cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy or early post-operative intraperitoneal chemotherapy should be considered [6].
In our case, clinical and analytical findings were suggestive of acute appendicitis. As we mentioned above, imaging tests showed up some findings highly suggestive of AM and were decisive to classify the lesion as a probably malignant appendicular mucocele, allowing an early diagnosis and helping in order to establish the surgical approach. Our patient underwent a right hemicolectomy and the histopathological exam demonstrated an appendicular mucinous neoplasm with several high-grade dysplasia foci compatible with mucinous cystadenocarcinoma.
In conclusion, appendicular mucocele is a rare disease which may have a clinical picture highly variable and can resemble acute appendicitis [3]. Therefore, this entity must be present in the differential diagnosis of an acute abdominal pain located in right iliac fossa. Presurgical radiologic diagnosis of a mucocele is important and helps determine the surgical approach [2]. However, the final diagnosis of a benign or malignant tumor will be definitely established by the histopathological examination of the surgical piece.
References
- Leonards L, Pahwa A, Patel M, et al. (2017) Neoplasms of the appendix: Pictorial review with clinical and pathologic correlation. RadioGraphics 37: 1059-1083.
- Honnef I, Moschopulos M, Roeren T (2008) Appendiceal mucinous cystadenoma. RadioGraphics 28: 1524-1527.
- BB SK, Jasuja P (2019) Appendiceal mucocele-a rare case report. Int J Surg Case Rep 58: 21-25.
- Pickhardt P, Levy A, Rohrmann C, et al. (2003) Primary neoplasms of the appendix: Radiologic spectrum of disease with pathologic correlation. RadioGraphics 23: 645-662.
- Demetrashvili Z, Chkhaidze M, Khutsishvili K, et al. (2012) Mucocele of the appendix: Case report and review of literature. Int Surg 97: 266-269.
- Mastoraki A, Sakorafas G, Vassiliu P, et al. (2016) Mucocele of the appendix: Dilemmas in differential diagnosis and therapeutic management. Indian J Surg Oncol 7: 86-90.
Corresponding Author
Blanca Prieto García, Servicio de Radiodiagnóstico, Complejo Asistencial Universitario de Salamanca, Spain.
Copyright
© 2020 García BP, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.