Optimizing Support and Hope: The Process of Self-Care among Women with HIV/AIDS
Abstract
We aimed to identify the level of self-care and its related factors in women with HIV/AIDS. In this qualitative study, 30 women with HIV/AIDS attending behavioral diseases counseling centers in Tehran, Iran, were invited to participate. Semi-structured interview was the method of data collection. Sampling began purposefully and gradually continued through theoretical sampling based on codes and categories until data saturation was reached. Data analysis was done using the basis of continuous comparative analysis of Strauss & Corbin.
Data analysis resulted in the emergence of three main themes, including empowering oneself and others, healthy lifestyle and informed care. "Self-care in the context of support and hope" was identified as the core theme in this research. Self-care process is affected by underlying factors such as social and economic support and can result in a range of informed care and lack of care. Findings of this study indicated that, the process of self-care in women with HIV/AIDS depends on underlying factors and can vary based on hope and support.
Keywords
HIV/AIDS, Hope, Reproductive age, Self-care, Women
Introduction
During March-September 2015, men and women constituted 66% and 34%, respectively, of HIV-positive cases reported in Iran, half of which (52%) aged 21-35 years-old [1]. Overall, women comprise about 50% of the individuals infected by HIV throughout the world [2] and young women constitute 20% of all new cases of HIV infection recorded throughout the world in 2015. More than half (56%) of these cases were adult women [3]. The main routes of HIV transmission have been shown to be unprotected sex (41%), intravenous drug abuse (39%) and mother-to-child transmission (3%). The route of transmission is, however, unknown in 17% of the cases [1].
HIV positive women in Iran generally lack good health, belong to low socioeconomic status groups, and suffer from severe depression [4]. Also, due to their inadequate education, young HIV-positive women usually fail to receive the required healthcare and social support [5]. Therefore, they commonly have to deal with pregnancy, its related complications and the fear of losing their fetus/baby as well as giving birth to an ill baby, or mother-to-child transmission of HIV through breastfeeding [6].
Self-care behaviors mainly aim at preventing complications [7] and they are defined differently within different cultural and social contexts [8]. During the process of self-care, the person knowingly learns and adopts recognizing and regulating behaviors within his/her stages of growth, development, health, and environment [9]. Self-care is regarded as an effective method to decrease healthcare costs, promote the relationships between participants and the healthcare team, enhance treatment compliance, and decrease the number of hospitalizations and emergency consultations [8].
The initiation and continuation of self-care behaviors can increase participants' motivation towards achieving the desired clinical outcomes. Therefore, such behaviors are essential for the recovery of people with HIV. The care is most effective when the healthcare team develops a deep understanding of the patients' conditions and designs the care plan accordingly [10].
Several studies have been conducted to investigate factors affecting self-care in women with HIV. A recent study on the facilitating and barrier factors to linkage and retention in chronic disease care in western Kenya has shown that only 16% of HIV-positive patients' who were recently diagnosed with the virus had received counseling and appropriate care during last three years [11]. Similarly, results of an observational cohort study revealed that 65-70% of HIV-positive patients' adhered to self-care that was facilitated by support groups and pill counts [12]. These reports are in accordance with findings of other research showing that support groups [13], professional services and work-related support [14] are facilitating factors of self-care in patients' with HIV.
Despite these reports, self-care has been under-studied, especially among women with HIV in Iran. Considering the crucial impact of HIV on women's lives, we conducted a qualitative study to explore self-care among women with HIV in Iran and aimed to optimize support and hope by identifying the level of self-care and its related factors in these women.
Methods
Setting and participants
The participants were selected from behavioral diseases counseling centers in Tehran, Iran. We recruited 30 women with HIV/AIDS. Flyers containing research objectives and information on the provision of free healthcare (including medications, physician visits, and tests) were posted in the notice boards of selected university-affiliated behavioral diseases counseling centers in Tehran.
The following inclusion criteria were applied: (i) A confirmed diagnosis of HIV infection; (ii) Aged 18-48 years-old; (iii) Ability to independently make decisions and perform self-care activities; (iv) Willingness to participate in the study; (v) Speaking Farsi language. We used maximum variation sampling to assess the effects of various factors (e.g. employment and marital status, time of diagnosis, and route of transmission) on women's experiences.
