Miniincisionl versus Median Sternotomy to the Cardiac Myxoma: A Comparison of Outcomes
Abstract
Background: Cardiac myxoma are the commonest benign cardiac tumor, its pathological character make it higher tendency for showering and embolic complications. Surgery done on urgent base to avoid its complications. Its location in atria make it safely and feasible to minimal invasive approaches.
Methods: This is retrospective study analysing data of 68 patients operated in zagazig university hospital and Naser institutes from July 2011 to December 2020. 49 patients operated through standard median sternotomy while 19 patients through mini incisions (right anterior mini thoracotomy and partial lower sternotomy).
Results: Demographic data of patients in both groups are non significant , while by pass time and aortic cross clamp is significantly higher in minimal approaches than standard and Tumor size was significantly bigger in standard median sternotomy group. Variables in post operative groups regarding ICU stay and hospital stay are significantly shorter in minimal approaches.
Conclusions: Mini incisions are safe and feasible in cardiac myxoma resection with comparable outcome to standard approach .its advantages in less post operative pain, less stay in hospital and less infection and better osmosis are predicators for encouraging to practicing these approaches.
Keywords
Benign cardiac tumor, Myxoma, Median sternotomy, Right minithoracotomy
Abbreviations
LA: Left atrium; AF: Atrial fibrillation; MS: Median sternotomy
Background
Benign cardiac tumor are cardiac pathology with incidence about 0.3%. OF which Cardiac myxoma is about 75%. No reported age prevalence and more in female than male. Commonly located in Atria and less in the ventricle [1] No specific symptoms characteristic to cardiac myoma, symptoms may be secondary to valve obstruction, embolic manifestation secondary to tumor pathology or incidental finding without symptoms. Transthoracic echocardiography is the basic diagnostic tool, with specificity 93% [2]. Surgery is the definitive therapy and carried on urgency basis. Median sternotomy is the standard approach to cardiac myxoma [3]. However Over last three-decade alternative non sternal approaches have been developed initially in ASD closure and valve surgery [4]. Its outcome have reported in many studies in term of less pain, less bleeding and better cosmesis [5,6]. Due to rarity of cardiac myxoma, few reports document outcome of mini thoracotomy in myxoma surgery.
