Impact of C-level Executives' Leadership Styles in the Healthcare Organizations
Abstract
Objective: To evaluate how the leadership styles of C-level Executives correlate with the hospital's ratings.
Methods: A qualitative study design was utilized for this study.
Results: Participants who practiced servant leadership style had reported overall highest ratings and profitability.
Conclusions: There is a correlation among those who practiced servant leadership styles.
Is the C-level Executive's leadership style important for a healthcare organization's success? Leadership is an extensively debated topic, with countless papers and books devoted to its research and appraisal, as well as its influence on team development, team performance, and team dynamics. One of the most essential elements in increasing an organization's overall performance is its leadership. The leadership style of C-level Executives dictates the organization's culture, overall performance, and financial stability. This study analyzes through the prism of several leadership styles, with a particular focus on four main leadership styles among the C-level Executives. Leadership styles have a strong association with an organization's success because how a leader manages their team determines the organization's overall performance. For example, experts believe that productivity can grow indirectly, especially among employees, who feel that they are a part of an input, which inspires them. According to the researchers, it all comes down to human behavior and psychological beliefs when it comes to selecting the right leadership style for a company [1]. This purpose of this study was to examine the influence of leadership on a hospital's overall rating, safety grade ratings as well as an annual financial audited statement.
Literature Review
The literature is replete with leadership research studies; conversely, there is a limited number of studies that highlight the impact of C-level Executives leadership styles on the hospital's overall ratings and safety grade ratings. The subsequent section of this article describes four main leadership styles.
Visionary
Visionary style leadership sets an example for communities or organizations by communicating their vision and inspiring rather than controlling. True visionary leaders empower their subordinates to figure out the best way to attain their goals while also realizing that it would take a lot of discipline and dedication to achieve them. These leaders are persistent, motivational, magnetic, open-minded, inventive, imaginative, courageous, collaborative, goal-oriented, well-organized, passionate, responsible, and emotionally aware.
Servant
The servant leader, according to Greenleaf, "begins with the natural impulse to serve, to serve first" and then "intensifies to lead." Servant leadership comprises a set of leadership behaviors as well as a set of leadership traits. This leader is deeply concerned about the needs of others, and he or she will most likely prioritize the interests of followers before their own [2].
Transformational
This leadership style encourages and empowers followers to attain their goals by instilling a feeling of purpose in them. This type of leader demonstrates integrity, emotional intelligence, self-awareness, honesty, empathy, and humility [3]. Individuals who aren't aligned with the organization's vision, risk-taking, and thinking outside the box attitude may have conflicts and challenges as a result of transformational leadership.
Situational
Paul Hersey and Ken Blanchard described this style as adapting to changing conditions. This method might be used in various different settings i.e., academia, corporate, and hospitals. This sort of leader must be adaptive and this kind of leadership needs the capacity of the leader to adapt to changing circumstances; else, it will fail.
Method
Study design
By design, this study can be classified as qualitative research. A previously developed leadership research tool was utilized to evaluate the leadership styles of the participants for this research. A trial study was conducted with a number of subjects to validate the accuracy of the tool. These participants had already explored their leadership style using various corporate tools and instruments. A convenience sampling approach was taken for this particular research. For example, fifty-five hospitals in the Tri-state area were contacted to take part in this study. The research was designed to be voluntary and participants were not required to complete the interview if they chose not to. The inclusion criteria for this study were that the participants needed to hold a C-level Executive position in the Tri-state area. Once the participants agreed to partake in the study, the research purpose, direction of taking part in the study, inclusion criteria, and a timeline were shared with the participants. This research allowed the flexibility to interpret the data rigorously and conscientiously while exploring the emerging themes [4].
Data collection & data analysis
Sixty minutes interviews were conducted using a combination of direct and open-ended questions. All participants were asked the same questions for this research study to avoid bias. Each participant was interviewed only once. All interviews were transcribed verbatim. Transcriptions were stored securely to keep participants' anonymity and confidentiality. Interpretation of the data took place once all the interviews were completed. During this time, the process and sampling were checked to see if there were any adjustments needed. Hospital's overall rating, safety grades, and financial audit statements were obtained from open databases i.e., Medicare and Leapfrog. Data were analyzed and summarized using descriptive statistics. Statistical analysis was done using the Statistical Package for Social Sciences (SPSS) software, Version 28.0.
Ethical considerations
The study did not require full Institutional Review Board (IRB) approval because it utilized publicly available databases and did not include any personal identifiers; however, participants were contacted after obtaining Drexel University IRB approval. All participants voluntarily took part in the study and could've opted out of this study at any point. Informed verbal consent was obtained before the observations and interviews.
