Trauma Cerebrospinal Fluid Otorrhea Treated Conservatively by Upright Position
Abstract
Cerebrospinal fluid otorrhea is common with basilar skull fractures. Treatment includes conservative and surgical treatment. Conservative treatment includes bed rest, head elevation to 20 degrees, avoiding nose blowing, and so forth. After these treatments have been implemented, the cerebrospinal fluid otorrhea doesn't cease, normally, continuous lumbar drainage and repair of the fistula are required. In this case, we improved the conservative method by raising the head from 20 to 90 degrees, upright position, cerebrospinal fluid otorrhea was cured. The level of head elevation should not be tried for more than two times, that would put the patient in a risk of intracranial infection. But we still think that this conservative treatment, raising the head to 90 degrees in upright position, is worth considering in some special cases.
Keywords
Trauma cerebrospinal fluid otorrhea, Conservative treatment, Upright position
Introduction
Cerebrospinal fluid otorrhea is common with basilar skull fractures and occurs in 2~20.8% of patients with head trauma [1]. Meningitis develops in 10~25% of these patients. Treatment includes conservative management, operative management, and endoscopic approaches, etc. [2] Conservative treatment includes raising the head to some degrees, antibiotic prophylaxis, avoiding blowing noses, etc. We report a case that was resolved conservatively by raising the head from 20 to 90 degrees.
Case Report
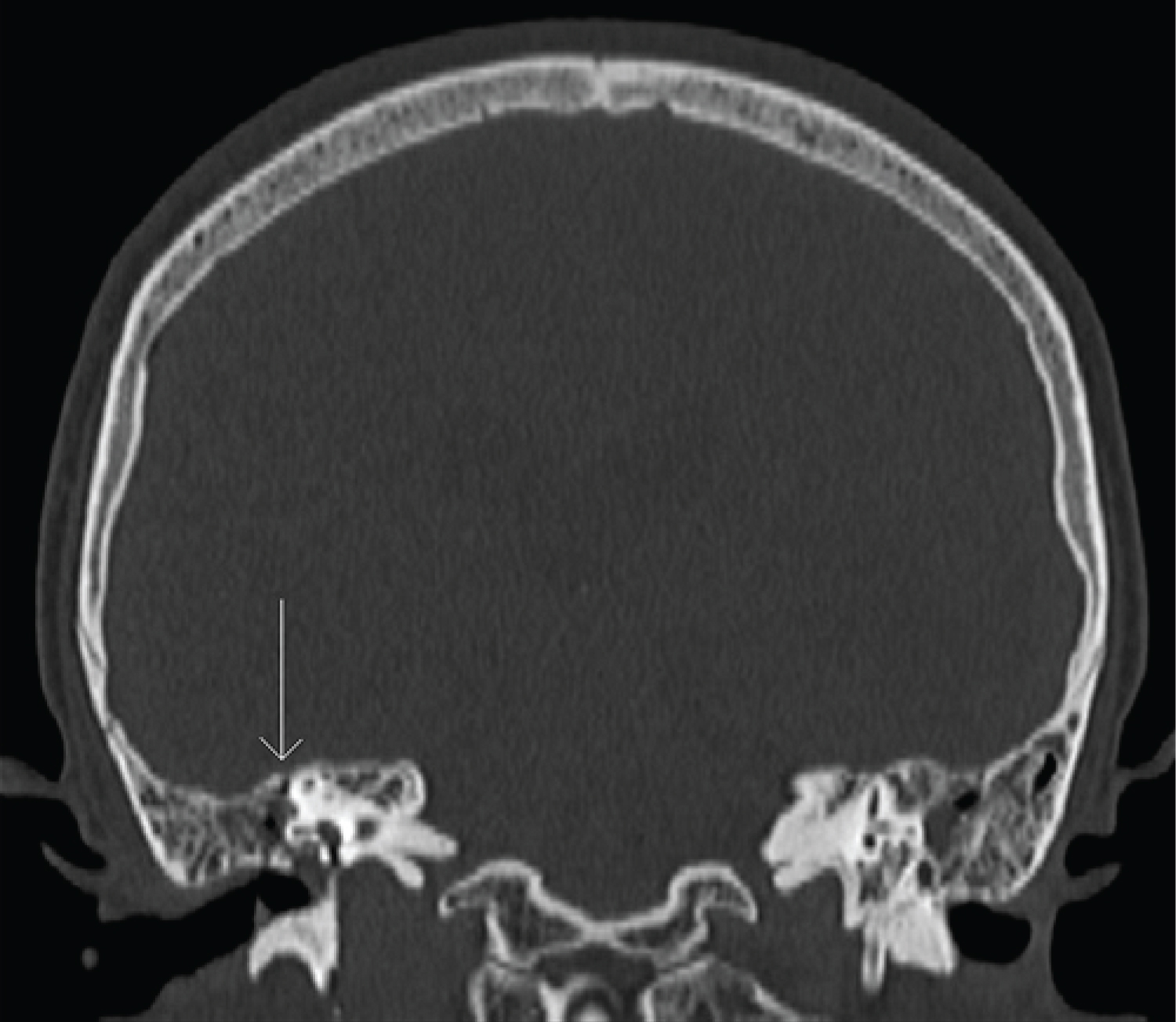
A 50-year-old woman was admitted to our hospital for a brain injury following a traffic accident that involved a lateral impact. When she presented to our department, she was conscious, although a pink liquid was seen leaking from her right ear. Head computed tomography (CT) showed a linear basilar skull fracture through the mastoid part of the temporal bone. Thin-slice three-dimensional CT showed the skull fracture. The coronal CT image (Figure 1) showed the fracture line extending to the right external auditory canal. Consequently, a central basilar skull fracture was diagnosed. The patient was treated conservatively by raising the head to 20 degrees, sleeping on her right side, antibiotic prophylaxis for 1 week, cefazolin 2 grams per day, avoiding blowing her nose, maintaining unobstructed defecation, and disinfection of the external auditory canal with iodine twice a day.