Main Text
To present or experience of mini-incisions and its feasibility and safety in resection of cardiac myxoma.
Methods
This is retrospective study analysing data of 68 patients operated in zagazig university hospital and Naser institutes from July 2011 to December 2020.
Surgical techniques
The surgical techniques are surgeon preference.
Median sternotomy
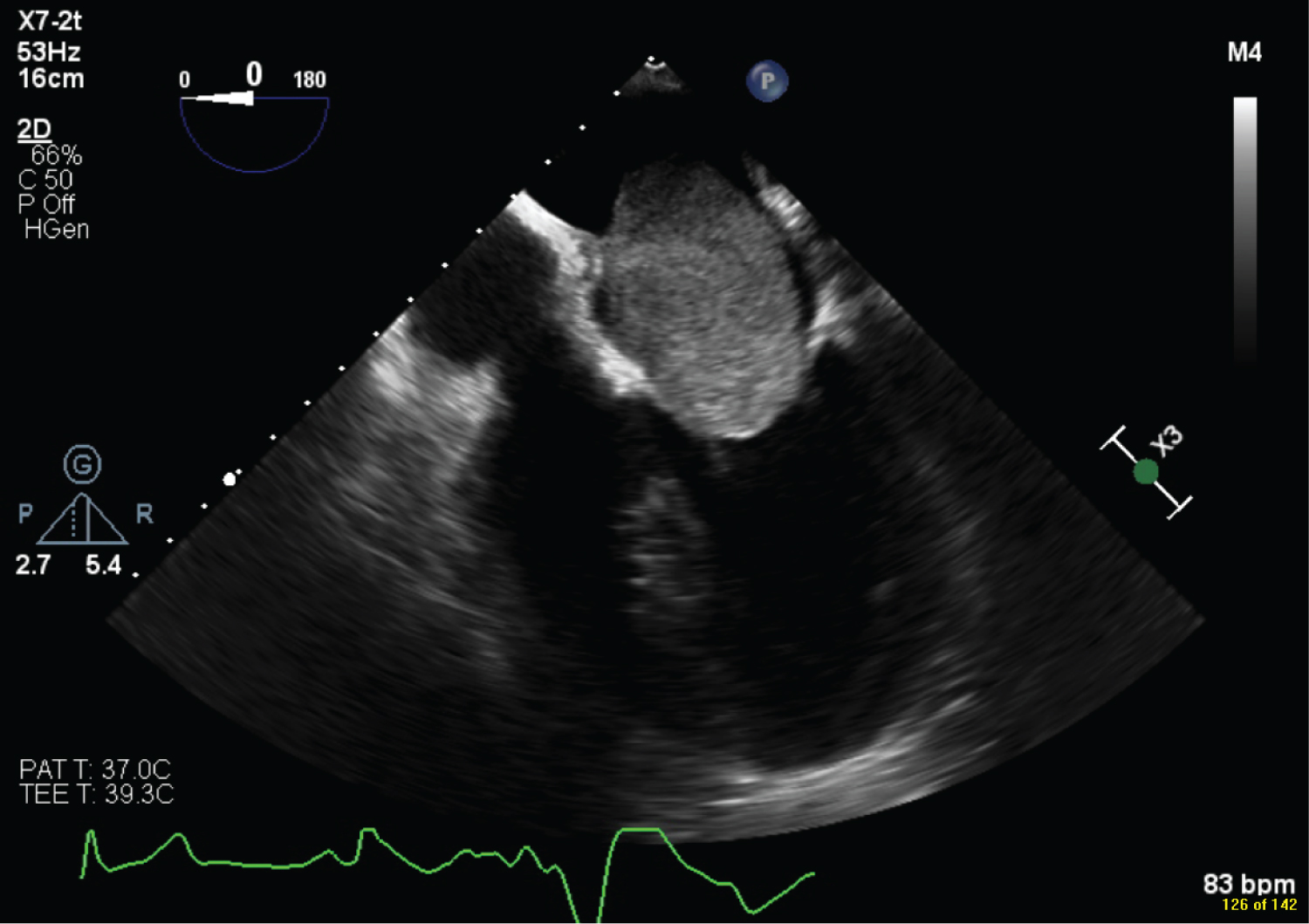
Under general anaesthesia. Aorto bicaval cannulation, antegrade cardioplegia. Incisions were individualized to appropriately remove the mass. Wean of bypass, Trans oesophageal echocardiography (TEE) to assess complete excision of mass, competency of the valves (figure 1).
Mini incisions
Partial lower sternotomy: Under general anaesthesia, 4 to 5 cm midline incision just below the sterno manburio junction extended to 1-2 cm above xiphoid process, aorto/bi caval cannulation. Antegradecardioplegia, right atrial incision, excision of fossa oval is with attached mass. Closure of surgical lines, wean of bypass, TEE for mass excision, no residual shunt, and valve competency.
Right Minithoracotomy: Under general anaesthesia with double -lumen endotracheal tube for single lung ventilation. The incision was made in 4th intercostal space, extended from right anterior axillary line to mid clavicular line. Femoral -femoral cannulation with superior caval cannulation. Pericardiotomy, aorto cross clamped and cardioplegia. Incisions according to tumor locations, size. Wean off bypass, TEE for complete mass excision.
Histopathological Examination
All resected tumors were sent to histopathological examination, and the diagnosis of myxoma was confirmed in all cases. Written informed consent was obtained from all participants, the study was approved by the research ethical committee of Faculty of Medicine, Zagazig University. The study was done according to The Code of Ethics of the World Medical Association (Declaration of Helsinki) for studies involving humans.
Statistical Analysis
Data obtained from medical records were compiled in an Excel spreadsheet. Data were then imported into Statistical Package for the Social Sciences (SPSS version 20.0) software for analysis.