Ethics
The study protocol was approved by the Human Research Ethics Committee at the …. before its commencement.
Data collection
Eligible women were approached in the study clinic and were briefed about study objectives. Those who were interested in participating received the participant information sheet and signed the consent form. Semi-structured in-depth interviews were conducted and field notes were used to collect data. An interview template was designed for data collection (Table 1). More probing questions, e.g. "Please elaborate on that" or "What do you mean by that?" were then raised. Two of the participants were interviewed twice to validate the findings of the first interviews and refine the concepts and categories.
All interviews were conducted in a private room in the counseling centers by the same researcher. Each interview lasted for 35-65 minutes (50 minutes on average). All interviews were audio-recorded in MP3 format upon the participants' approval and were transcribed word by word by the researcher. Data collection was performed over a 12-month period and continued until data saturation occurred.
Qualitative analysis
Strauss and Corbin's approach [15] was adopted for data analysis. Each interview was transcribed verbatim and analyzed immediately after its completion. Open, axial, and selective coding was used for simultaneous data collection and analysis [15]. Grounded theory uses open coding, i.e. line by line coding of the text, to break the text into its main elements. Constant comparisons were also applied during the analysis, to detect any relations between the identified elements. Axial coding was also performed concurrently with data collection to identify the main themes. A number of techniques, e.g. constant comparative analysis, theoretical memo writing, and theoretical sampling, were used during the process of data analysis to determine the existing categories [16]. Any questions or new ideas arisen during the open coding stage were recorded as memos and used for selecting the next participant, revising the interview questions, and analyzing the data. Following the emergence of the initial categories, the data suggested the need for collecting more information about caregivers, e.g. the patient's husband, mother, and sister.
Findings
A total of 30 women with HIV/AIDS were interviewed with the mean age of 35.5 ± 6.3 years (ranged 20-46 years). Demographic characteristics of the participants are shown in Table 2. Out of 30 participants, four had presented symptoms of AIDS infection and were frequently admitted to the hospital for eye Cytomegalovirus retinitis, blindness, Type II Herpes simplex virus and/or renal disease.
The core category in the process of self-care in women with HIV/AIDS was shown to be 'self-care in the context of support and hope'. Three main theses and 11 sub-themes were identified (Table 3).
Theme 1: Empowering oneself and others
Empowering oneself and others was one of the main categories that emerged in the process of self-care. A while after the diagnosis of the disease was confirmed, the participants focused on empowering themselves. They also attempted to obtain information and transfer it to others by using learning and teaching strategies, such as understanding the disease, its complications and its treatment.
Sub theme 1.1: Awareness: Participant's statement indicated both sufficient and insufficient awareness about self-care. Sometimes information was not given to women especially women who did not attend the positive club. For example one woman said:
"… I have a lot of trouble since we've become HIV positive. You feel that question mark on your head and want to leave the community until you become aware and recognize the illness" (P 15, 42-years-old).
Subtheme 1.2: Learning about HIV: After consultation with psychologist and the doctor, the women began to learn about HIV/AIDS and tried to attend the classes at the positive club and learn about self-care. One woman explained:
"I came here and my mindset changed, I noticed that this disease is not a monster as people outside say" (P 15, 42-years-old).
Subtheme 1.3: Searching for information: One of the strategies taken by the participants was to obtain more information on HIV/AIDS. Availability of behavioral diseases counseling centers which provided them with essential information and training about self-care. Those who were more educated tried to obtain information about the disease themselves. They read books, newspapers and magazines. For instance, one woman declared:
"Well, I searched through internet looking for new medications, and I got a lot of new things" (P 2, 38-years-old).
Subtheme 1.4: Information transfer: HIV-positive women thought they had a duty to inform others about HIV/AIDS as they themselves had become infected with this virus due to the lack of awareness about the disease. They informed friends and neighbors and had interviews with the media. One woman mentioned:
"… I myself was the victim of the lack of information. If I knew about it, I wouldn't have become infected. I work with the center's doctor to inform others. I have talked with the Member of Parliament. I have attended various courses and have worked in the drop-in centre as a counselor giving advice on HIV/AIDS. I also volunteer to speak about it easily, if any opportunity arises" (P 20, 44-years-old).
