The Microlift, a Composite Biplane Mini-Face Lifting
Background
Thread face lifting procedures are gaining more and more interest among patients seeking an easy cheap and non-harmful rejuvenating facial attempt. It appears that a surgical lighter procedure than the standard facelift, though strictly biplane microlift (SMAS and skin are elevated together without separation) is technically feasible and still easy to perform under strict local anesthesia and on a outpatient basis. To rejuvenate properly the face by surgical means, it seems that the biplane microlift may represent a solution to solve the problem of slight to moderate facial aging. Minilfts have been the old and first surgical solution of treatment directed to combat the aging facial process. Composite and MACS Minilfts of the face have already gained popularity [1]. Composite flaps have become used widely. Stocchero [2] advised a purse string of the Smas, Bonnefon [3] has advocated a main vertical composite flap, but going subperiosteally, which I do not agree for all cases, Saleh [4] combines a minilift and threads.
These procedures are gaining a place vacant before, in a field where thread lifts performed by non-surgeons are dominating the scope of easy rejuvenation. There is a strong appeal within the patients population to undergo minimal face lifts (Stephenson, [5-7]. For the Microlift, a biplane composite minilift of the face, I devised a simple method, and more harmonious, because there is a nice regularity of the tension through multiple layers od SMAS and skin pulled together undetached, a creation of a double layer of extended Smas adhesion in the pre-tragal area, which gives very natural results. Deep Dissection is performed minimally only below the SMAS layer, not under the skin at all, with preservation of a maximum of Furnas ligaments, in order to pull the entire face in a strong manner, due to the suturing of the dissected SMAS on the top of the preserved peri-auricular SMAS deep carpet, as an on top extra layer.
Microlift the surgical Method
1. Anesthesia: local infiltration of diluted lidocaine + adrenalin 0001 :1 cc of lidocaine. 0, 5/1000 is mixed with 100cc of saline +. Usually30 to 50 cc are used for each side.
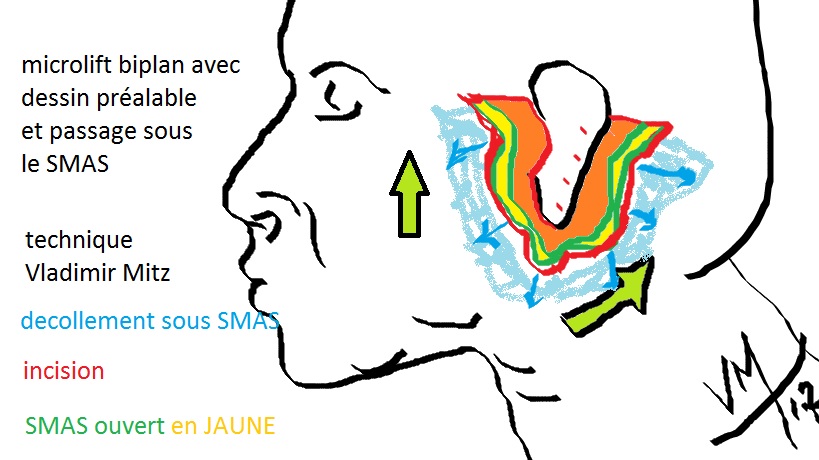
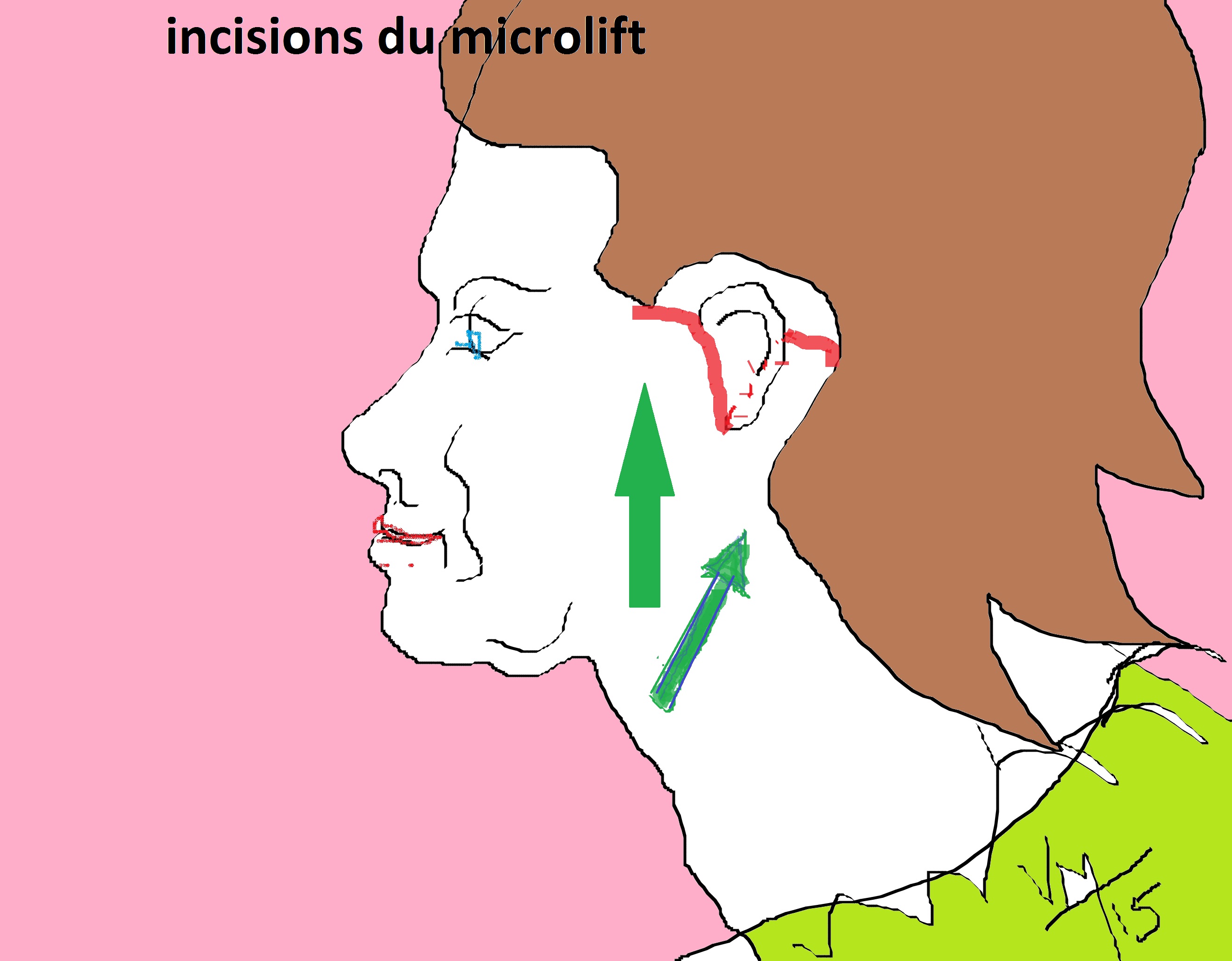
2. Design of skin excision: a predesigned periauricular incision is used in order to keep a nice balance of skin redraping. (Figure 1 and Figure 2 and Figure 3): The incision respects the hairy temporal area, and extends behind the ear, with a pre-capillary extension, toward the retro-auricular, and mastoid areas, in order to pull the neck extra skin to be removed. The width of the predesigned skin excision depends on the amount of skin laxity, evaluated by pinch test prior to the surgery. It is from 25 to 45mm, depending of each case; correction by additional excision is always possible if the pull does not satisfy the surgeon at end of the procedure, without a strangulating excitement.
