Current Status of Grafts Materials Used in Rhinoplasty. Literature Review
Abstract
Background: The overall aesthetics of the face are significantly affected by the appearance of the nose. Among the nasal defects, the saddle type of nose is often found. Various grafting materials are widely used in rhinoplasty. However, the choice of the optimal material in different clinical situations remains a matter of debate.
Purpose: The purpose of this review was to evaluate effects various grafting materials used in rhinoplasty advantages and disadvantages of each.
Methods: The review included articles from Google Scholar, Medline, Scopus, Web of Sciences, PubMed, Cochrane Library websites were searched. Saddle type of nose, rhinoplasty autograft, (septal cartilage, auricular cartilage, costal cartilage), allograft, PRP, fluid cartilage, rhinofiller and alloplastic implants, were used as search keywords; the effectiveness of the use of each material, resorption results, complications, functional and aesthetic satisfaction of patients were evaluated. Review was conducted according to the PRISMA guidelines.
Results: Out of 127 articles in the literature search, 71 articles that met the inclusion criteria were included in this article. Autograft is very applicable in dorsal rhinoplasty, but autograft surgery of autograft cartilage is not acceptable for all patients in all cases, due to various complications that may occur at the donor site, such as pain, pneumothorax, and scarring. An alternative is allograft (irradiated and non-irradiated rib) which excludes the above-mentioned complications, but has a higher resorption rate; Currently used alloplastic materials also have drawbacks and scientific research in the optimal direction is ongoing.
Conclusions: With this comprehensive review, the authors hope to highlight the advantages and disadvantages of the different materials currently used in aesthetic rhinoplasty, which may enable the surgeon to achieve optimal aesthetic and functional results. Further research is needed to establish clear guidelines for selecting the appropriate material for rhinoplasty.
Keywords
Saddle type of nose, Grafts materials used in rhinoplasty, Autograft, Allograft, PRF, Fluid cartilage, Rhinofiller, Alloplastic grafts materials
Introduction
One of the most popular plastic surgeries in the maxillofacial area is rhinoplasty, which improves the harmony of the face and the proportions of the nose [1].
The etiology of aesthetic defects of the nose is diverse: congenital, traumatic and iatrogenic (violation of the dorsal L-shaped support after septoplasty), which forces the patient to resort to the method of rhinoplasty [2-4].
Among the nasal defects, the saddle type of nose is often found, which is associated with the loss of the dorsal part of the quadrangular cartilage of the nose [5,6].
Defects in the profile of the nasal dorsum are classified into major and minor defects. There are two different types of rhinoplasty procedures: Open and Closed Rhinoplasty [7]. Depending on the nasal corrections needed to be made, surgeons determine the type of rhinoplasty needed by examining the advantages and risks of both procedures.
In an open rhinoplasty, an incision will be made beneath the tip of the nose where the columella is. A closed rhinoplasty is also known as an endonasal rhinoplasty. In an endonasal rhinoplasty, surgical incisions are made inside the patient’s nose.
Different graft materials are used in plastic surgery of the nose, mainly 3 types of grafts are used; [8-23]
autogenous,
homograft,
synthetic.
The purpose of this review was to evaluate effects various grafting materials used in rhinoplasty advantages and disadvantages of each.
Methods
The review included articles from Google Scholar, Medline, Scopus, Web of Sciences, PubMed, Cochrane Library websites were searched.
Autograft, (septal cartilage, auricular cartilage, costal cartilage), allograft, PRP, fluid cartilage, rhinofiller and alloplastic graft materials, were used as search keywords; the effectiveness of the use of each material, resorption results, complications, functional and aesthetic satisfaction of patients were evaluated. Two review authors screened the results of the searches against inclusion criteria and in duplicate. First, articles obtained from the database search were identified; then, articles were selected, excluding duplicates and those not relevant to certain descriptors, by screening titles and abstracts; after this step, an eligibility check was performed with full text reading, excluding articles that did not meet the previously established criteria; finally, relevant articles were included in the systematic review.
