Comparative study of earlier EuroSCORE and EuroSCORE II among CABG patients-A cohort Study in Bangladeshi population
Abstract
Objective
The European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) is an updated version of the original EuroSCORE. The goal of this analysis was to compare EuroSCORE II and additive and logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) in predicting early mortality after coronary artery bypass surgery in a single center of Bangladesh.
Methods
A prospective consecutive series of 400 adults who underwent coronary artery bypass surgery between January 2014 and December 2016 was studied in National Heart Foundation Hospital & Research Institute. The newly developed EuroSCORE II was applied in this sample and compared to the additive and logistic version of the models. Validity was assessed on the basis of its calibration (using the Hosmer-Lemeshow test) and its discrimination using the receiver operating characteristic curve (ROC) and the association between observed and predicted mortality were performed using the one proportion Z test.
Results
The Hosmer-Lemeshow test showed that the model calibration was satisfactory (p = 0.738 in EuroSCORE II, p = 0.114 in additive method and p = 0.645 in logistic method), and area under ROC curve 0.972 in EuroSCORE II, 0.903 in additive model and 0.915 in logistic model. Hospital overall observed early mortality was 1.25%. EuroSCORE II predicted mortality 1.3% [95% confidence interval (CI) 0.49-3.10] having p value 0.860, additive EuroSCORE predicted mortality is 4.3% [95% confidence interval (CI) 2.53-6.78], having p value 0.001, and mortality prediction my logistic EuroSCORE 2.2% [95% confidence interval (CI) 1.00-4.16], having p value 0.112.
Conclusion
EuroSCORE II is better calibrated than the previous model. Mortality prediction by the EuroSCORE II is not very different from observed early mortality in CABG patients in National Heart Foundation Hospital and Research Institute.
Keywords
Coronary artery bypass grafting, Early Mortality, EuroSCORE, Risk assessment
Introduction
The European System for Cardiac Operative Risk Evaluation (EuroSCORE) is a risk-stratified scoring scheme which is applied to assess mortality and morbidity. Between 1995 and 1999 the EuroSCORE model was originally developed for measuring the bedside operation risk as an additive model (additive EuroSCORE, AES) [1]. Then logistic EuroSCORE (LES) was launched in 2003 [2] to gain predictive performance in a high-risk group. Since then the EuroSCORE has become a standard cardiac surgery risk prediction tool used worldwide. Over the last few years, several professionals from many parts of the world have reported that the model now overpredicts the risk [3], as the result of cardiac surgery have improved significantly.
In 2011 EACTS (European Association for Cardiothoracic Surgery) meeting in Lisbon, an upgraded version of this model named EuroSCORE II has been proposed. It used to be based on the data on 22381 consecutive patients undergoing major cardiac surgery. This new EuroSCORE II model discovered better calibrated than the previous EuroSCORE in detecting hospital mortality preserving high discrimination. It has demonstrated a discriminative capability identical to EuroSCORE (AUC EuroSCORE II = 0.81 vs. AUC EuroSCORE = 0.78), and precise calibration (Hosmer-Lemeshow chi-squared test, x2HL two [EuroSCORE II] = 15.48; P = 0.0505) [4] consequently it is validated that EuroSCORE II is higher tool than the original AES and LES.
Previously a study was done to evaluate the performance of former EuroSCORE model among coronary artery bypass grafting (CABG) patients [5], although EuroSCORE II has never been applied in this group. Our aim is to assess the performance of this EuroSCORE II model among patients who had undergone Coronary artery bypass grafting and to compare its predictive performance with additive EuroSCORE (AES) and logistic EuroSCORE (LES) in terms of calibration and discrimination.
Methods
Patients
Between July 2014 to June 2016 400 patients admitted for elective CABG. A prospective cohort study was performed. Patients undergoing surgical ventricular restoration procedure and Acute Aortic dissection were excluded from this study. All patients had received general anesthesia before surgery, a conventional median sternotomy was used to open the chest. Patients were discharged at 7th post-operative day routinely unless otherwise any of them complicated by other factors. Those patients were successfully discharge was contacted via mobile phone at the 31st postoperative day whether any mortality event occurred and recorded accordingly. Those were complicated by other factors and had prolonged hospital stay they were followed till their discharge or any mortality event and recorded accordingly.
