Acute Cholecystitis in a True Left-Sided Gallbladder - A Case Report
Abstract
We describe our experience with a 69-year-old gentleman who presented with phlegmonous acute cholecystitis affecting a left-sided gallbladder. The cholecystectomy was successfully completed by a total laparoscopic approach. Through this Case report we highlight the possibility of occurrence of such an entity (true left-sided gallbladder), the risks entailed, and to stress the need to abandon surgical hubris in favour of wisdom in the interest of patient safety should the situation appear unclear and overtly challenging to the surgeon.
Keywords
Anatomy, Laparoscopy, Bile duct, Outcomes
Introduction
The normal anatomical location of the gallbladder is within the fossa formed by segments IVb and V of the liver to the right of the ligamentum teres. The radiological and/or clinical surprise of finding a gallbladder located to the left of the ligamentum teres is broadly referred to as a left-sided gallbladder [1]. While left-sided gallbladders may be the result of situs inversus or due to an abnormally located ligamentum teres, true left-sided gallbladders are an even less common within this broad spectrum. Either way, they present a challenge to surgeons especially when encountered in the setting of emergency surgery. Given the increased association with aberrant biliary and vascular anatomy, cholecystectomy for left-sided gallbladders have a higher than normal risk of bile duct injury. We present our experience in a patient who presented with phlegmonous acute cholecystitis affecting a true left-sided gallbladder.