Theme 2: Healthy lifestyle
This category consisted of two subcategories, including "responsibility for care", "changing behaviors".
Subtheme 2.1: Responsibility for care: The level of individual's responsibility towards oneself and others is different. Although, responsibility for caring is not limited to a specific period of life and individuals feel responsible for themselves and others for their entire lifetime, its role and necessity in chronic illness such as HIV/AIDS is undeniable. For example, one woman said:
"… I used to hide my disease when going to doctors in the past, but now I tell the truth and get the right medication that helps me got well quickly" (P 21, 37-years-old).
Subtheme 2.2: Changing behaviors: Following a changing lifestyle in the self-care process, these women viewed HIV/AIDS as an opportunity to change their behavior, planned to abandon their previous risky behaviors and replace them with healthy appropriate behaviors. One woman mentioned:
"I take more care unconsciously when choosing the people, I associate with. I say to myself, I do not have hepatitis, so I should be careful not to add it to my disease" (P 20, 44-years-old).
Theme 3: Informed care
Informed care was one of the important components of the self-care process, which was characterized by four sub-themes, including 'spiritual' 'psychological', 'socio-emotional', 'physical' and 'sexual behavior' reconstruction.
Subtheme 3.1: Spiritual reconstruction: Women with HIV/AIDS, despite dilemmas they had within the community, referred to "communication with God" as a source of support. They repeatedly referred to "trust in God", "life in the hands of God" or "divine test" in their statements. For example, one woman said:
"I have left everything in God's hand. I said: God, bring me whatever that is right for me" (P 20, 44-years-old).
Subtheme 3.2: Psychological reconstruction: The spiritual reconstruction was a basis for improved mental health and a calmer personality. They accepted their illness and fought for their life to stay alive through psychological reconstruction. One woman mentioned:
"… following my suicide, I had 15 sessions of psychotherapy. This year, my life has become very good, especially since 3 months ago. Suddenly I was faced with this illness. It was very difficult at first" (P 24, 28-years-old).
Subtheme 3.3: Socio-emotional reconstruction: Having healthy interpersonal relationships with family, friends and peers was one of the important factors in the socio-emotional reconstruction of these participants. Many of them stated that they have learned most of their information about the disease from their peers. For example, one woman mentioned:
"... I like this community [the counseling center]. They are my family. Saturdays we share breakfast …. It is a very good time" (P 22, 36-years-old).
Subtheme 3.4: Physical reconstruction: Participants did not undermine HIV, and the footprint of fight for life and survival could be seen in them. Their passion for learning and gathering information about HIV/AIDS had provided a condition for them to continue trying for survival. In physical reconstruction, the participants paid attention to their nutrition, trying to consume vegetables and fruits as much as possible depending on their economic status. They attended the Behavioral Counseling Center for follow-up treatment and vaccine injection, had enough sleep and regularly took their medications. The fear of opportunistic infections and their love of life was the most important reason for self-care in these participants. For instance, one woman declared:
"Nutrition is important for me ... I try to have a good diet and take my medication regularly without interruption. I did yoga for a month ... I used to play volleyball and swim… I walk for about half an hour every day" (P 17, 28-years-old).
Subtheme 3.5: Sexual behavior reconstruction: Taking responsibility in sexual relationships played an important role in preventing the transmission of HIV/AIDS, or if the spouse was HIV positive. For example, one woman said:
"… You should use a condom when having sex with anyone. It may affect your virus, and situation may get worse... I shouldn't let the condition to get worse until I the virus in my body becomes zero" (P24, 28-years-old).