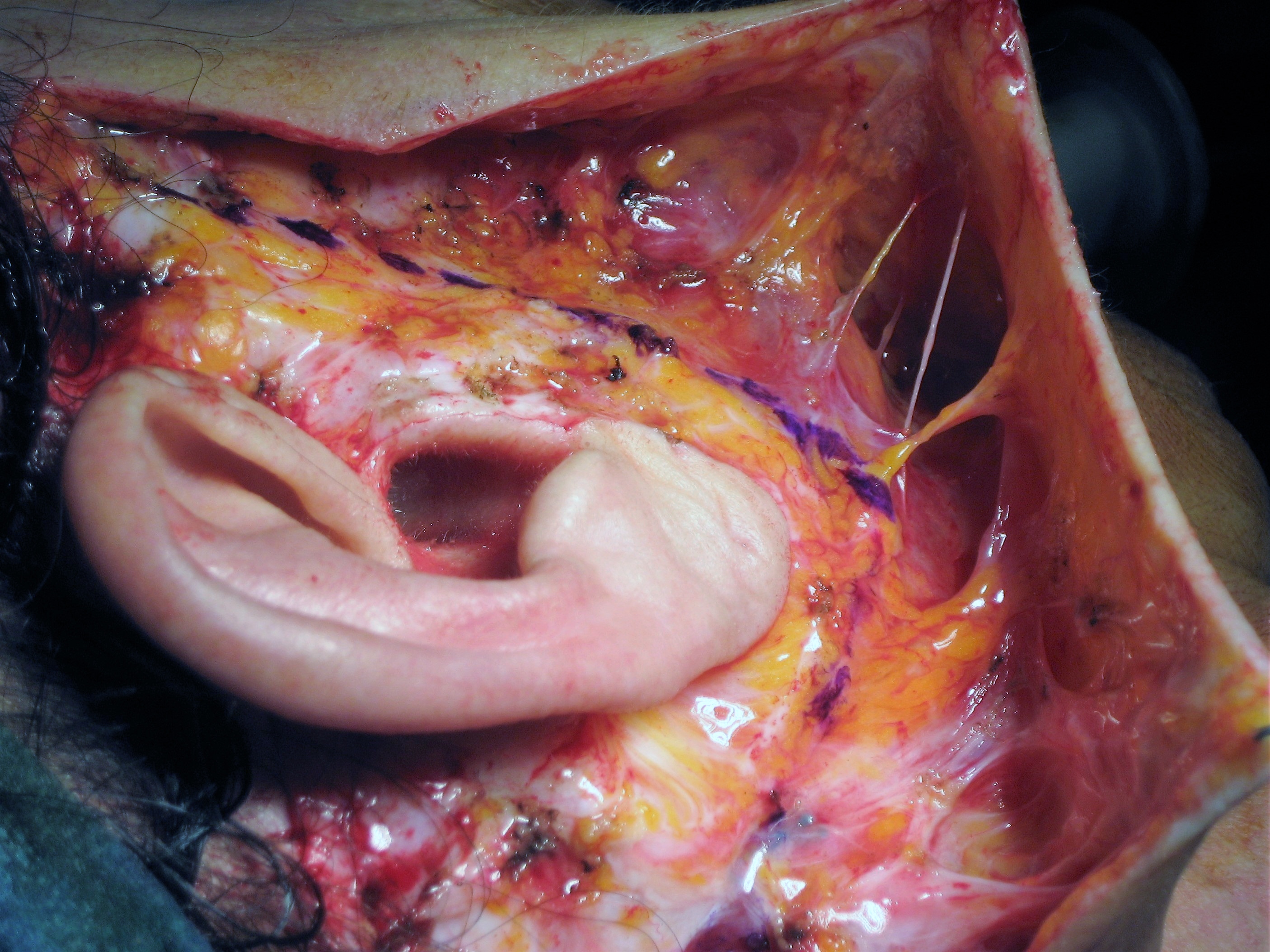
3. Skin excision: (Figure 4) The peri-auricular skin excision is performed, leaving the SMAS layer intact in the depth of the operating field. It is not a simple de-epithelialization, but a removal of the entire skin around the ear; Upper limit of the skin excision is the temple hairy area, downward limit is the mastoid hairline behind the ear.
4. Peripheral incision of the SMAS layer and neck penetration: The Smas is incised at the distal border of skin excision, This maneuver is quite easy in the cheek area, above the parotid gland; it is more delicate behind the ear, above the sternocleidomastoid fascia, where the delineation between Smas and deep muscles is less obvious; the incision in the cheek area must be delicate in order not to penetrate the parotid gland, and not to injury facial nerve branches. An extent of 2 to 3, 5 cm of Smas is thus preserved in front of the tragus. This layer will support an over coverage by the distal Smas -skin composite flap which will be mobilized in order to elevate the facial teguments in the face lift procedure.
5. Under the Smas, a careful and limited elevation is performed, with preservation of deep pedicles and ligaments, until the composite cheek flap moves up and backward. (Figure 5); This is a fundamental break through, because it appeared to me that rupturing or sectioning of the Furnas retaining ligaments of the face is not necessary to mobilize the cheek, once the parotid adherent Smas is freed: the retaining ligaments may be elongated by dissecting them gently with scissors opened vertically, or other dedicated instruments; this delicate freeing of the under SMAS layer preserves perfectly branches of facial nerve, the vascular and lymphatic supply of skin and deeper structures, thus allowing a quicker recovery time for a well performed microlift.