The cerebrospinal fluid leakage lasted for 15 days, the liquid gradually became pale yellow. We strongly recommended continuous drainage of the lumbar cistern to avoid meningitis. But the patient refused. This time we improved the method, raising the head from 20 to 90 degrees in upright position even in nighttime. The cerebrospinal fluid leakage gradually decreased and finally resolved 5 days later. No infection was detected on bacterial cultures of the leaking CSF. At the 1-month follow-up, the patient was well, with no facioplegia, dizziness, or face stolidity; the only finding was right hearing loss.
Discussion
Treatment of cerebrospinal fluid otorrhea includes conservative and surgical management [2]. Most authors think that the condition should be treated conservatively only for 3 to 7 days [2-4]. After this, continuous lumbar drainage [5] and repair of the fistula are required. According to our national treatment guidelines [6], a continuous leakage for more than 15 days should be managed surgically, so the patient had been undertaken conservative treatment for the first 15 days. The leakage still appeared. Because of the patient's strong refusal, we were forced to change the management, raising the head from 20 degrees to 90, even in the night sleeping time. The cerebrospinal fluid otorrhea gradually decreased and finally resolved.
It is well-known that cerebrospinal fluid leakage is cured by the closure of the leak. The cerebral tissue compressed the leak, and a regenerated layer of fibrous tissue or mucosa closed the leak [2]. When the head raised to 20 degrees, the leak might have not been completely blocked by the cerebral tissue, it didn't cease. When the head raised to 90 degrees, the leak might have been completely blocked, and it was cured. However, the level of head elevation should not be tried for more than two times, that would put the patient in a risk of intracranial infection.
Why did no intracranial infection happen? We think that there were two reasons: 1) The use of antibiotic prophylaxis. Although the antibiotic prophylaxis is still controversy, we think it is useful in the treatment of cerebrospinal fluid otorrhea; 2) Disinfection of the external auditory canal.
With conservative treatment, there is no trauma, it is easy to implement, and it is readily accepted by patients. The disadvantage is that it increases the risk of intracranial infection. Upright position in nighttime is very tired, the patient should overcome it. However, intracranial infection and recurrence may still occur after surgical treatment [7,8]. Lumbar drainage could lead to brain herniation [9]. So surgical treatment and lumbar drainage also have shortness.
Conclusion
The level of head elevation should not be tried for more than two times, that would put the patient in a risk of intracranial infection. But we still think that this conservative treatment, raising the head to 90 degrees in upright position, is worth considering in some special cases.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
None.
Author Contributions
Shuguang Zhang: Conceive the idea, edit the paper; Wenming Wang: Data collect and analyze, paper write and submit.
References
- Ross M, Lang E (2012) Does antibiotic prophylaxis prevent meningitis in patients with basilar skull fracture. Ann Emerg Med 60: 624-625.
- Ziu M, Savage JG, Jimenez DF (2012) Diagnosis and treatment of cerebrospinal fluid rhinorrhea following accidental traumatic anterior skull base fractures. Neurosurg Focus 32: E3.
- Alagöz F, Daglıoglu E, Korkmaz M, et al. (2015) Surgical management of traumatic cerebrospinal fluid fistulas with associated lesions. Ulus Travma Acil Cerrahi Derg 21: 450-456.
- Phang SY, Whitehouse K, Lee L (2016) Management of CSF leak in base of skull fractures in adults. Br J Neurosurg 30: 596-604.
- Hussein M, Abdellatif M (2019) Continuous lumbar drainage for the prevention and management of perioperative cerebrospinal fluid leakage. Asian J Neurosurg 14: 473-478.
- Zhongcheng W (2015) Neurosurgery. China. Hubei Science & Technology Press 435-437.
- Ringel B, Carmel-Neiderman NN, Peri A, et al. (2018) Continuous lumbar drainage and the postoperative complication rate of open anterior skull base surgery. Laryngoscope 128: 2702-2706.
- McCutcheon BA, Orosco RK, Chang DC, et al. (2013) Outcomes of isolated basilar skull fracture: readmission, meningitis, and cerebrospinal fluid leak. Otolaryngol Head Neck Surg 149: 931-939.
- Nasi D, Dobran M, Iacoangeli M (2016) Paradoxical brain herniation after decompressive craniectomy provoked by drainage of subdural hygroma. World Neurosurg 91: 673.e1-673.e4.
Corresponding Author
Wenming Wang, Neurosurgery, The First People's Hospital of Kunshan, No.91 West Qianjin Road, Kunshan, Jiangsu Province, 215300, China, Tel: +86-13656268761
Copyright
© 2022 Zhang S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.