Self-care model: The linkage between self-care themes and self-care process
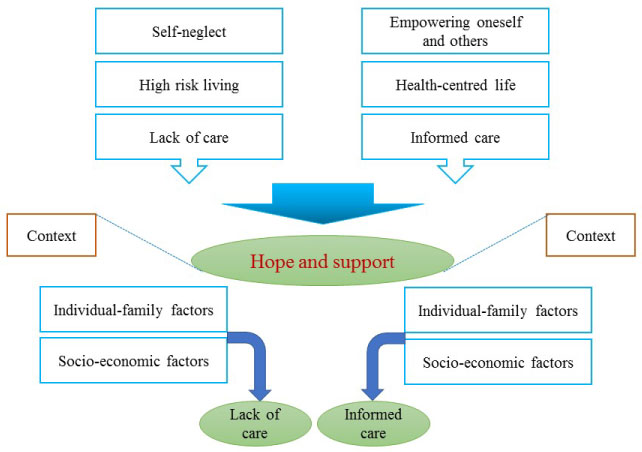
With regards to the themes and sub-themes, six elements were discovered in our study which were linked to one another through the concept of hope and support as shown in the process of self-care, Figure 1. The route from 'hope and support' to 'lack of care' or 'informed care' was modulated by the individual-family factors and socio-economic factors.
As shown in Figure 2, the women's response to the HIV/AIDS included the focus on empowerment oneself and others, healthy lifestyle and informed care, which formed three levels of self-care process in the women, including informed care, irregular care and lack of care. These levels of care had a dynamic nature indicating that women might have been moving, side to side, among these levels of care. It was shown that when the supportive bedrock was available and the patients had the hope for survival, they had a sense of responsibility and as a result, they performed better self-care behaviors and saw better results. These women had a tendency to move forward and have informed self-care, but they needed a favorable ground. However, when the conditions were not favorable, the women had inferior self-care behaviors.
The nature of HIV/AIDS and need for drug use, negative and varying viewpoints of people, being at the advanced stage of the disease, unfamiliarity with the term 'AIDS', and lack of adequate education within the community significantly affected the self-care of women with HIV/AIDS. Problems caused by the disease created limitations in occupation and income, causing financial problems and irregular or lack of self-care. Inadequate awareness of community about AIDS, hopelessness and depression, fear of disease progress, and inadequate support for HIV-positive women significantly affected self-care in these women, pointing to a dark and awful future. This fear of disease progress highlighted itself so much that it was recognized as a major socio-psychosocial problem among these women. However, in some women, the fear of disease progress had provided a basis for a more active self-care, while in others the ability to take care of themselves was undermined by the weakening of morale and hope.
Discussion
In this study, three main themes and 11 sub-themes were emerged, which were correlated with the concepts of support and hope as the main socio-psychosocial processes. Physical disabilities and psychological distress were two major concerns for women with HIV/AIDS, caused by anxiety, depression, and negative attitudes. Some women had lost their hope and felt disappointed, saying they did not know what will be the fate of themselves and their children. The usual questions in these women included "what would happen at the end?" "Will I be treated?" "Will definitive treatment be discovered for this disease?" These feelings varied from person to person, so that, in women who had the support of family and friends, such psychological distress was less. In dealing with these problems, women behaved differently, some of them said that cancer is better than HIV/AIDS because it will kill the patient more quickly, but in some women, the hope for survival had made them to have a different understanding of HIV/AIDS and work hard to survive. These findings are in accordance with the reports of Eller, et al. [17] study in which depression symptoms in HIV positive people was associated with negative emotions (sadness, fear, anxiety, and suicidal thoughts), physical symptoms (fatigue), and interpersonal problems (loneliness and isolation) and reduced motivation [17]. Other studies have shown that the rate of depression and anxiety in HIV-positive women is higher than HIV- positive men [2,17].
One of the most important sources in coping with the HIV/AIDS problem, affecting the outcome of self-care was the perceived support from family/friends, healthcare team, and health system. Results of Harralson's [18] study showed that the more support women received from friends, family and colleagues, the more they tended to seek treatment [18]. Having support also boosted the life expectancy of the women. Financial support from the health system helped them to maintain their calmness and hope and also attend scheduled visits to doctor. These women did their best to carry out self-care behaviors, including "spiritual reconstruction" "psychological reconstruction", "socio-emotional reconstruction", "physical reconstruction", and "sexual behavior reconstruction". For those women who had irregular self-care, their self-care behaviors were heavily influenced by the support from the family, especially the spouse, making them to adhere to self-care behaviors in a desirable manner. In contrast, family concerns and tensions, such as failure to remarry, arguments and conflicts with the spouse, addiction and divorce of parents interfered with the process of self-care and disturbed their peace.