Results
Demographic
The ultimate response rate for the study was hundred percent (n = 23). Seventy (n = 16) percent of the facilities were from Pennsylvania (PA), twenty-two (n = 5) percent from New Jersey (NJ), and nine (n = 2) percent from New York (NY). It was determined that eighty-three (n = 19) percent of participants were females and seventeen (n = 4) percent were male. Sixty-one (n = 14) percent participants were from magnet and thirty-nine (n = 9) percent were from non-magnet hospitals. Ninety-one (n = 21) percent of participants were Caucasians, four (n = 1) percent were African-American, and the remaining four (n = 1) percent preferred not to answer. Eighty-three (n = 19) percent of participants had a doctorate level degree and the remaining seventeen (n = 4) percent had a master's degree. Fifty-two (n = 12) percent participants were Chief Nursing officers (CNOs), twenty-two (n = 5) percent were Chief Operating Officers (COOs), nine (n = 2) percent were Chief Executive Officers (CEOs), and the remaining seventeen (n = 4) percent participants were titled Executives (See Table 1).
Fifty-two (n = 12) percent of hospitals had an average (3-Stars) to excellent (5-Stars) overall rating. Thirty-nine (n = 9) percent had below-average (2-Stars) to poor (1-Star) overall rating. The remaining nine (n = 2) percent did not have any reporting. Fifty-two (n = 12) percent of the hospitals had the highest safety grade of an "A." Thirty-five (n = 8) percent had safety grades of "B" and "C." The remaining thirteen (n = 3) percent had safety grades of "D" or either it was not listed. Sixty-five (n = 15) percent of hospitals' yearly audited financial statements showed profitability; whereas, thirty (n = 7) percent of hospitals' yearly audited financial statements did not show profitability. The remaining hospital's profitability was not accessible (See Table 2).
Participants leadership styles
The major leadership style themes that emerged from this study were servant, situational, transformational, and visionary. Pre-interview sixty-one (n = 14) percent thought that they practiced transformational, seventeen (n = 4) percent believed they practiced situational, and thirteen (n = 3) percent believed that they practiced servant leadership style. The remaining nine (n = 2) percent thought they practiced the visionary leadership style. Post-interview it was determined that thirty-nine (n = 9) percent of the participants practiced servant, thirty-five (n = 8) percent practiced situational, seventeen (n = 4) percent practiced transformational, and the remaining nine (n = 2) percent practiced visionary leadership style (See Table 3).
Servant leadership style
Out of the thirty-nine (n = 9) percent of participants who practiced servant leadership style, seventy-eight (n = 7) percent executives had 3-Stars to 5-Stars overall hospital ratings as well as the highest safety grade rating of an A. Four (n = 1) percent of the participant who practiced servant had a safety grade rating of C and the remaining four (n = 1) percent ratings were not reported. Hundred (n = 9) percent of those who practiced servant leadership style had reported increased profitability in the yearly audited financial statements.
Situational leadership style
Out of the thirty-five (n = 8) percent of participants who practiced situational leadership style, fifty (n = 4) percent had an overall rating of 4-Stars and 5-Stars and the remaining fifty (n = 4) percent had 2-Stars overall ratings. Fifty (n = 4) percent of the participants who practiced situational had the highest safety grade ratings of an A. Forty-two (n = 3) percent of the participants who practiced situational had safety grade ratings of B. Remaining fourteen (n = 1) percent practiced situational had safety grade ratings of C. Fifty (n = 4) percent of those who practiced situational leadership style had reported positive profitability through the financial statements.
Transformational leadership style
Out of the seventeen (n = 4) percent of participants who practiced transformational leadership style, hundred (n = 4) percent had 3-Stars to 1-Star overall hospital ratings. Twenty-five (n = 1) percent of the participants who practiced transformational had the highest safety grade ratings of B. Fifty (n = 2) percent of the participants had safety grade ratings of C. Remaining twenty-five (n = 1) percent had safety grade ratings of D. Twenty-five (n = 1) percent of those who practiced transformational leadership style had reported positive profitability through the financial statements. Fifty (n = 2) percent had reported a loss in their yearly audited financial statements and the remaining twenty-five (n = 1) percent financial statements were not accessible.
Visionary leadership style
Out of the nine (n = 2) percent of participants who practiced visionary leadership style, hundred (n = 2) percent had 3-Stars to 1-Star overall hospital ratings. Fifty (n = 1) percent of the participants who practiced visionary leadership style had the highest safety grade ratings of an A; whereas, the remaining fifty (n = 1) percent of the participants had safety grade ratings of D. Fifty (n = 1) percent had reported profitability in their yearly audited financial statements and remaining fifty (n = 1) percent reported loss in their yearly financial statement. See Table 4 for a cross-tabulation summary of each leadership style.