Categorical variables were presented as frequency and percentage. Chi-square test (χ2) was used to test differences for categorical variables. P values were set at < .05 for significant results
Results
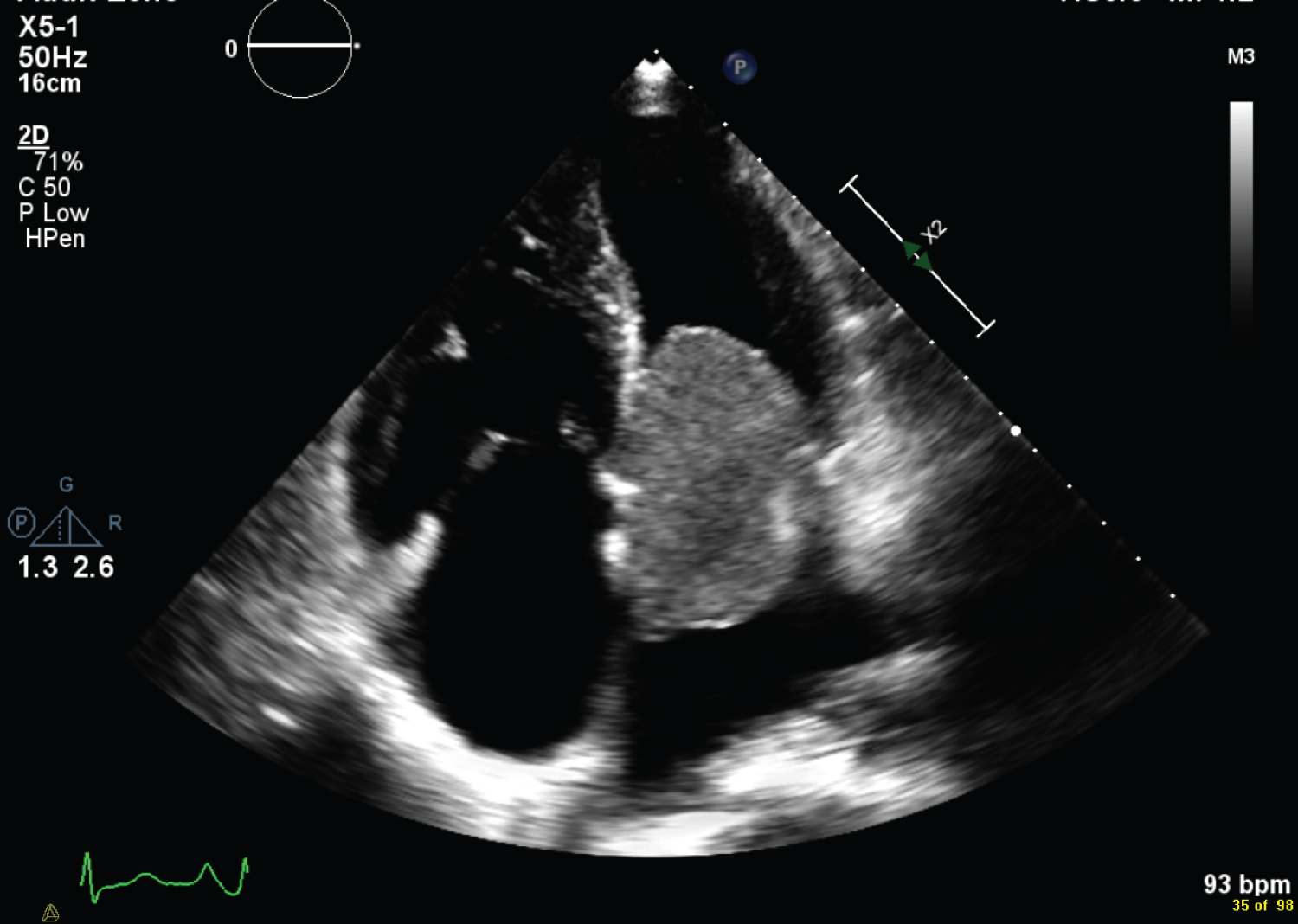
Mean age was 51 ± 13 years in median sternotomy while 47 ± 11 in mini-incisions group. With no significant difference in both groups. The majority of patients was female in both groups (66%). Embolic complications reported in 11 patients. Stroke was the most common complications in 9 patients while 2 patients complicated by peripheral emboli. Dyspnoea is the most common complaints 23 patients while 5 only have congestive symptoms TTE is the diagnostic tool in all cases (Figure 2).
