Survival Following Invasive Aspergillus Endocarditis Resection and Amphotericin B Washing
Abstract
Invasion of Aspergillus fungus into cardiac tissue is a rare occurrence typically seen in immunocompromised patients. Detection is typically a combination of galactomannan testing and imaging of heart tissue. Treatment of invasive cardiac aspergilloma can include intensive cardiac tissue debridement, repair and antifungal washout but has previously always resulted in patient death due to complications. This case presents a patient with extensive left heart Aspergillus invasion and right sided pulmonary embolus following chemotherapy for lymphoma with successful cardiac treatment and grafting of coronary vessels. Importantly, this patient survived for several years following surgery.
Keywords
Endocarditis, Cardiac aspergilloma, Aspergillus fumigatus
Introduction
Aspergillus is a ubiquitous mold that colonizes the human sin pulmonary tract via inhalation of fungal spores. It is an important cause of morbidity and mortality in immunocompromised hosts, although Aspergillus endocarditis is not common [1]. Prolonged neutropenia, high-dose corticosteroids, hematologic malignancies like acute leukemia, myelodysplastic syndrome, and recipients of allogenic stem cell and solid organ transplantation are at a high risk for development of invasive cardiac aspergillosis, and treatment includes a combined approach with surgery and antifungal management [2-5]. We present a case of successful management of invasive Aspergillus endocarditis in an immunocompromised patient.
Case Report
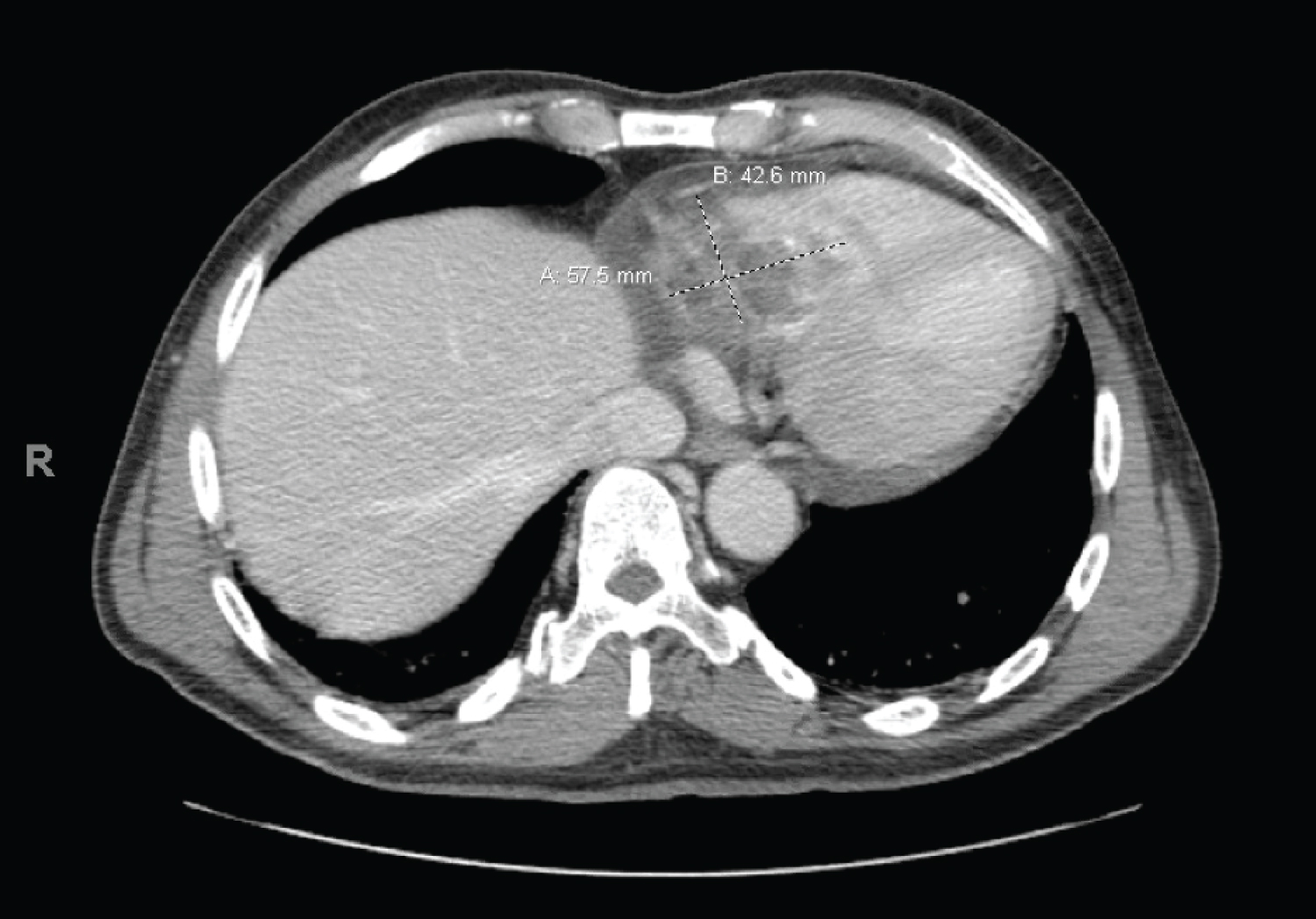
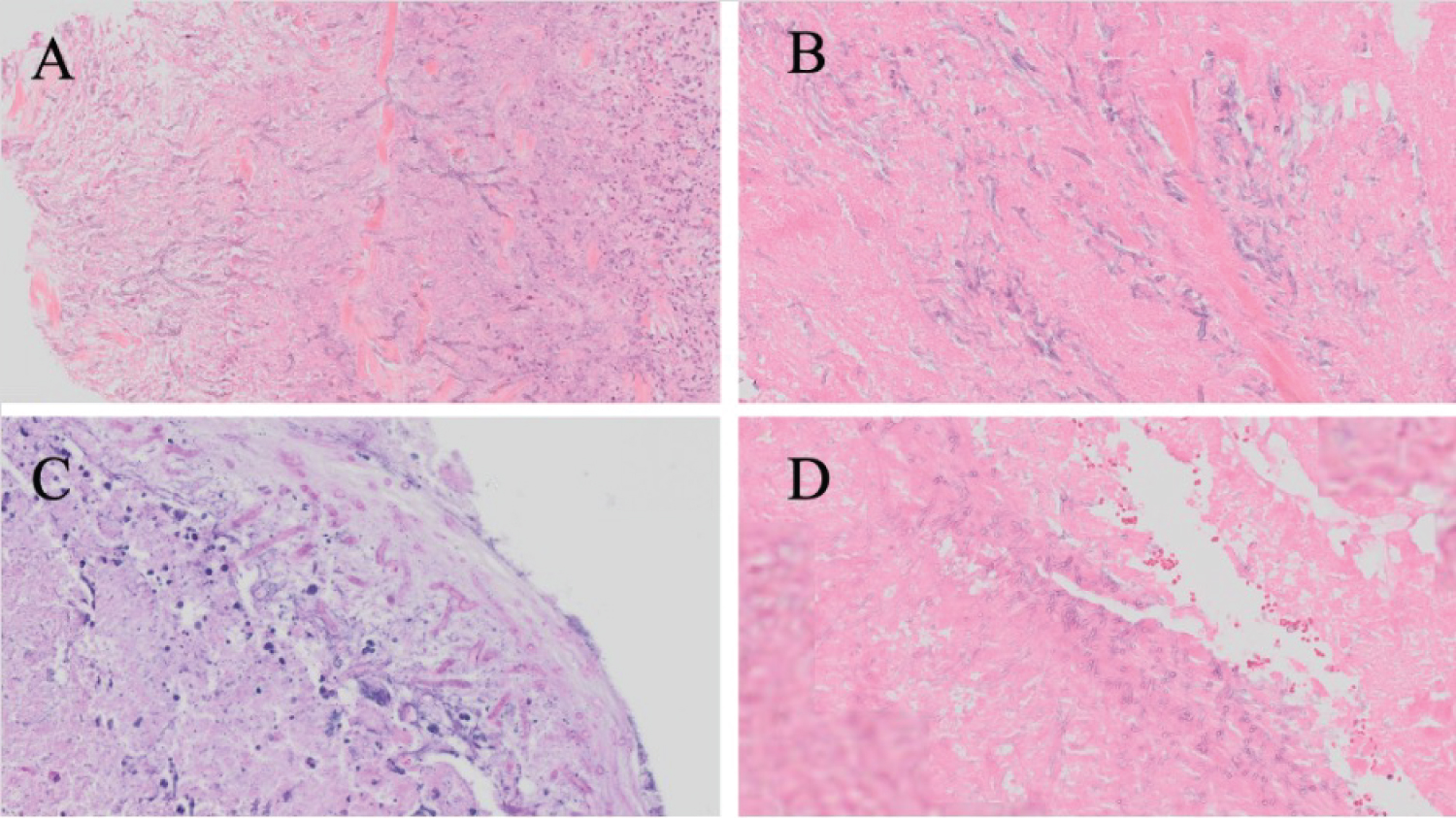