Discussion
In this study, all participants promoted interprofessional health care with positive patient outcomes. There were number of interdisciplinary personnel who crossed boundaries from one function to another. For example, the CEO's roles and responsibilities were made up of interdisciplinary professional tasks and responsibilities. Interdisciplinary work is challenging as it requires numbers of people collaborating to provide high-quality treatment. These participants were vital connections between the hospital's other functions such as operations, medical, nursing and finance. Also, C-level Executives collaborated and worked with each other and ensured their functions operated in a multidisciplinary fashion to provide best quality care. C-level Executives were interviewed from the various magnet and non-magnet hospitals. Given the limited sample size, it can be noticed that the majority (eighty-three percent) of the C-level Executives in the healthcare organization were Caucasian females who held a doctorate level degree. Blackman [5] stated: "Within 31 leadership positions in the organization, women were in the majority at 58.1%, and men were in the minority at 41.9%." This research's demographical findings negate Blackman [5] conclusions at least in the Tri-state region. Furthermore, Mose (2021) stated: "Women executives generally were underrepresented in all positions except in chief human resources and chief nursing officer positions, 73% (95% confidence interval [CI] 7175) and 91% (95% CI 8694), respectively……Women were underrepresented in hospital top positions and were less likely to hold executive positions in large systems or hospitals. (Pg. 124). To add to Mose's (2021) findings, our results suggest that female representation in executives' positions were as follows: Eighty-three (n = 10) percent CNOs, twenty-two (n = 5) percent COOs, and seventeen (n = 4) percent other executives. The findings highlighted that majority (n = 14) of the participants believed that they practiced transformational leadership style; however, most (n = 9) of these C-level Executives practiced the servant and situational (n = 8) leadership styles.
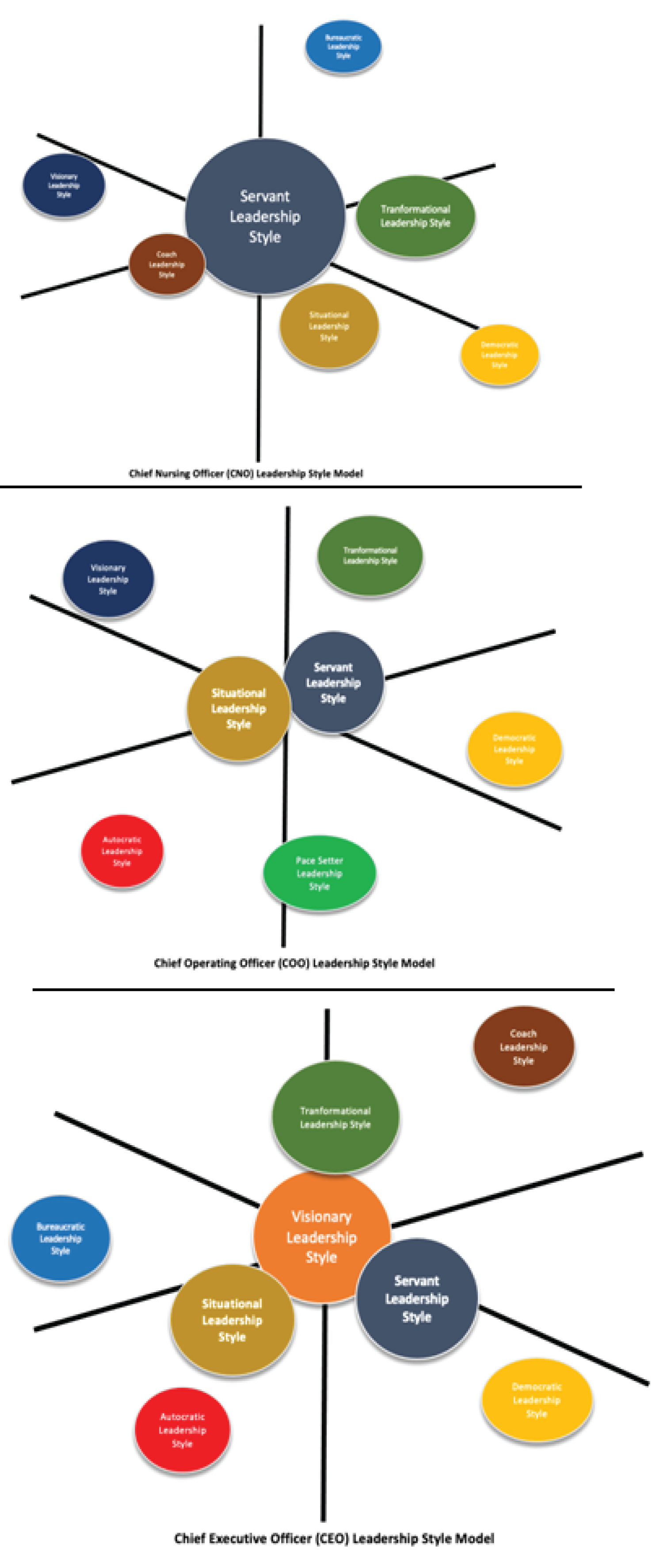
Based on the discussions with participants, it can be concluded that the majority of the C-level Executives found the servant leadership style to be the foundation for any healthcare organization. Based on the roles and responsibilities of the participants, they opted to select alternate leadership styles and build on their predominant leadership style. Figure 1 depicts the leadership styles that the participants practiced according to the organization's titles. It is critical to note that the style at the origin was predominantly practiced by the subject. This research demonstrated that there is a correlation among all those hospitals whose leaders practiced servant leadership styles. The most beneficial leadership styles were a servant and situational when it comes to overall ratings, safety, and financials. Sixty-five (n = 15) percent of hospitals were profitable according to their yearly financial statements. It is vital to note that all those participants who practiced servant leadership style (n = 9) had reported profitability in their yearly financial audit statement. Limitations that may have contributed to the results of this research include the sample size as well as the geographical location [6-15].