Results
From the 127 articles considered in the analysis, 71 articles that met the inclusion criteria were included. Review was conducted according to the PRISMA guidelines (Table 1).
Sources of autogenous grafts remain the gold standard in rhinoplasty of the dorsum of the nose, as they provide sufficient quantity and quality of grafts.
Small defects can be repaired using septum or auricular cartilage [24,25]. Large deformities of the dorsum the preferred graft is costal cartilage [26,27].
Usually, autogenous cartilage is harvested from either the septum, auricle, or rib and each of them is used in different clinical situations based on its specific properties (Figure 1).
Autogenous septal cartilage is the preferred graft material for rhinoplasty because its ability to provide a single surgical field, its stability, and its resistance to infection, with minimal deformation and resorption [24, 28-30]. Autologous septal cartilage grafts integrate well with the surrounding tissues, and their elasticity provides good support, but these surgical methods are undesirable for patients due to donor site morbidity (Figure 2, Figure 3 and Figure 4).
Conchal cartilage is also often used for nasal grafts. It has a characteristic curve and is softer and more flexible than septal cartilage, conchal cartilage is ideal for nasal tip grafts [31,32]. Conchal cartilage advantages include low morbidity, and resistance to resorption (Figure 5 and Figure 6).
The use of costal cartilage is dictated by a number of features of its structure, which have a number of obvious advantages [33].
- Sufficient thickness- upto 5-7 cm;
- Strength;
- The ability to create almost any given configuration;
- Stability of the resulting structure
However, the difficulties associated with obtaining costal cartilage such as various complications: prolonged pain, pneumothorax, scarring, second surgical site make many patients reluctant to resort to this method [15,34] (Figure 7, Figure 8 and Figure 9).
One of the methods of non-surgical rhinoplasty is the use of autologous fat as filler [35]. Currently, nasal lipofilling using autologous fat is one of the minimally invasive methods for correcting the aesthetics and contour of the nose; this method is effective, is relatively low- morbidity and has a low incidence of complications [36].
Recently, PRF has also been used in rhinoplasty, which contains factors such as platelet-derived growth factor, vascular endothelial growth factor [37,38].
In dorsal rhinoplasty, crushed septal cartilage and PRF have also been used occasionally when indicated [20,39] (Figure 10 and Figure 11).
For large dorsal defects, rib allograft lyophilized Freeze-Dried Allograft Bone used; it has high osteo conductivity, is strong enough to provide structural support, and overcome soft tissue resistance [40-42] (Figure 12).
However, allograft also has disadvantages such as inflammatory reactions, infection, and resorption. During preparation, the cartilage is irradiated with 30,000-50,000 Gy. It is believed that with increasing radiation intensity, collagen damage increases and resorption increases accordingly [17,43-45].
Small dorsal defects can be repaired by AlloDerm, it is a lyophilized sheet of human dermis collagen matrix and allows the ingrowth of host tissue is a good alternative to autogenous dorsal rhinoplasty [46]. Partial AlloDerm resorption, is a definite disadvantage (Figure 13).
Hyaluronic acid (HA) is also used for rhinoplasty due to its effectiveness and short recovery time, but HA filler injections are not without complications. HA filler injections can cause some complications: skin necrosis; hypersensitivity; vascular disorders, etc. [47-52].
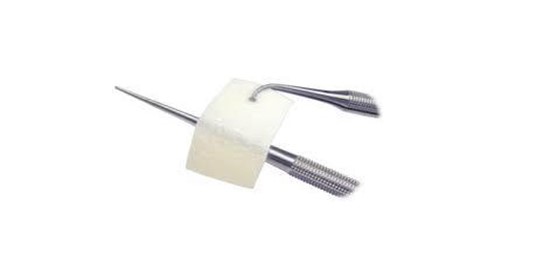
In aesthetic rhinoplasty for minor contour deformations of the nasal surface, liquid cartilage is also used and its use is a microinvasive procedure [53].