The median sternotomy still the commonest incision for atrial myxoma in 49 patients (72%), while left atrium is the commonest tumor location 58 while right atrium 10 patients 57 ± 7 min (Table 1) preoperative demographic data.
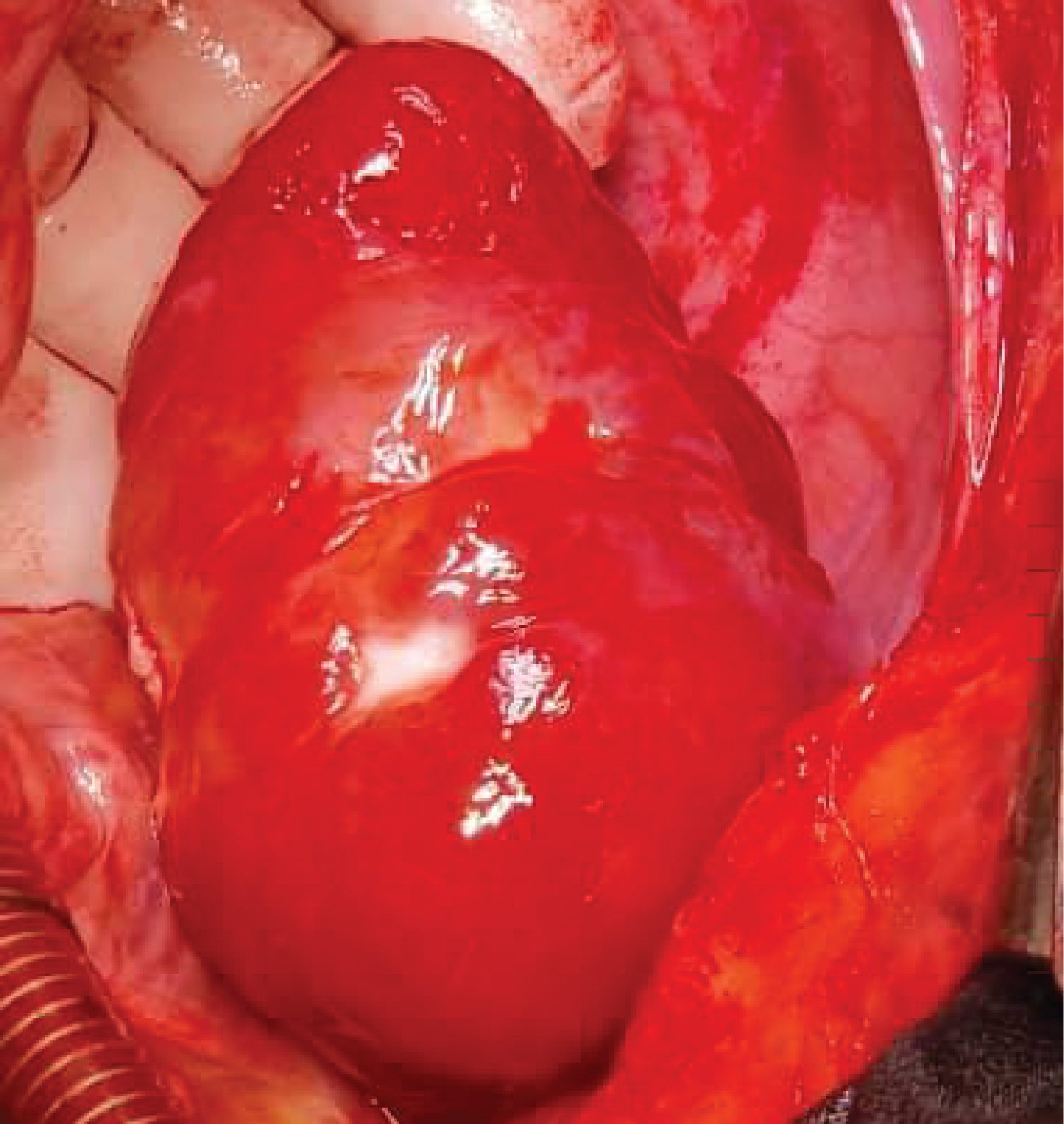
Right atrial approach is the comments incision for tumor resection. Mean cross clamp time was 67 ± 11 min and 87 ± 17min in both groups respectively while aortic cross clamp 57 ± 7 min & 73 ± 9 min in both groups. Mean tumor size was 4.8 cm in MS group while 4.1 cm in mini-incision group (Figure 3). All masses are hist pathologic analysed and reported as benign cardiac myxoma tumor (Table 2) intra operative variable.