Data collection procedure
Data were collected using a preformed data collection sheet (questionnaire). Baseline information was collected from the patient after exploration of different complaints, sign, and symptoms. All information regarding clinical features and microbiological results were recorded in a data collection sheet. Data were collected by the researcher himself. Data acquisition was performed by using EuroSCORE II and original EuroSCORE data sheet from patients file and later compiled in the online calculator present in this site http://www.euroscore.org/calc.html.
Data processing and analysis
Data had been compiled into the computer on a master folder first. Then, Data was analyzed via computer software Statistical Packages for Social Scientist (SPSS) model 16 The effects were presented in tables. Continuous variables had been expressed as mean ± standard deviation, and discrete variables have been summarized by using percentages. The cohort was once grouped into the low, medium and high chance team in accordance with EuroSCORE II, additive and logistic model of EuroSCORE model. The validity of the model was analyzed by using its calibration (statistical precession) with Hosmer-Lemeshow (H-L) check and discriminatory capability (statistical capacity) with the ROC curve. The association between determined and envisioned mortality was assessed by immediately evaluating the found and predicted mortality figure with a 95% confidence interval using One proportion Z test, a P value less than 0.05 considered significant.
Results
As show on Table 1, the mean age of our sample was 53.95 ± 8.08. Majority of our patients were male 82.5% (330 out of 400), and female were 17.5% (70 out of 400) Study population was grouped into three categories (Table 2, Table 3 and Table 4), in EuroSCORE II 76% patient falls into low risk, 21.8% in moderate risk and 2.2% of the study population fall into a high-risk group. In additive EuroSCORE 59.5% patient in this study group is in low-risk category followed by moderate risk of 35.5% and only 5.5% patient fall into high risk. Whereas in logistic EuroSCORE 58.2% patient in this study group is in low-risk category followed by moderate risk 35% and only 6.8% patient fall into high risk.
Calibration of these models are shown (Table 5, Table 6 and Table 7), C statistic obtained with the Hosmer-Lemeshow test was p = 0.738 in EuroSCORE II , p = 0.114 in additive method and p = 0.645 in logistic method and were not significant in different risk groups of NHF sample and p value remains > 0.05 in all subgroups which indicates risk factors used in the EuroSCORE model could predict the operative mortality satisfactorily for patients undergoing coronary surgery in our center.
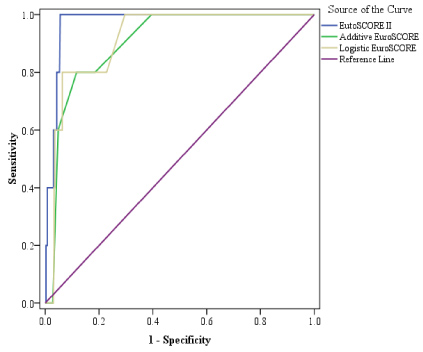
The area under the ROC curve was 0.8905 in the original EuroSCORE II data set [4]. In this study, the model's discriminatory power also good and useful, as indicated by an area under ROC curve of 0.972 in EuroSCORE II model, 0.903 in additive method and 0.915 in logistic method that means EuroSCORE II method can predict the outcome with 97% accuracy, additive method with 90% accuracy and the logistic method does that with 91% accuracy. It signifies that the EuroSCORE II model has better discriminatory power than the additive and logistic version of EuroSCORE. The ROC curve of the entire cohort given in Figure 1.
The overall mortality in our setting was 1.25% (5 out of 400). Table 8 is showing the association between predicted and early mortality. The EuroSCORE II predicted mortality was 1.3% [95% confidence interval (CI) 0.49-3.10], 4.3% [95% confidence interval (CI) 2.53-6.78] by the additive method and by the logistic EuroSCORE 2.2% [95% confidence interval (CI) 1.00-4.16].
One proportion Z test was done to measure the level of significance. The performance of the model was assessed by comparing the observed and predicted mortality figures with 95% confidence intervals. The observed early mortality in three different risk groups was compared by univariate analysis with predicted mortality by EuroSCORE II, additive and logistic method of EuroSCORE. The p value was 0.860 in EuroSCORE II 1, 0.001 in additive method and 0.112 in the logistic method that means both EuroSCORE II predicted mortality and mortality predicted by logistic EuroSCORE is as similar to observed early mortality for CABG patients in NHFH.
By this present study, we can conclude that the EuroSCORE II model has been validated for use in this center and that it has proven to be a reliable instrument for risk stratification. This signifies that the model's predictions of the probability of dying are valid and appropriately risk-adjusted for patients undergoing coronary artery surgery in NHFH.