Liquid cartilage grafts are more flexible for filling lesions, they are prepared from septal, lateral or less commonly conchal cartilage and are inserted through a needle from the surface of the skin or mucosa shell into the defect area without any incision or raising a skin flap [54]. Its disadvantage is poor mechanical stability and rapid decomposition, leading to wrinkling and deformation (Figure 14).
Alloplastic materials can be used successfully for dorsal augmentation. The most commonly used alloplastic materials include silicone, expanded polytetrafluoroethylene (Gore-Tex; W. L. Gore and Associates, Flagstaff, Ariz.), or porous high-density polyethylene (Medpor; Porex Medical, Fairburn, Ga) as they are readily available to avoid complications associated with the donor site [55,56]. Silicone implants should not be used for the tip of the nose as it fails to build up the underlying structure, thereby causing an unnatural result and possible side effects. Problems associated with alloplastic materials in rhinoplasty described in the literature [57] (Figure 15 and Figure 16).
Each of these materials has unique structural and biocompatibility properties and is therefore used for different procedures and indications. Each of the grafts has advantages and disadvantages, and the choice of the ideal graft material remains a matter of debate.
Discussion
Surgical rhinoplasty techniques are constantly being improved, and work continues on the use of the optimal biocompatible graft [58].
Cartilage allografts are optimal for rhinoplasty [59]. The biochemical composition of septal cartilage includes 90-95% collagen II, and the rest contains collagens I, IX, X, and XI [60-63].
One of the common complications of cartilage grafts is their resorption.
It has a low rate of resorption, extrusion, and deformation [64].
Currently, gamma-irradiated cartilage allografts are also used in rhinoplasty [65,66].
According to published literature, the resorption rate of irradiated homologous lateral cartilage (31%) is significantly higher than that of autologous cartilage (3%), which is due to the lack of viable cells in cartilage allografts [67].
PRF is currently used in rhinoplasty because it provides angiogenesis [37,42].
The presented literature review shows that the selection of the optimal graft in aesthetic rhinoplasty is a topical and urgent issue that requires a thorough long-term study.
Conclusions
With this comprehensive review, the authors hope to highlight the advantages and disadvantages of the different materials currently used in aesthetic rhinoplasty, which may enable the surgeon to achieve optimal aesthetic and functional results. Further research is needed to establish clear guidelines for selecting the appropriate material for rhinoplasty.
Declarations
Competing interest
No competing interest.
Funding:
Not funded.
Ethical approval
Not availability.
Consent for publication
Patients gave written consent for their surgical figures to be included in the article.
Availability of data and materials
Not availability.
References
- Khan N, Rashid M, Khan I, et al. (2019) Satisfaction in patients after rhinoplasty using the rhinoplasty outcome evaluation questionnaire. Cureus 11: e5283.
- Dresner HS, Hilger PA (2008) An overview of nasal dorsal augmentation. Semin Plast Surg 22: 65-73.
- Park SS (2011) Fundamental principles in aesthetic rhinoplasty. Clin Exp Otorhinolaryngol 4: 55-66.
- Hohman MH, Fichman M, Piedra Buena IT (2025) Rhinoplasty. StatPearls Publishing, Treasure Island, FL.
- Daniel RK, Brenner KA (2006) Saddle nose deformity: A new classification and treatment. Facial Plast Surg Clin North Am 14: 301-312.
- Malone M, Pearlman S (2015) Dorsal augmentation in rhinoplasty: A survey and review. Facial Plast Surg 31: 289-294.
- Gupta R, John J, Ranganathan N, et al. (2022) Outcomes of closed versus open rhinoplasty: A systematic review. Arch Plast Surg 49: 569-579.
- Harutyunyan A (2024) Use of grafts materials in dorsal augmentation rhinoplasty. Bulletin of stomatology and maxillofacial surgery 20: 142-151.