The estimated ICU and hospital stay are comparable no statistical difference. The AF is the most common a post-operative arrythmia is more common in mediansternotomy than in mini-incision. Post-operative respiratory complication in term of atelectasis more with median sternotomy than miniincision. we report 1 case surgical site infection in median sternotomy , no cases in mini incision group (Figure 4). No reported mortality in both group/Table 3 post-operative.
Discussion
Benign Cardiac tumor are very rare with incidence 0.3% up to 75% are myxoma. Widely spread among females, no specific presentation. commonly located in Left atrium . Echocardiography is the diagnostic tool . unlike right sided mass which need further multi modality imaging.
AS right sided masses are malignant in nature. Surgical excision is the standard management [1]. Median sternotomy still the standard surgical approach for cardiac myxoma .Although minimal invasive approach is well established in valve surgery but it is outcome in myxoma reported in few studies [5].
In 1998 when KO, et al. reported first myxoma resection through right minithoracotomy [7] in our study. The majority of patients are females in both groups and tumor location in left atrium near 85% same finding in literature review. The time of bypass and aortic cross -time is prolonged in mini incision group than MS with higher significant P -value. And no negative impact post operative on bleeding or requirements for transfusion or re exploration. This is unlike recent study with Dong et al, who comparing minithoracotomy to median sternotomy showed no significant difference in aortic cross -time and cardiopulmonary bypass time but minithoracotomy has shorter hospital stay and more cosmetic outcome [8].
We documented less bleeding in mini incision group than median sternotomy and no transfusion in both group . Sama as Sawaki et al no significant difference in bleeding requiring operation in his study [9]. Atrial fibrillation the most common dysrhythmia reported 11 patients 9 of them in median sternotomy. Mihos, et al. related less arrythmia post minithoracotomy to less surgical trauma and less inflammation in mini incision than in median sternotomy [10].
Loulmet, et al. reported excision of left atrial myxoma through Right minithoracotmy on fibrillating heart [11]. Also video -assisted excision of benign cardiac mass [12] and even Robotically Kesavuori, et al. [13] compared robotically assisted surgery with the conventional sternotomy approach and showed statistically significant shorter length of stay in hospital in the robotically assisted group, although cardiopulmonary bypass time, aortic occlusion and ventilation times were shorter in the sternotomy group.
Partial lower sternotomy is another mini incision with proven outcome in valve surgery .Chen et al in his study reported myxoma excision safely through partial lower sternotomy [14] same with Risteski, P et al. document Triple valve surgery can be completed using lower partial sternotomy with benefits [15] Doty, DB et al. documented feasibility and safety of Partial sternotomy (lower half ) in cardiac valve operations [16].
We used partial lower sternotomy in three patients, Two of them trans right atrial incision and third case transverse bi atrial approach doubst technique it was feasible access with adequate exposure to tumor excision. We reported one case surgical site infection and one mortality in median sternotomy, No mortality in both groups, Tumor size was significantly larger in MS than mini incisions.
Tumor location in the atrium make it easy accessible through mini approaches. Right atrial incision is the commonest incision, other left atrium or bi atrial, Dubost incision all reported as incision in myxoma with good exposure and complete excision [17]. Some studies reports cryoablation or radiofrequency as adjunct to prevent recurrence. Can be safely used through mini incisions [18].