Discussion
In recent years the EuroSCORE has become one of the most widely used prognostic scoring systems. Among the different studies to stratify the risk, the EuroSCORE has proved to be accurate, even when applied to non-European populations [6].
National Heart Foundation Hospital (NHFH) & Research Institute is a reference center for this type of heart surgery and performs a large number of coronary surgeries every year. Before using a probabilistic model in a context other than upon which it was created should be validated otherwise it may produce erroneous probabilities. As such EuroSCORE was inappropriate for risk prediction in Australia [7].
In this study group distribution of early mortality in EuroSCORE II Mean ± SD (5.19 ± 2.12), Mann-Whitney U test to measure the level of significance showed p value of 0.001 (considered significant), whereas distribution of additive EuroSCORE (5.20 ± 1.30) with p value 0.002 (considered significant); distribution of logistic EuroSCORE (5.39 ± 1.79) with p value 0.001 (considered significant).
In this study, the C statistic obtained with the Hosmer-Lemeshow test was p = 0.738 in EuroSCORE II , p = 0.114 in additive method and p = 0.645 in logistic method and were not significant in different risk groups of NHF sample and p value remains > 0.05 in all subgroups which indicates risk factors used in the EuroSCORE model could predict the operative mortality satisfactorily for patients undergoing coronary surgery in our center.
The area under the ROC curve was 0.8905 in the original EuroSCORE II data set [4]. In this study, the model's discriminatory power also good and useful, as indicated by an area under ROC curve of 0.972 in EuroSCORE II model, 0.903 in additive method and 0.915 in logistic method that means EuroSCORE II method can predict the outcome with 97% accuracy, additive method with 90% accuracy and the logistic method does that with 91% accuracy. It signifies that the EuroSCORE II model has better discriminatory power than the additive and logistic version of EuroSCORE.
The overall mortality in our setting was 1.25% (5 out of 400) and the predicted mortality was 1.3% [95% confidence interval (CI) 0.49-3.10] by the EuroSCORE II, 4.3% [95% confidence interval (CI) 2.53-6.78] by the additive method and 2.2% [95% confidence interval (CI) 1.00-4.16] by the logistic EuroSCORE.
The observed early mortality in three different risk groups was compared by univariate analysis with predicted mortality by EuroSCORE II, additive and logistic method of EuroSCORE. The p value was 0.860 in EuroSCORE II 1, 0.001 in additive method and 0.112 in the logistic method that means both EuroSCORE II predicted mortality and mortality predicted by logistic EuroSCORE is as similar to observed early mortality for CABG patients in NHFH.
Conclusion
The effects of this study enable us to conclude that despite substantial demographic and epidemiological differences between Bangladesh and European population, EuroSCORE II used to be validated and carried out nicely on NHFH patients and could be recommended as a risk stratification system to estimate the chance of early mortality in patients scheduled for coronary artery bypass grafting in Bangladesh. This study demonstrates that the EuroSCORE II is more accurate in predicting operative mortality than the additive EuroSCORE (AES) and logistic EuroSCORE (LES) in patients undergoing coronary artery bypass grafting patients. This analysis was done in a single center of Bangladesh, and it represents only a fraction of patient undergoing Coronary Artery Bypass Grafting. The focus of this analysis was adult patients undergoing CABG and/or valve surgery, the identified independent risk factors may not be applicable to other surgeries such as aortic surgery, congenital heart surgical procedure or cardiac transplantation.
Table 1 shows that majority of patients were within 5th decade, lowest age in this study was 29-years and no patient found above 72-years. Mean age 53.95 ± 8.08.
Table 2 state that 76% patient in this study group is in low risk category followed by moderate risk 21.8% and only 2.2% patient fall into high risk.
Table 3 state that 59.5% patient in this study group is in low risk category followed by moderate risk 35.5% and only 5.5% patient fall into high risk.
Table 4 state that 58.2% patient in this study group is in low risk category followed by moderate risk 35% and only 6.8% patient fall into high risk.
Table 5 shows no significant association between EuroSCORE II predicted mortality and observed early mortality. Therefore, all risk factors taken into considerations in the EuroSCORE II model can accurately predict early mortality on NHF cohort.
Table 6 shows no significant association between Additive EuroSCORE predicted mortality and observed early mortality. Therefore, all risk factors taken into considerations in this model can accurately predict early mortality on NHF cohort.