A 60-year-old African American male with history significant for Burkitt's lymphoma presented for routine follow-up after chemotherapy complicated by periods of neutropenia. He was diagnosed with Burkitt's Lymphoma ten months prior and treated with seven rounds of chemotherapy (cyclophosphamide, methotrexate, etoposide, doxorubicin, rituximab, and steroids). Per IDSA aspergillus guidelines, this patient was routinely tested for invasive aspergillosis using a serum galactomannan antigen assay [6]. He was tested monthly for 9 months, and all results were negative. Following chemotherapy, routine positron emission tomography (PET) scans and a follow up echocardiograph revealed a large tissue density measuring 5.3 cm × 3.2 cm with a second mass measuring 1.5 cm × 0.8 cm in his right heart. The mass involved the tricuspid valve and extended into the right ventricle. Transthoracic echocardiogram (TTE) revealed an ejection fraction (EF) of 50-55%. Computed tomography (CT) scan confirmed the presence of the right heart mass as well as a pulmonary embolism of the right pulmonary artery (Figure 1). Right heart catheterization with biopsy showed significant hyphae concerning for a fungal infection but no signs of relapsed lymphoma (Figure 2a). Blood cultures were negative for Aspergillus. However, galactomannan antigen assay was positive at 1.05 (index value < 0.5) and the patient was scheduled for surgery due to concerns for fungal endocarditis.
Perioperatively, a large right atrial and right ventricular mass was seen with biopsy consistent aspergillosis (Figure 2b and Figure 2c). Intraoperative transesophageal echocardiography (TEE) revealed a hypokinetic left ventricular function (EF of 55%) and moderate tricuspid regurgitation with a mass. A large fungating necrotic mass replaced the