Case Report
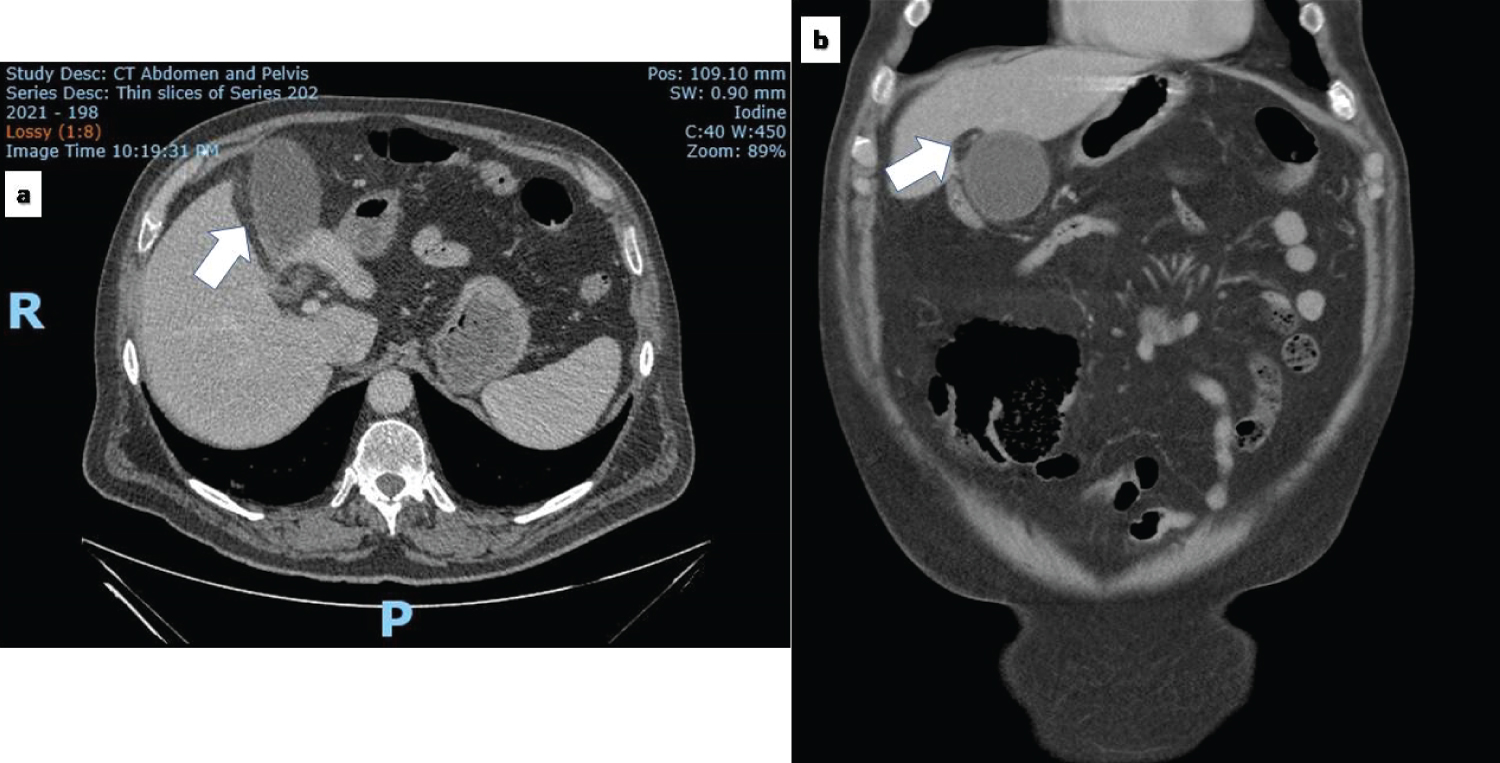
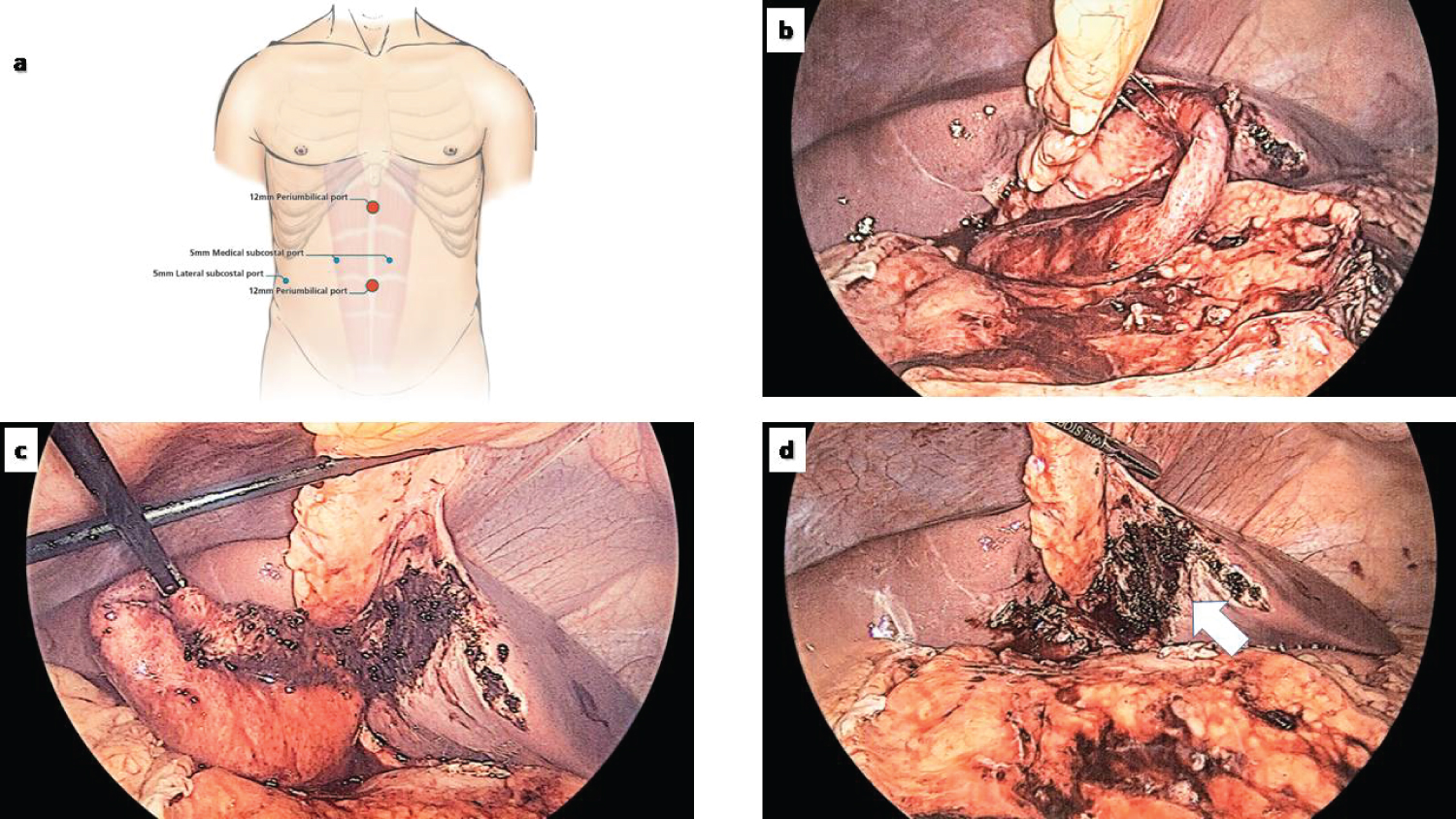
A 69-year-old gentleman presented to the emergency department close to midnight with a two-day history of right upper quadrant and epigastric pain. The pain was steadily increasing in severity with a change in character from an initial colic to a more constant dull ache. He reported feeling febrile and vomiting ingested food and bile as a result of the pain. On clinical examination, the patient was afebrile but tender with voluntary guarding in the right hypochondrium and epigastric regions. A contrast-enhanced computed tomography scan of the abdomen and pelvis confirmed radiological features consistent with acute cholecystitis secondary to a calculus impacted in the neck of the gallbladder. The patient was fasted and commenced on intravenous antibiotics with a plan for an emergency laparoscopic cholecystectomy the following morning. Intraoperatively, he was found to have a large phlegmon involving the gallbladder comprising the omentum, stomach and duodenum. On bluntly peeling the omentum away from the gallbladder, it was noticed that the patient's gallbladder was almost entirely situated to the left of the falciform ligament attached to segment III. The gallbladder was turgid, partly intrahepatic (Figure 1), and appeared ischaemic with fibrin exudates adherent to it. After a controlled decompression of the gallbladder with a Veress needle, it was deemed necessary to insert an additional port to the left of the midline (Figure 2a) to facilitate dissection. Given the atypical anatomical location and the extent of inflammation in the porta, the gallbladder was dissected fundus first, off segment III as this would later enable its retraction towards the right-hand side of the patient better displaying the portal structures over which the gallbladder appeared to be draped (Figure 2b and Figure 2c). A grasper inserted via the right lateral subcostal port (5 mm) was initially only used to retract the falciform ligament to allow both medial subcostal ports to serve as working channels. A combination of blunt and sharp (diathermy) dissection was used to dissect the gallbladder off the falciform ligament. The gallbladder appeared to arise to a smaller extent from the left lobe of the liver (Figure 2d). In view of the cystic duct that was isolated by blunt dissection leading directly posteriorly into the common hepatic duct, the severe extent of inflammation in the region, and normal preoperative liver functions, the decision was taken not to perform an intraoperative cholangiography. The cystic duct was clipped and divided and the cystic artery running in the left wall of the gallbladder was also clipped and divided. A 15Fr Blake's drain was left in Morisson's pouch. The patient made an uneventful recovery and was discharged on post-operative day 2 after removal of the drain, with normal liver function tests. Histology confirmed acute cholecystitis with areas of ulceration and necrosis.