Conclusion
In conclusion, the results demonstrated that predominantly servant (thirty-nine percent, n = 9) and situational (thirty-five percent, n = 8) leadership styles were being practiced among the hospital's C-level Executives in the Tri-state region. Also, the hospital's executives and/or leaders who practiced servant leadership style had reported the highest overall ratings and safety grade ratings. Furthermore, when exploring the financials, it showed that all hospital executives who practiced servant leadership style had reported positive financial numbers. The findings of the study support previous research as well as expands the knowledge as it relates to the leadership style. Future research can explore additional executives to this existing body of work as well as geographical considerations.
Acknowledgment
We want to sincerely thank all CEOs, CNOs, and COOs who took part in this study. Their input and contributions to this research are greatly appreciated. We thank Dr. Dana Kemery, Dr. Travis Pollen, Dr. Frances Cornelius, and Professor Virginia Wilson for the face validation phase of the research. We thank Dr. Janet Dawson, Dr. Robert Mele, Shaughan Kennedy, and Christian Keener for their support during the pilot run of this research and giving additional insights from a corporate perspective. We also like to thank Waqas Malak for providing constructive feedback on the manuscript.
Conflicts
None to declare.
References
- Al-Khaled Akram Abdulraqeb Sultan, Chung Jee Fenn (2020) The impact of leadership styles on organizational performance. Journal of Services & Management 13: 55-62.
- Cruz V (2016) Leadership’s role enabling quality culture.
- Cherry K (2019) Why do some people become great leaders?
- Braun V, Clarke V (2006) Using thematic analysis in psychology. Qualitative Research in Psychology 3: 77-101.
- Blackman M (2021) Study finds women only make up 15% of health system CEOS. HealthLeaders Media.
- Aij KH, Rapsaniotis S (2017) Leadership requirements for Lean versus servant leadership in health care: A systematic review of the literature. Journal of healthcare leadership 9: 1-14.
- Anna Montgomery (2018) Servant Leadership Style: 7 Lessons for Developing Leaders.
- Buch K, Rivers D (2001) TQM: The role of leadership and culture. Leadership and Organization Development Journal 22: 365-371.
- Carmeli A (2003) The relationship between emotional intelligence and work attitudes, behavior and outcomes: an examination among senior managers. Journal of Managerial Psychology 18: 788-813.
- Dittrich L (2019) Servant Leadership in Healthcare: A Natural Fit.
- Kellish A (2014) Leadership styles of clinical coordinators and clinical instructors in physical therapy clinical education.
- Sun PY (2013) The servant identity: Influences on the cognition and behavior of servant leaders. Leadership Quarterly 24: 544-557.
- Peláez Zuberbuhler MJ, Salanova M, Martínez IM (2020) Coaching-based leadership intervention program: A controlled trial study. Frontiers in psychology10: 3066.
- Trinkoff AM, Johantgen M, Storr CL, et al. (2010) A comparison of working conditions among nurses in Magnet and non-Magnet Hospitals. The Journal of Nursing Administration40: 309-315.
- Trastek VF, Hamilton NW, Niles EE (2014) Leadership models in health care – a case for servant leadership. Mayo Clinic Proceedings89: 374-381.
Corresponding Author
Haroon M Malak, DHSc, MBA, MSc,Administrator and Scientific Researcher, Department of Health Science, Drexel University, Philadelphia, Pennsylvania, 19102,USA
Copyright
© 2022 Malak HM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.