Table 7 shows no significant association between the logistic EuroSCORE predicted mortality and observed early mortality. Therefore, all risk factors taken into considerations in the logistic EuroSCORE model can accurately predict early mortality on NHF cohort.
The performance of the model was assessed by comparing the observed and predicted mortality figures with 95% confidence intervals.
Table 8 shows no significant association between observed early mortality and predicted by EuroSCORE II and logistic EuroSCORE, whereas significant association found between mortality predicted by the Additive EuroSCORE and observed early mortality.
EuroSCORE II bears Area under the Receiver Operating Characteristic (ROC) curve 0.972, which means it can predict mortality with 97% accuracy, whereas AUC of ROC curve of additive EuroSCORE and logistic EuroSCORE was 0.903 and 0.915 respectively.
Funding
Department of Cardiothoracic surgery, National Heart Foundation Hospital & Research Institute.
Conflict of Interest
None declared.
Ethical Issues
Keeping compliance with Helsinki Declaration of Medical Research Involving Human Subjects 1964, all patients were informed verbally about the study design, the purpose of the study. Participants had the right to withdraw themselves from the project, at any time, for any reasons. Written informed consent was taken from the respondents. No data were disclose without the permission of the respondents no forceful attempt was taken to interview of any unwilling respondent Permission was taken from the academic and institutional ethical and review board (IRB) of National Heart Foundation Hospital and Research Institute for conducting this study. Permission of the study was taken from the concerned departments of the institute.
Contribution Statement
Conception and design of the research
Dr. Mauin Uddin,
Dr. Mohammad Ziaur Rahman
Dr. Prasanta Kumar Chanda.
Collection of the data
Dr. Mauin Uddin
Dr. Sumsul Arif Mohammad Musa.
Analysis and interpretation of the data
Dr. Mauin Uddin
Dr. Rubana Forhad.
Statistical analysis
Dr. Rubana Forhad
Dr. Mohammad Mostafizur Rahman
Dr. Sumsul Arif Mohammad Musa.
Drafting the manuscript
Dr. Mauin Uddin
Dr. Mohammad Mostafizur Rahman
Dr. Sumsul Arif Mohammad Musa.
Critical revision of the manuscript
Dr. Mauin Uddin
Dr. Mohammad Mostafizur Rahman.
Final approval of the manuscript
Dr. Mohammad Ziaur Rahman
Dr. Prasanta Kumar Chanda.
Obtained funding
Dr. Prasanta Kumar Chanda
Dr. Farooque Ahmed.
Overall responsibility
Dr. Mohammad Ziaur Rahman
Dr. Prasanta Kumar Chanda
Dr. Farooque Ahmed.
Declaration
I there by humbly declared that this thesis entitled “Comparative study of earlier EuroSCORE and EuroSCORE II for among CABG patients-A cohort Study in Bangladesh population” is based on the work carried out by me in the Department of Cardiac Surgery in National Heart Foundation Hospital and Research Institute (NHFH & RI), Dhaka, Bangladesh during the period of July 2014 to June 2016. No part of this thesis has been presented previously for higher degrees or published in journals.
References
- Nashef SA, Roques F, Michel P, et al. (1999) European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg 16: 9-13.
- Roques F, Michel P, Goldstone AR, et al. (2003) The logistic EuroSCORE. Eur Heart J 24: 881-882.
- Mack MJ (2011) Risk scores for predicting outcomes in valvular heart disease how useful? Curr Cardiol Rep 13: 107-112.
- Nashef SA, Roques F, Sharples LD, et al. (2012) EuroSCORE II. Eur J Cardiothorac Surg 41: 734-744.
- Rahman MZ, Sayeed S, Choudhury SR, et al. (2012) Single centre performance of the EuroSCORE on a consecutive sample of Coronary Artery Bypass Surgery in a developing country. Journal of National Heart Foundation of Bangladesh 1: 58-61.
- Nashef SA, Roques F, Hammill BG, et al. (2002) Validation of European system for cardiac operative risk evaluation (EuroSCORE) in North American cardiac surgery. Eur J Cardiothorac Surg 22: 101-105.
- Yap CH, Reid C, Yii M, et al. (2006) Validation of the EuroSCORE model in Australia. Eur J Cardiothorac Surg 29: 441-446.
Corresponding Author
Mauin Uddin, Post graduate fellow, National Heart Foundation Hospital and Research Institute, Dhaka, Bangladesh, Tel: +8801747617997.
Copyright
© 2020 Uddin M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.