Hormone-Negative, Her2-Positive Male Breast Cancer with a Poor Prognosis: A Case Report
Abstract
We experienced a case of HER2-positive male breast cancer with a poor prognosis. A 64-year-old man visited our hospital due to general malaise, a left breast mass, and neck edema. The patient was diagnosed with HER2-positive breast cancer after needle histology. Weekly paclitaxel and trastuzumab therapy was started. However, the patient experienced lightheadedness and dizziness, and developed brain metastasis. After whole-brain irradiation, the condition worsened, and the patient died. HER2 type male breast cancer has a poor prognosis. There are many cases that are difficult to diagnose, but it is necessary to take immediate measures such as treatment decisions.
Keywords
Male breast cancer, HER2 type
Abbreviations
HER2: Human Epithelial Growth Factor Receptor Type 2; MBC: Male Breast Cancer; CT: Computer Tomography; FDG-PET: Fluorodeoxyglucose-Positron Emission Tomography; CEA: Carcinoembryonic Antigen; CA15-3: Cancer Antigen 15-3; BRCA: Breast Cancer Susceptibility Gene; PARP: Poly ADP-Ribose Polymerase
Introduction
Male breast cancer (MBC) is rare, accounting for 0.5-1.0% of all breast cancer cases, and is mostly hormone-dependent luminal type. The proportion of HER2 type of hormone-negative and HER2-positive cancer is extremely rare among patients with MBC (0.6-1.2%) and the prognosis is reportedly poor in many patients (1-4). We here in report our experience with a case of advanced hormone-negative, HER2-positive MBC.
Case
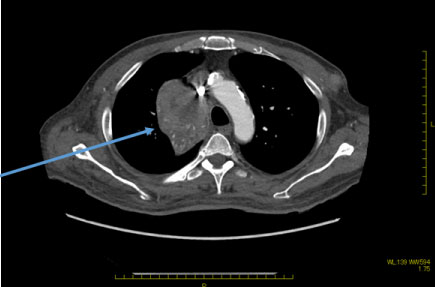
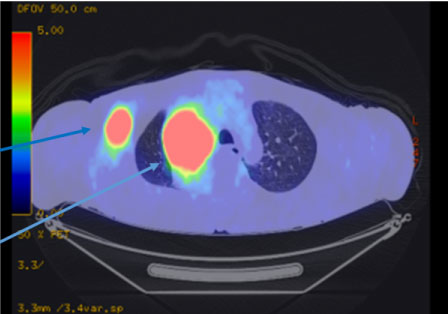
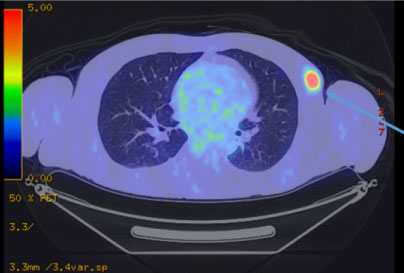
A 64-year-old man was referred from a local doctor for a left breast mass, left neck swelling and general malaise. The patient had a height of 162 cm and body weight of 64 kg. A mass with a size of 15 mm was observed in the left upper outer quadrant. Computed tomography (CT) revealed a mass with a size of 70 mm in the right thoracic cavity along with mediastinal lymph node (LN) enlargement, bilateral cervical LN enlargement, right axillary LN enlargement, and left breast mass (Figure 1 and Figure 2). Positron emission tomography with FDG showed accumulation of maximum standardized uptake value of 14 at sites consistent with the lesions on CT (Figure 3 and Figure 4). In the blood test, tumor markers were high (CEA, 22 ng/mL; CA 15-3, 125 U/mL). On the same day, after core needle biopsy, the patient was diagnosed with invasive ductal carcinoma (solid-tubular carcinoma; ER (-), PgR (-), HER2 (3+), nuclear grade III, ki-67 90% and T3N3M1 Stage IV). Although cerebellar metastasis was suspected on magnetic resonance imaging of the brain, we started weekly paclitaxel and trastuzumab therapy considering the possibility that treatment opportunity might be lost due to the worsened general condition. After completion of one cycle, dizziness and lightheadedness were reported. Thus, whole brain irradiation was performed with glycerol and steroid for the prevention of brain edema. However, the patient�s condition worsened, and he died approximately 3 months after the diagnosis.
Discussion
Male breast cancer is rare, accounting for 0.5-1.0% of all breast cancer cases, and is reportedly a hormone-dependent luminal type in many cases. The proportion of HER2 type with hormone-negative, HER2-positive MBC, as we presented herein, is as low as 0.6-1.2% among the rare MBC. It is sometimes detected in patients with advanced recurrent breast cancer, and their prognosis is often poor [1-4]. At our hospital, among 3,194 patients with breast cancer under treatment between 2000 and 2018, there were 14 (0.44%) cases of MBC. Of these male patients, 12 patients were hormone-dependent (ER and/or PgR positive) and HER2-negative. A total of 10 patients are still alive after 5 years of hormone therapy only (tamoxifen), and two patients (one with stage III b and the other with stage IV cancer at the initial visit) died after 1 year and 8 months and 5 years and 8 months, respectively. One patient was diagnosed with hormone-negative, HER2-positive breast cancer after visiting our hospital with the chief complaints of extensive progression of right precordial mass and lymphoedema of the upper limbs due to multiple enlarged LN. A partial remission has been maintained with anticancer drugs and anti-HER2 therapy, and treatment is still ongoing. Together with the present case, we had an impression that HER 2 type MBC was detected in the advanced state.