6. The retro- auricular area is uneasy to free: The main difficulty stays in this retro-auricular area, where the dissection plane between the sterno-cleido muscular fascia and the deep skin is sometimes tricky to find in order to redrape the posterior part of the platysmal complex structures. Care has also to be taken in freeing the auricular lobule, not to injure the tiny auricular sensibility nerve.
7. A thorough hemostasis is mandatory: This step is a precise one, because the operated patients are on an ambulatory scheme, and we do not want them to come back in an emergency situation with a giant hematoma; the hemostasis may provoke some mimic muscle contractions by direct stimulation of the nerve branches below the freed SLMAS layer; no drains are necessary though, at least in my short experience.
8. A deep layer of Smas sutures is then performed: creating a Smas overlap of at least 2 to 4 cm width. Slow resorbable sutures are used. The design of the skin excision and SMAS incision allows a vertical vector to the cheek flap, with even a rotational advancement inward of the SMAS below the zygoma. The distal Smas flap is sutured to the tragus fibrotic layer, to the sub-zygomatic fibrous angle. In the mastoid area, the pull of the deep layer is at a 45° angle, toward the mastoid fibrous structures to be anchored to.
9. The resultant double layer of Smas in front to the ear: is not perceived once sutures are done ,nor by fingering the surface, nor by view in my experience; May be that this doubled Smas layer will bring some better resistance to relapse in time; Until now, I did not practice any local biopsy in the cases I have been performing a secondary microlift; there is no proof what so ever that this hypothesis may be true or not. The auricular earlobe is carefully put back in his proper location, in order to avoid the ear elongation (devil earlobes), by a suture of resorbable stitch fixing the skin-SMAS flap to the parotid fascia.
10. The skin is then sutured: with a double layer of 4:0 resorbable sutures
11. Control of excised skin: (Figure 6); I try to not forget to make photographs of the amount of excised skin, on both sides; this is intended to keep a precise record of each procedure, and to be able to show the picture to the patient, once he comes back for the following of his case.
12. A sterile varnish: is applied on the sutures to protect them from fingering by an anxious patient.
13. A Compressive dressing: is applied for 24 or 48 hours.
14. The patient is discharged on an Ambulatory procedure, after a few hours.
15. The fatty neck and jowls: a local liposuccion (lipolift) is performed before any incision, as the first operative step; The syringe technique is preferred; the fat is kept in order to add a lipofilling to the central face, if needed and scheduled with the patient approval.
16. Additional surgeries: blepharoplasty, facial injections, dermabrasion of the upper lip are performed at the end of the microlift, when scheduled.
17. Duration of the procedure in the operative room: usually 90 to 120 minutes.
Principles
The aim of the procedure is to rejuvenate the starting signs of the aging process, mostly located in the jowls and the neck areas. The procedure is not intended to fill or alleviate permanently the nasolabial folds or the central face aging.
The overlapping of 2 layers of the SMAS in front of the ear, in the parotid and cheek area, allows a good adhesion of tissues, about 2 cm to 3 cm of width, maintaining the result for several years in most of the cases i performed. There is no exaggerate tension imposed on the tragus, because the elevated Smas flap is sutured toward the deep layers of the tragus, on the SMAS origin, thus avoiding skin disruption.
Results
31 patients well-selected patients have been operated with this technique since 2013, with minimal complications and complaints.