posterior tricuspid leaflet and extended into the adjacent right atrium and deep into the right ventricular walls to the level of the posterior and partially anterior papillary muscles. There were multiple small vegetations at the level of septal and anterior leaflets and adjacent chordae and papillary muscles. Extensive debridement was performed, and the valve was not amenable to repair. A radical resection of the myocardial aspergilloma was performed with debridement extending into healthy right ventricular myocardium. The right atrium and ventricle were copiously irrigated with Amphotericin B solution. The posterior tricuspid annulus and adjacent right ventricular wall were reconstructed with an endoventricular patch of bovine pericardium. A segment of healthy anterior leaflet with adjacent chords was transposed to posterior annulus to reinforce the repair and a replacement valve was placed, which moved freely.
Embolectomy of the right pulmonary artery was performed. The embolus had a similar gross appearance to the fungal vegetations, and biopsy revealed fungal features (Figure 2d).
While weaning from cardiopulmonary bypass, ST segment elevation was noted in the inferior leads and TEE showed inferior left ventricular wall hypokinesia suggestive of right coronary hypoperfusion. Right ventricular function was normal. These findings, which correlated with prior location of the aspergilloma and the extent of debridement, suggested distal dominant right coronary artery hypoperfusion. Bypass of the posterior descending artery was performed using a saphenous vein graft with resulting improvement of ST segment elevation and wall motion. Post-procedure TEE demonstrated an EF of 50% with a functional tricuspid prosthesis.