In general, the standard treatment for HER2-positive advanced recurrent breast cancer is the combination of anticancer therapy and anti-HER2 therapy. It has been also reported that treatment with paclitaxel and trastuzumab was effective in patients with MBC [5]. Since general malaise and edema, seemingly caused by cancerous cachexia, were observed in the patient, we initiated drug therapy. However, brain metastasis was suspected at the initial visit, and considering the progress status, it was difficult to determine the treatment policy. The usefulness of pertuzumab, trastuzumab and docetaxel for advanced recurrent HER2 type breast cancer has been reported [6]. However, docetaxel requires careful administration and attention in patients with edema or pleural effusion, and its use is often difficult. Since there are few reports of HER2-positive MBC and no data support the difference in treatment between men and women, it was considered appropriate to refer to such clinical studies in the present case.
Furthermore, genetic breast cancer accounts for 5-10% of breast cancer, and the proportion of BRCA mutation-positivity is reportedly higher in MBC than in female breast cancer [7,8]. BRCA mutation-positive patients are generally HER2 negative. It is believed that both HER2 loci are missing because they are close to the BRCA-1 gene. However, 8-10% of patients are reported to be HER2-positive [9]. Unlike anticancer drugs, PARP inhibitors [10], which can be currently used for patients with BRCA mutation-positive advanced cases, are relatively easy to use even in poor general condition. If there are not many alternative drugs to be used like in the present case, BRCA mutation testing could have been an option for us to consider their use. In addition, in the future, exploration of treatment with gene panel tests [11] will be included as one of the study items.
Conclusion
HER2 type male breast cancer has a poor prognosis. There are many cases that are difficult to diagnose, but it is necessary to take immediate measures such as treatment decisions.
Declarations
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Ethics approval and consent to participate
All procedures used in this research were approved by the Ethics Committee of Asahikawa Medical University.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent form is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Authors contribution
MK have operated this case and analyzed all data. SY, MA, NY, SO, KI did the assistant of chemotherapy.
All authors read and approved the final manuscript.
Acknowledgements
The authors declare that they have no competing interests.
References
- Leone JP, Leone J, Zwenger AO, et al. (2015) Prognostic significance of tumor subtypes in male breast cancer: A population-based study. Breast Cancer Res Treat 152: 601-609.
- Masci G, Caruso M, Caruso F, et al. (2015) Clinicopathological and immunohistochemical characteristics in male breast cancer: A retrospective case series. Oncologist 20: 586-592.
- Chavez-Macgregor M, Clarke CA, Lichtensztajn D, et al. (2013) Male breast cancer according to tumor subtype and race: A population-based study. Cancer 119: 1611-1617.
- Abreu MH, Afonso N, Abreu PH, et al. (2016) Male breast cancer: Looking for better prognostic subgroups. Breast 26: 18-24.
- Hayashi H, Kimura M, Yoshimoto N, et al. (2009) A case of HER2-positive male breast cancer with lung metastases showing a good response to trastuzumab and paclitaxel treatment. Breast Cancer 16: 136-140.
- Baselga J, Cortés J, Kim SB, et al. (2012) Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med 366: 109-119.
- Kwiatkowska E, Teresiak M, Filas V, et al. (2003) BRCA2 mutations and androgen receptor expression as independent predictors of outcome of male breast cancer patients. Clin Cancer Res 9: 4452-4459.
- Hesse-Biber S, An C (2017) With in-gender differences in medical decision making among male carriers of the BRCA genetic mutation for hereditary breast cancer. Am J Mens Health 11: 1444-1459.
- Vaziri SA, Krumroy LM, Elson P, et al. (2001) Breast tumor immunophenotype of BRCA1-mutation carriers is influenced by age at diagnosis. Clin Cancer Res 7: 1937-1945.
- Tutt A, Robson M, Garber JE, et al. (2010) Oral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and advanced breast cancer: A proof-of-concept trial. Lancet 376: 235-244.
- Zehir A, Benayed R, Shah RH, et al. (2017) Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat Med 23: 703-713.
Corresponding Author
Masahiro Kitada, Department of Breast Disease Center, Asahikawa Medical University, Midorigaoka-Higashi 2-1-1-1, Asahikawa Hokkaido 078-8510, Japan, Tel: +81-166-68-2494, Fax: +81-166-68-2499.
Copyright
© 2019 Kitada M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.