- Khan NA, Rehman A, Yadav R (2016) Uses of various grafting techniques in external approach rhinoplasty: An overview. Indian J Otolaryngol Head Neck Surg 68: 322-328.
- Sajjadian A, Rubinstein R, Naghshineh N (2010) Current status of grafts and implants in rhinoplasty: part I. Autologous grafts. Plast Reconstr Surg 125: 40e-49e.
- Kim YK, Kania K, Nguyen AH (2015) Rhinoplasty with cartilage and alloplastic materials, Nasal SMAS management in Asian rhinoplasty, contracture classification, and secondary rhinoplasty with contracture. Semin Plast Surg 29: 255-261.
- Nguyen HL, Hoang MP, Nguyen VM, et al. (2022) Use of septal cartilage in rhinoplasty to correct nasal deformity after unilateral cleft lip and palate surgery. Clin Cosmet Investig Dent 14: 131-140.
- Zhang C, Jin TT, Li JY, et al. (2021) Application of conchal cartilage grafts in nasal tip plasty: Comparison and experience of 3 methods. Ann Plast Surg 86: S199-S207.
- Gunter JP, Cochran CS, Marin VP (2008) Dorsal augmentation with autogenous rib cartilage. Semin Plast Surg 22: 74-89.
- Aboul Wafa AM (2019) Extended L-Framework: An innovative technique for reconstruction of low nasal dorsum by autogenous costal cartilage graft. Plast Reconstr Surg Glob Open 7: e2080.
- Alshehri WM, Aldosari A, Alherz AH, et al. (2020) Augmentation rhinoplasty using iliac crest graft in saddle nose deformity. Cureus 12: e9705.
- Clark RP, Pham PM, Ciminello FS, et al. (2019) Nasal dorsal augmentation with freeze-dried allograft bone: 10-year comprehensive review. Plast Reconstr Surg 143: 49e-61e.
- Vargas G, Biguria R (2018) Cartilage allografts for aesthetic nose surgery: A viable option. Plast Reconstr Surg Glob Open 6: e1859.
- Civinini R, Macera A, Nistri L, et al. (2011) The use of autologous blood-derived growth factors in bone regeneration. Clin Cases Miner Bone Metab 8: 25-31.
- Gode S, Ozturk A, Berber V, et al. (2019) Effect of injectable platelet-rich fibrin on diced cartilage's viability in rhinoplasty. Facial Plast Surg 35: 393-396.
- Kumar V, Jain A, Atre S, et al. (2021) Non-surgical rhinoplasty using hyaluronic acid dermal fillers: A systematic review. J Cosmet Dermatol 20: 2414-2424.
- Saadoun R, Solari MG, Rubin JP (2023) The role of autologous fat grafting in rhinoplasty. Facial Plast Surg 39: 185-189.
- Joo YH, Jang YJ (2016) Comparison of the surgical outcomes of dorsal augmentation using expanded polytetrafluoroethylene or autologous costal cartilage. JAMA Facial Plast Surg 18: 327-332.
- Yoon SH, Kim CS, Oh JW, et al. (2021) Optimal harvest and efficient use of septal cartilage in rhinoplasty. Arch Craniofac Surg 22: 11-16.
- Boccieri A, Marano A (2007) The conchal cartilage graft in nasal reconstruction. J Plast Reconstr Aesthet Surg 60: 188-194.
- Malhotra M, Varshney S, Joshi P, et al. (2018) A Modified technique of rhinoplasty using cortical bone graft to correct saddle nose deformity with loss of septal cartilage. Exp Rhinol Otolaryngol 2: 101-104.
- Gurley JM, Pilgram T, Perlyn CA, et al. (2001) Long-term outcome of autogenous rib graft nasal reconstruction. Plast Reconstr Surg 108: 1895-1905.
- Parrilla C, Artuso A, Gallus R, et al. (2013) The role of septal surgery in cosmetic rhinoplasty. Acta Otorhinolaryngol Ital 33: 146-153.