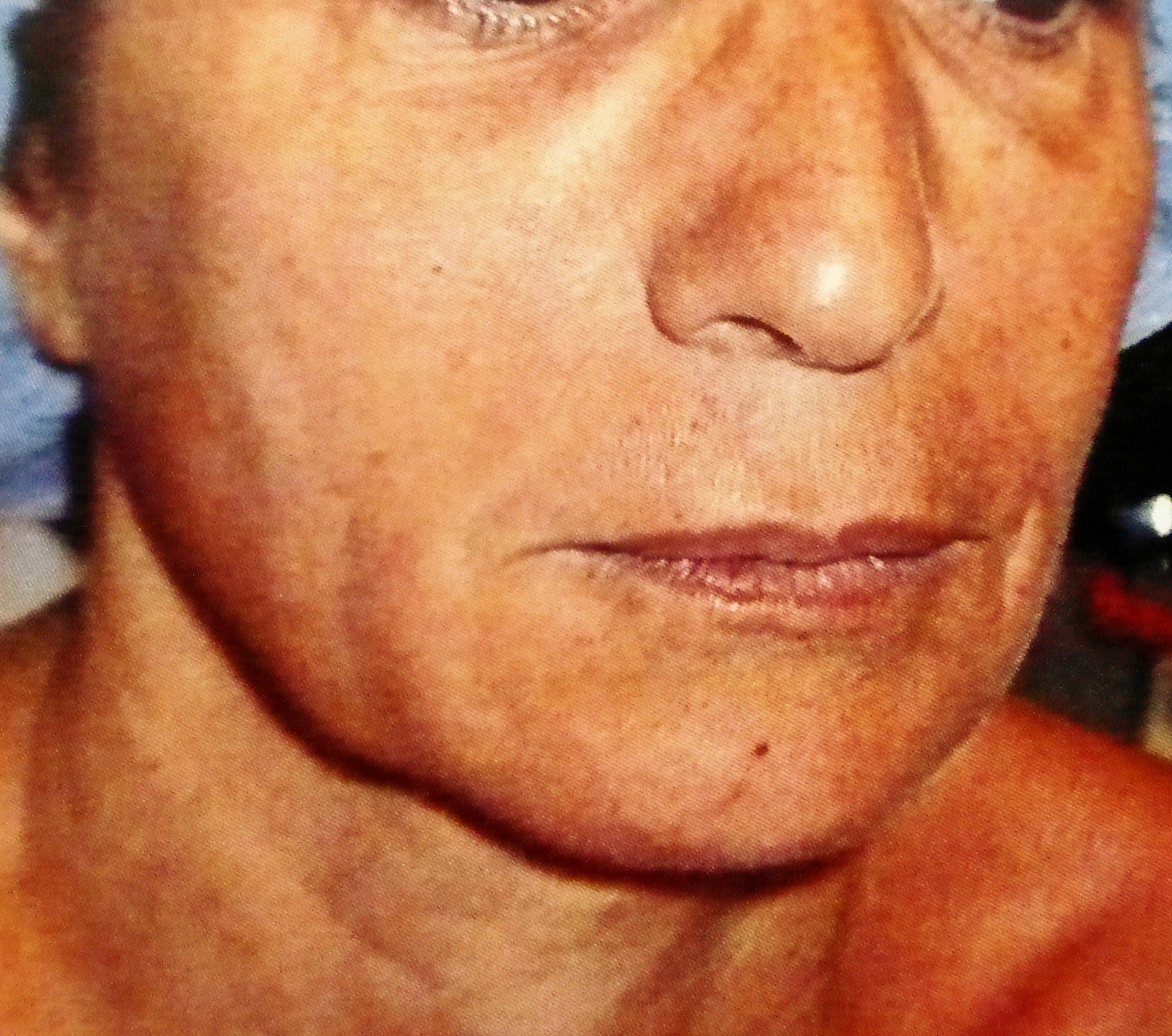
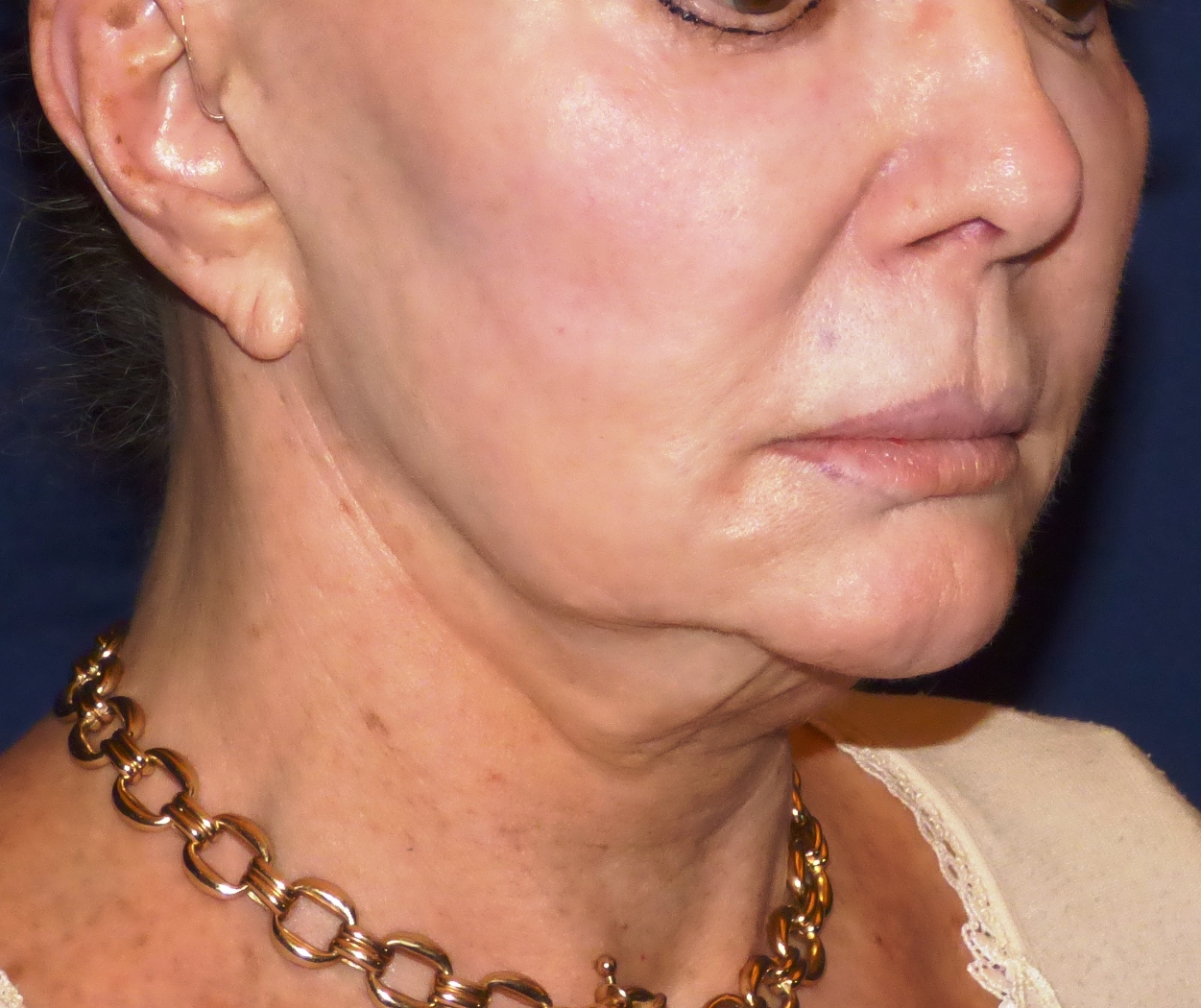
2 examples are shown (Figure 7 and Figure 8 and Figure 9 and Figure 10 and Figure 11 and Figure 12 and Figure 13 and Figure 14 and Figure 15 and Figure 16).
6 patients had a moderate skin relapse after one year; 3 of them asked for a secondary skin retightening. This has been performed under local anesthesia and as an outpatient procedure.
Conclusion
The Microlift, a composite biplane facial lifting technique, is an adjunct to our cervico-facial Biplane extended technique; it may help to operate quickly and effectively patients who would otherwise search in thread lifts or other medical devices, a non-surgical solution because of their fear toward a more complex procedure.
Disclosure
The author has no financial disclosure to declare and there was no funding for the production of this article.
References
- Mitz V, Peyronie M (1976) The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg 58: 80-88.
- Mitz V (2018) The biplane microlift. Principles, technic, results. Ann Chir Plast Esthet 63: 262-269.
- V Mitz (2021) Rhytidoplasty: My current techniques, biplane extended facelift, and microlift. Aesthetic Fac Surg 463-490.
- Bonnefon A (1995) Deep vertical facelift. Development of a concept. Ann Chir Plast Esthet. 40: 327-339.
- Stocchero IN (2007) Shortscar face-lift with the RoundBlock SMAS treatment: A younger face for all. Aesthetic Plast Surg 31: 275-278.
- Stephenson KL (1970) The "mini-lift," an old wrinkle in face lifting. Plast Reconstr Surg 46: 226-235.
- Saleh DB, Brierley N, Riaz M (2021) “R” face and neck lift: a modified technique for en-bloc facial rejuvenation. Plast Aesthet Res 8: 10.
Corresponding Author
Vladimir Mitz, MD, Private Practice, France
Copyright
© 2022 Mitz V. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.