Some of these women preferred to see their doctor only whenever they had a symptom or physical problem, and used drug irregularly only to relieve the symptoms. For these women, factors such as the follow-ups of counseling staff, the fear of opportunistic infections, and deterioration of the disease were acting as incentive to self-care behaviors temporarily. Contrary to them, there were women who not only did not take any preventative action, but also did not pay attention to the spiritual, psychological, social and sexual aspects of self-care. This group was considered as a risk to the community as they neglected their illness. Previous research [19] has reported that the risk of neglecting or undermining the illness is greater in people who have not experienced the effects of illness, can control the effects of disease by irregular use of drugs or have other goals such as maintaining a job over their illness. The consequences of the lack of self-care included opportunistic infections, increased viral load and transmitting it to others and eventually, presenting symptoms of AIDS.
Self-care is a part of a broader concept known as self-management. Self-management of a chronic disease, such as HIV-AIDS, is defined as engaging in health promoting activities or being responsible for routine daily management of the disease [20]. Nevertheless, studies on the self-management education programs and the group visits program have shown that the patients' favorable outcomes are highly correlated with the patients' perceived self-efficacy to cope with the consequences of their chronic diseases and not strongly related with the incorporated activities and programs [21]. These reports imply that the central outcome of the learning experience is enhancing patients' confidence that can help them cope with the consequences of the disease and more effectively manage their course of illness.
Implications for practice and/or policy
Previous research [22] has reported three programmes that can enhance the patients' participation in their healthcare. The first is self-management and self-care education that provides information on the medication use, behavior changes, social and workplace adjustments, coping with emotional reactions, interpretation of variations in the disease and its consequences, and the use of medical and community resources [23,24]. The second approach is group visits offering recurrent meetings between groups of patients and their healthcare provider. This approach has been shown to enhance their quality of life, increase their life satisfaction, and decrease the use of medical services, while the patients are responsible for their own care [25]. The third medical management approach is remotely through the telephone or electronic communication, which has been shown to decrease cost and improve the health status of patients and can benefit those who may not normally attend a healthcare facility [26].
The development of self-care plans and programs appear to be the key to avoid helplessness and powerlessness inherent in women with HIV/AIDS. Empowering techniques, such as learning about their disease and how to stop spreading the virus while looking after own health, can help promote self-care among women living with HIV. Our findings indicate that all of these techniques can be more effective when learned in the context of a caring relationship with the clinicians.
Self-care can also help achieve the institutional health goals in resource-scarce and fragile settings. The improved cooperation between communities, healthcare providers and health ministries, multi-pillar self-care interventions can be projected to meet people's needs through widespread and cohesive health services.
Limitations and strengths
Our study has several limitations and strengths. One of the limitations of the study is lack of generalizability of the findings as they were extracted from a qualitative research designs. Another limitation of this study is selecting the participants from HIV clinics which eliminated the chance to explore the perceptions of women who did not participate in their communities. Despite these shortcomings, our study has several strengths including detailed description of the context, maximum variation and theoretical sampling. Also, the use of in-depth interviews provided researchers with the opportunity to understand the women's feelings and perspectives of self-care.
Conclusions
The theory and model of 'self-care in the context of hope and support' showed that self-care process in women of reproductive age with HIV/AIDS occurred in a complex setting consisting of various cultural, socio-economic and psychological factors. In addition, the women's response to the HIV/AIDS included the focus on empowerment oneself and others, healthy lifestyle and informed care, which formed different levels of self-care process in the women, including informed care, irregular care and lack of care.
Acknowledgements
This study is a part of the Ph.D. dissertation supported by Iran University of Medical Sciences. We would like to thank the Health Deputy of Iran, Tehran and Shahid Beheshti Universities of Medical Sciences for their cooperation and financial support. We also express our gratitude to all the participating women for sharing their valuable experiences.
Conflict of Interest
The authors declare no conflict of interest.
References
- Ministry of Health and Medical Education, C. f. t. m. o. i. d. (2015) Registered cases of HIV infection reported in Iran.
- Padyana M, Bhat RV, Dinesha AN (2013) HIV in females: A clinico-epidemiological study. J Fam Med Prim Care 2: 149-152.