- Sancho BV, Molina AR (2014) Use of septal cartilage homografts in rhinoplasty. Aesthetic Plastic Surgery 24: 357-363.
- Sancho BV, Molina AR (2000) Use of septal cartilage homografts in rhinoplasty. Aesthetic Plast Surg 24: 357-363.
- Kumar R, Darr A, Gill C, et al. (2022) The use of auricular cartilage grafts in septorhinoplasty: A dual-centre study of donor site patient-reported outcome measures. Cureus 14: e26547.
- Jovanovic S, Berghaus A (1991) Autogenous auricular concha cartilage transplant in corrective rhinoplasty. Practical hints and critical remarks. Rhinology 29: 273-279.
- Al-Qattan MM (2007) Augmentation of the nasal dorsum with autogenous costal cartilage using the "edge on" technique. Ann Plast Surg 59: 642-644.
- Gunter JP, Clark CP, Friedman RM (1997) Internal stabilization of autogenous rib cartilage grafts in rhinoplasty: A barrier to cartilage warping. Plast Reconstr Surg 100: 161-169.
- Kovacevic M, Kosins AM, Göksel A, et al. (2021) Optimization of the soft tissue envelope of the nose in rhinoplasty utilizing fat transfer combined with platelet-rich fibrin. Facial Plast Surg 37: 590-598.
- Keyhan SO, Ramezanzade S, Bohluli B, et al. (2021) Autologous fat injection for augmentation rhinoplasty: A systematic review. Aesthet Surg J Open Forum 3: ojab010.
- Gode S, Ozturk A, Kismali E, et al. (2019) The effect of platelet-rich fibrin on nasal skin thickness in rhinoplasty. Facial Plast Surg 35: 400-403.
- Ozer K, Colak O (2019) Micro-autologous fat transplantation combined with platelet-rich plasmafor facial filling and regeneration: a clinical perspective in the shadow of evidence-based medicine. J Craniofac Surg 30: 672-677.
- Yan D, Li SH, Zhang AL, et al. (2023) A clinical study of platelet-rich fibrin combined with autologous high-density fat transplantation in augmentation rhinoplasty. Ear Nose Throat J 102: 598-604.
- Rohrich RJ, Shanmugakrishnan RR, Mohan R (2020) Rhinoplasty refinements: Revision rhinoplasty using fresh frozen costal cartilage allograft. Plast Reconstr Surg 145: 1050e-1053e.
- Harutyunyan A, Hakobyan G (2024) Saddle nose deformity reconstruction with a allograft bone. Aesthetic Plast Surg 48: 4839-4847.
- Harutyunyan A, Hakobyan G (2024) Dorsal augmentation rhinoplasty by cartilage allograft. J Cosmet Dermatol 24: e16724.
- Wan R, Weissman JP, Williams T, et al. (2023) Prospective clinical trial evaluating the outcomes associated with the use of fresh frozen allograft cartilage in rhinoplasty. Plast Reconstr Surg Glob Open 11: e5315.
- Mohan R, Shanmuga Krishnan RR, Rohrich RJ (2019) Role of fresh frozen cartilage in revision rhinoplasty. Plast Reconstr Surg 144: 614-622.
- Singh R, Singh D, Singh A (2016) Radiation sterilization of tissue allografts: A review. World J Radiol 8: 355-369.
- Gryskiewicz JM (2008) Dorsal augmentation with AlloDerm. Semin Plast Surg 22: 90-103.
- Gentile P (2023) Rhinofiller: Fat grafting (surgical) versus hyaluronic acid (non-surgical). Aesthetic Plast Surg 47: 702-713.
- Giammarioli G, Liberti A (2023) Non-surgical rhinoplasty technique: An innovative approach for nasal reshaping with hyaluronic acid fillers. J Cosmet Dermatol 22: 2054-2062.