Conclusions
Mini incisions are feasible and save approaches in resection of cardiac myxoma. Tumor location in atria making it easily accessible through mini approaches. Its outcome are comparable to median sternotomy with proven its advantages regarding surgical site infection, pain, cosmosis and adequate resection with no recurrence.
References
- Reynen K (1995) Cardiac myxomas. N Engl J Med 333: 1610-1617.
- Sütsch G, Jenni R, von Segesser L, et al. (1991) Herztumoren: Häufigkeit, Verteilung, Diagnostik. Anhand von 20.305 Echokardiographien [Heart tumors: Incidence, distribution, diagnosis. Exemplified by 20,305 echocardiographies]. Schweiz Med Wochenschr 121: 621-629.
- Patel J, Sheppard MN (2010) Pathological study of primary cardiac and pericardial tumours in a specialist UK centre: Surgical and autopsy series. Cardiovasc Pathol 19: 343-352.
- Maraj S, Pressman GS, Figueredo VM (2009) Primary cardiac tumors. Int J Cardiol 133: 152-156.
- Hoffmeier A, Sindermann JR, Scheld HH, et al. (2014) Cardiac tumors: Diagnosis and surgical treatment. Dtsch Arztebl Int 111: 205-211.
- Bakaeen FG, Reardon MJ, Coselli JS, et al. (2003) Surgical outcome in 85 patients with primary cardiac tumors. Am J Surg 186: 641-647.
- Schaff HV, Mullany CJ (2000) Surgery for cardiac myxomas. Semin Thorac Cardiovasc Surg 12: 77-88.
- Dong NG, Zhang KL, Wu L, et al. (2018) Right anterolateral minithoracotomy versus median sternotomy approach for resection of left atrial myxoma. Thorac Cardiovasc Surg 66: 193-197.
- Ko PJ, Chang CH, Lin PJ, et al. (1998) Video-assisted minimal access in excision of left atrial myxoma. Ann Thorac Surg 66: 1301-1305.
- Mihos CG, Santana O, Lamas GA, et al. (2013) Incidence of postoperative atrial fibrillation in patients undergoing minimally invasive versus median sternotomy valve surgery. J Thorac Cardiovasc Surg 146: 1436-1441.
- Loulmet DF, Patel NC, Jennings JM, et al. (2008) Less invasive intracardiac surgery performed without aortic clamping. Ann Thorac Surg 85: 1551-1555.
- Kesävuori R, Raivio P, Jokinen JJ, et al. (2015) Quality of life after robotically assisted atrial myxoma excision. J Robot Surg 9: 235-241.
- Takazawa K, Fuse K, Konishi T, et al. (1992) Cryosurgery for left atrial myxoma with coronary artery bypass grafting. Kyobu Geka 45:1021-1023.
- Chen-Yuan Hsiao, Chih-Pei Ou-Yang, Cheng-Hsiung Huang (2012) Less invasive cardiac surgery via partial sternotomy. J Chin Med Assoc 75: 630-634.
- Risteski P, Monsefi N, Miskovic A, et al. (2017) Triple valve surgery through a less invasive approach: Early and mid-term results. Interact Cardiovasc Thorac Surg 24: 677-682.
- Doty DB, DiRusso GB, Doty JR (1998) Full-spectrum cardiac surgery through a minimal incision: Mini-sternotomy (lower half) technique. Ann Thorac Surg 65: 573-577.
- Shahzad G Raja, Jeremy Felderhof (2011) Excision of left atrial and right ventricular myxoma through biatrial approach: Correction please! Interact Cardiovasc Thorac Surg 12: 624.
- Wauthy P, Mircev D, Marinakis S (2016) Three years follow-up after cryoablation of a right atrial myxoma arising from the Koch's triangle. J Cardiothoracic Surg 11: 154.
Corresponding Author
Ehab Mohamed kasem, Assistant professor, Department of cardiothoracic surgery, Zagazig university, Zagazig, Sharkia, Egypt; Department of cardiothoracic surgery, King Abdullah medical city, Makkah, Saudi Arabia
Copyright
© 2022 Kasem EM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.