- UNAIDS, P. o. H. A. (2016) Global AIDS Response Progress Reporting (GARPR).
- Dolan K, Salimi S, Nassirimanesh B, et al. (2011) Characteristics of Iranian women seeking drug treatment. J Womens Health (Larchmt) 20: 1687-1691.
- Plach SK, Stevens PE, Heidrich SM (2006) Social roles and health in women living with HIV/AIDS: A pilot study. J Assoc Nurses AIDS Care 17: 58-64.
- Olagbuji BN, Ezeanochie MC, Ande AB, et al. (2010) Obstetric and perinatal outcome in HIV positive women receiving HAART in urban Nigeria. Arch Gynecol Obstet 281: 991-994.
- Coyle MK, Martin EM (2007) Reflecting on a self‐care process in the home setting for traumatic brain injury survivors. J Neurosci Nurs 39: 274-277.
- Baquedano IR, Dos Santos MA, Martins TA, et al. (2010) Self-care of patients with diabetes mellitus cared for at an emergency service in Mexico. Rev Lat Am Enfermagem 18: 1195-1202.
- Orem D (2001) Nursing concepts of practice. Mosby, Inc Google Scholar, St Louis, USA.
- Perrett SE, Biley FC (2013) Negotiating uncertainty: The transitional process of adapting to life with HIV. J Assoc Nurses AIDS Care 24: 207-218.
- Rachlis B, Naanyu V, Wachira J, et al. (2016) Identifying common barriers and facilitators to linkage and retention in chronic disease care in western Kenya. BMC Public Health 16: 741.
- Achieng L, Musangi H, Ong'uti S, et al. (2012) An observational cohort comparison of facilitators of retention in care and adherence to anti-eetroviral therapy at an HIV treatment center in Kenya. PLoS One 7: e32727.
- Kuchinad KE, Hutton HE, Monroe AK, et al. (2016) A qualitative study of barriers to and facilitators of optimal engagement in care among PLWH and substance use/misuse. BMC Res Notes 9: 229.
- Barkey V, Watanabe E, Solomon P, et al. (2009) Barriers and facilitators to participation in work among Canadian women living with HIV/AIDS. Can J Occup Ther 76: 269-275.
- Strauss A, Corbin J (1998) Basics of qualitative research techniques. Sage Publications.
- Holloway I (2005) Qualitative research in health care. McGraw-Hill Education, UK.
- Eller LS, Corless I, Bunch EH, et al. (2005) Self‐care strategies for depressive symptoms in people with HIV disease. J Adv Nurs 51: 119-130.
- Harralson TL (2007) Factors influencing delay in seeking treatment for acute ischemic symptoms among lower income, urban women. Heart Lung 36: 96-104.
- Charmaz K (2014) Constructing grounded theory. Sage Publishing.
- Lorig KR, Holman H (2003) Self-management education: History, definition, outcomes, and mechanisms. Ann Behav Med 26: 1-7.
- Holman H, Lorig K (2004) Patient self-management: A key to effectiveness and efficiency in care of chronic disease. Public Health Rep 119: 239-243.
- Holman H, Lorig K (2000) Patients as partners in managing chronic disease. Partnership is a prerequisite for effective and efficient health care. BMJ 320: 526-527.
- Lorig K, Mazonson PD, Holman HR (1993) Evidence suggesting that health education for self‐management in patients with chronic arthritis has sustained health benefits while reducing health care costs. Arthritis Rheum 36: 439-446.
- Lorig KR, Sobel DS, Stewart AL, et al. (1999) Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Med Care 37: 5-14.
- Beck A, Scott J, Williams P, et al. (1997) A randomized trial of group outpatient visits for chronically ill older HMO members: The Cooperative Health Care Clinic. J Am Geriatr Soc 45: 543-549.
- Simon GE, VonKorff M, Rutter C, et al. (2000) Randomised trial of monitoring, feedback, and management of care by telephone to improve treatment of depression in primary care. BMJ 320: 550-554.
Corresponding Author
Farzaneh Kashefi, Nursing Care Research Center, Iran University of Medical Sciences, Tehran, Iran, ORCID iD: 0000-0003-2306-267X.
Copyright
© 2019 Kashefi F, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.