The patient was started on Amphotericin B post-procedure, which was later discontinued due to elevated creatinine concerning for Amphotericin B related acute kidney injury. The patient was then switched to voriconazole with good response. Four follow-up PET and CT scans showed no evidence of disease recurrence. Serum galactomannan assay remained negative until this patient passed away several years later in hospice care due to complications associated with lymphoma recurrence and malnutrition.
Discussion
Invasive Aspergillus is typically seen in immunocompromised hosts, and factors that increase risk of fungal endocarditis include intravenous drug abuse, extended antibiotic use, drug induced immunocompromise, open heart cardiac surgery and prosthetic valves [2-5]. Non-invasive fungal endocarditis alone recurs in 29% of cases, and the typical morbidity and mortality rate for patients with aspergillus endocarditis is 80-96% [1,7]. Invasion of Aspergillus into surrounding heart valves and chambers is even more rare and always fatal in the small number of cases reported [4]. The diagnosis of aspergillus endocarditis is difficult due to poor yield of blood cultures [7]. Serum fungal markers like aspergillus galactomannan and beta-D-glucan can be used with radiologic and clinical signs for diagnosis. Galactomannan assay has a reported sensitivity of approximately 70% in patients with hematologic malignancies, which decreases if patients are on antifungal therapy and thus its use is limited [8]. Biopsy and histopathology are essential, which may cause diagnostic delays. Voriconazole and Amphotericin B are the first line drugs of choice, and surgery for source control is essential for better outcomes [4,6]. Patients often require prolonged or even lifelong antifungal therapy due to high risk of recurrence.
This is the first reported case involving long-term patient survival after removal of highly invasive aspergilloma with valve and myocardial involvement [7]. The technique of intraoperative amphotericin B washing following surgical aspergilloma removal and heart reconstruction in conjunction with post-operative antifungal therapy may be a novel approach to treating cardiac aspergilloma. This case also supports the observation that an immunocompromised state (i.e., chemotherapy-induced neutropenia) is a strong risk factor for cardiac aspergilloma. While the exact mode of infection in this patient is unknown, immunocompromise (neutropenia) and venous catheterization for chemotherapy access likely contributed to susceptibility to infection.
Conflicts of Interest
None.
References
- Pierrotti LC, Baddour LM (2022) Fungal endocarditis, 1995-2000. Chest 122: 302-310.
- Navabi MA, Ajami H, Amirghofran A, et al. (1998) Aspergillus endocarditis: Rare but serious Aspergillus ball obstructing the pulmonary artery. Eur J Cardio-Thoracic Surg 14: 530-532.
- Shoar MG, Zomorodian K, Saadat F, et al. (2004) Fatal endocarditis due to Aspergillus flavus in Iran. J Pak Med Assoc 54: 485-486.
- El-Hamamsy I, Durrleman N, Stevens LM, et al. (2005) Aspergillus endocarditis after cardiac surgery. Ann Thorac Surg 80: 359-364.
- Challa S, Prayaga AK, Vemu L, et al. (2004) Fungal endocarditis: An autopsy study. Asian Cardiovasc Thorac Ann 12: 95-98.
- Patterson TF, Thompson GR, Denning DW, et al. (2016) Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases society of America. Clin Infect Dis 63: e1-e60.
- Singla MK, Shrivastava A, Mukherjee KC, et al. (2011) Potentially fatal tricuspid valve aspergilloma detected after laparoscopic abdominal surgery. South African J Anaesth Analg 17: 266-268.
- Riviere S, Lortholary O, Michon J, et al. (2013) Aspergillus endocarditis in the era of new antifungals: Major role for antigen detection. J Infect 67: 85-88.
Corresponding Author
Zechariah C Harris, BS, Wake Forest School of Medicine, Wake Forest Baptist Medical Center, 1 Medical Center Blvd, Winston-Salem, NC, 27103, USA, Tel: 912-231-5844
Copyright
© 2022 Harris ZC, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.