- Lee W, Moon HJ, Yang EJ (2020) Comments on “filler rhinoplasty based on anatomy: The dual plane technique”. JPRAS Open 38: 313-315.
- Al-Taie DS, AlEdani EM, Gurramkonda J, et al. (2023) Non-Surgical Rhinoplasty (NSR): A systematic review of its techniques, outcomes, and patient satisfaction. Cureus 15: e50728.
- Jung GS, Chu SG, Lee JW, et al. (2019) A safer non-surgical filler augmentation rhinoplasty based on the anatomy of the nose. Aesthetic Plast Surg 43: 447-452.
- Jasin ME (2013) Nonsurgical rhinoplasty using dermal fillers. Facial Plast Surg Clin North Am 21: 241-252.
- Trivisonno A, Cohen SR, Magalon G, et al. (2019) Fluid cartilage as new autologous biomaterial in the treatment of minor nose defects: Clinical and microscopic difference amongst diced, crushed, and fluid cartilage. Materials (Basel) 12: 1062.
- Nikparto N, Yari A, Mehraban SH, et al. (2024) The current techniques in dorsal augmentation rhinoplasty: A comprehensive review. Maxillofac Plast Reconstr Surg 46: 16.
- Skouras A, Skouras G, Karypidis D, et al. (2012) The use of Medpor© alloplastic material in rhinoplasty: Experience and outcomes. J Plast Reconstr Aesthet Surg 65: 35-42.
- Keyhan SO, Ramezanzade S, Yazdi RG, et al. (2022) Prevalence of complications associated with polymer-based alloplastic materials in nasal dorsal augmentation: A systematic review and meta- analysis. Maxillofac Plast Reconstr Surg 44: 17.
- Kim HS, Park SS, Kim MH, et al. (2014) Problems associated with alloplastic materials in rhinoplasty. Yonsei Med J 55: 1617-1623.
- Popko M, Bleys RLAW, de Groot JW, et al. (2007) Histological structure of the nasal cartilages and their perichondrial envelope. I. The septal and lobular cartilage. Rhinology 45: 148-152.
- Bleys RLAW, Popko M, De Groot JW, et al. (2007) Histological structure of the nasal cartilages and their perichondrial envelope. II. The perichondrial envelope of the septal and lobular cartilage. Rhinology 45: 153-157.
- Ronaldo doAmaral JFC (2012) Isolation of human nasoseptal chondrogenic cells: A promise for cartilage engineering. Stem Cell Res 8: 292-299.
- Chiu LLY, To WTH, Lee JM, et al. (2017) Scaffold-free cartilage tissue engineering with a small population of human nasoseptal chondrocytes, Laryngoscope 127: E91-E99.
- Reuther MS, Briggs KK, Neuman MK, et al. (2014) Volume expansion of tissue engineered human nasal septal cartilage. J Otol Rhinol 3: 1000172.
- Aksoy F, Yildirim YS, Demirhan H, et al. (2012) Structural characteristics of septal cartilage and mucoperichondrium, J Laryngol Otol 126: 38-42.
- Kridel RWH (1995) Grafts and implants in revision rhinoplasty. Facial Plast Surg Clin North Am 3: 473-486.
- Cissell DD, Hu JC, Griffiths LG, et al. (2014) Antigen removal for the production of biomechanically functional, xenogeneic tissue grafts. J Biomech 47: 1987-1996.
- Wee JH, Mun SJ, Na WS, et al. (2017) Autologous vs irradiated homologous costal cartilage as graft material in rhinoplasty. JAMA Facial Plast Surg 19: 183-188.
- Menger DJ, Nolst Trenité GJ (2010) Irradiated homologous rib grafts in nasal reconstruction. Arch Facial Plast Surg 12: 114-118.
Corresponding Author
Gagik Hakobyan, DMSC, PhD, Professor, Head of Department of Oral and Maxillofacial Surgery, Yerevan State Medical University, Yerevan, Armenia.
Copyright
© 2025 Harutyunyan A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.