Discussion
There are less than 200 reported cases in literature of gallbladders attached to the left side of the liver [1,2]. However, the true incidence is believed to be 0.2 to 1.1% [3]. This implies that while not often reported in textbooks [4] as an anatomical abnormality of the gallbladder, the location of the gallbladder on the left side is not uncommon. When considering left-sided gallbladders it is important to appreciate that the true left-sided gallbladders (as in this report) are far less common than a left-sided gallbladder occurring in conjunction with situs viscerum inversus or an abnormally-located right-sided round ligament [5]. Either way, the clinical relevance of such an anatomical abnormality lies in the appreciation that such an anomaly is associated with an increased risk of bile duct injuries (7.3%) [1] compared to a rate of up to 0.6% noted for all cholecystectomies [6]. This could either be due to the relatively intrahepatic location of the gallbladder in the region of the umbilical fissure (as noted in this report), the unpredictable confluence of the cystic duct into the common bile duct (direct posterior insertion in this patient) and the variable vascular anatomy [7]. While laparoscopic cholecystectomy may be feasible, the presence of severe inflammation must warrant caution and attention to detail with the surgery preferably being performed by an advanced laparoscopic surgeon. Maintaining patient safety as the utmost goal, the surgeon must constantly attempt to reorient oneself with the portal anatomy and revisit in his/her mind options available including conversion to open and the selective use of intraoperative cholangiography [1] if the confusing anatomy or the extent of inflammation precludes safe dissection.
Conclusions
True left-sided gallbladders are an uncommon entity under the spectrum of gallbladders located to the left of the falciform ligament. There is need to create awareness of this entity owing to it being increasingly reported in literature and the lack of preoperative diagnosis in most cases [8]. The altered extra-hepatic biliary and vascular anatomy poses a challenge more so in the setting of acute inflammation. Diligent dissection, appropriate technique and surgical wisdom in knowing when to convert to open are aspects that need to reverberate with surgeons faced with a left-sided gallbladder.
Acknowledgement
David Summerhayes and Eric Lum for help with the illustrations in the manuscript.
Conflict of Interests
None to declare.
Role of Funding Source
Not applicable.
Ethics Committee Approval
Not applicable.
Authors Declaration
Informed consent was obtained from the patient for the Case Report.
References
- HK Abongwa, B De Simone, L Alberici, et al. (2017) Implications of left-sided gallbladder in the emergency setting: Retrospective review and top tips for safe laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech 27: 220-227.
- T Saafan, JY Hu, AE Mahfouz, et al. (2018) True left-sided gallbladder: A case report and comparison with the literature for the different techniques of laparoscopic cholecystectomy for such anomalies. Int J Surg Case Rep 42: 280-286.
- E Savier, J Taboury, O Lucidarme, et al. (2005) Fusion of the planes of the liver: An anatomic entity merging the midplane and the left intersectional plane. J Am Coll Surg 200: 711-719.
- PG Jackson, SRT Evans (2017) Biliary system. In: CM Townsend, RD Beauchamp, BM Evers, et al. Sabiston Textbook of Surgery. (edn), The Biological basis of Modern Surgical Practice, Elsevier.
- M Nagai, K Kubota, S Kawasaki, et al. (1997) Are left-sided gallbladders really located on the left side? Ann Surg 225: 274-280.
- JT Cohen, KP Charpentier, RE Beard (2019) An update on iatrogenic biliary injuries: Identification, classification, and management. Surg Clin North Am 99: 283-299.
- PK Reddy, RV Subramanian, S Yuvaraja (2005) Laparoscopic cholecystectomy for left-sided gallbladder (Sinistroposition). JSLS 9: 356-357.
- RW Strong, J Fawcett, M Hatzifotis, et al. (2013) Surgical implications of a left-sided gallbladder. Am J Surg 206: 59-63.
Corresponding Author
Savio George Barreto, Division of Surgery and Perioperative Medicine, Flinders Medical Centre, Bedford Park, Adelaide, South Australia, Australia; College of Medicine and Public Health, Flinders University, South Australia, 5042, Australia, Tel: +61-8-82045511
Copyright
© 2020 Barreto SG, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.