A Giant Bleeding Pancreatic Pseudocyst after a Blunt Traumatism in a Thirteen Year-Old Child
Abstract
A thirteen-year-old boy presented with a grade IV blunt pancreatic traumatism with a cephaloisthmic disjunction. A giant pancreatic pseudocyst was developed and complicated with a massive intracystic bleeding. An evacuation and drainage of all collections was performed by laparotomy. Intracystic bleeding is rare but potentially letal, CT/MRI and selective angiography lead to a better management. Surgical treatment may be confined to recurrent, multiple or > 200 mm pseudocysts.
Keywords
Pancreatic traumatism, Pancreatic pseudocyst, Intracystic bleeding, Chemical peritonitis
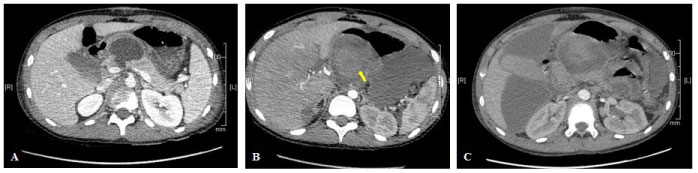
A thirteen-year-old boy presented with a grade IV blunt pancreatic traumatism with a cephaloisthmic disjunction secondary to an impact on his bicycle handlebar. As expected, he developed a pancreatic pseudocyst measuring 170 × 86 × 18 cm (Figure 1A: CT scan at day 14 showing uncomplicated pseudocyst and the pancreatic trauma). Whereas he was only slightly symptomatic, he presented at day 15 an acute and massive intracystic bleeding by erosion of the posterior pancreaticoduodenal artery (Figure 1B: CT scan demonstrating an active intracystic bleeding with a dramatic increased size). A radiological embolization of the proximal gastroduodenal artery allowed hemodynamic stabilization of the patient. He secondary developed a compartmental syndrome of the abdomen with an active pancreatic leakage and chemical peritonitis (Figure 1C: multifocal peritonitis with sequestrated pseudocyst, an old hematoma and hydro-hydric levels). The surgical evacuation and drainage of all the collections were performed by laparotomy. The pancreatitis and the ductal fistula eventually had a slow but favorable outcome.
Children pancreatic injury is the fourth solid organ injury in blunt abdominal trauma, following the spleen, liver and kidneys. Pseudocyst is a frequent complication. The presence of a ductal injury is a strong predictor of failure of nonoperative treatment [1]. However, severe injury of the pancreatic head can be managed expectantly, limiting drainage to symptomatic or > 50 mm pseudocysts [2]. Surgical treatment may be confined to recurrent, multiple or giant (> 200 mm) pseudocysts [3]. Intracystic bleeding is rare but potentially lethal, CT/MRI and selective angiography lead to a better management.
References
- Mattix KD, Tataria M, Holmes J, et al. (2007) Pediatric pancreatic trauma: Predictors of nonoperative management failure and associated outcomes. J Pediatr Surg 42: 340-344.
- Patty I, Kalaoui M, Al-Shamali M, et al. (2001) Endoscopic drainage for pancreatic pseudocyst in children. J Pediatr Surg 36: 503-555.
- F Nouira, Y Ben Ahmed, N Sarrai, et al. (2011) Les pseudokystes du pancréas chez l'enfant: Quelle approchethérapeutique? Pancreatic pseudocyst in children: What is the best therapeutic approach? Arch Pediatr 18: 1176-1180.
Corresponding Author
Verónica Alonso, Pediatric Surgery Department, Hospital Clínico Universitariode Valladolid Av. Ramón y Cajal, 3, 47003 Valladolid, Spain, Tel: +34-983-42-00-00.
Copyright
© 2019 Alonso V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.